
Authors: Simon Sarkisian, DO (EM Attending, Cooper University Hospital/US Army, Camden, NJ) and Zachary Sletten, MD (EM Attending, Brooke Army Medical Center) // Reviewed by: Alexander Y. Sheng, MD, MHPE (@theshenger); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
You are a busy emergency medicine (EM) attending physician, and you hear about a facial laceration that just checked in. The intern asks you for help repairing the laceration, and you eagerly accompany them into the room excited to endow them with your wisdom on laceration repair. After stepping into the room, you realize you might be in over your head (no pun intended). This is not your run of the mill facial laceration.
The series will review the repair of head, eyes, ears, nose, and throat (HEENT) lacerations, with a focus on the areas where emergency physicians tend to struggle. Today we look at oral mucosa lacerations.
Case
A 10-year-old boy was swinging on the monkey bars at the playground when he slipped and fell landing face down on the wooden platform. In your ED, he has a 3 cm deep laceration to his right outer cheek. When you look inside the mouth you also notice that the external laceration has gone through all the layers to a 2.5 cm internal laceration.
Oral Mucosa Lacerations
As a rule of thumb, most lacerations involving the oral mucosa heal on their own without intervention. However, primary closure is preferred for intraoral lesions where6:
- The wound is deep enough to trap food particles
- The wound is > 2cm in length
- Wounds with a flap of tissue between the occlusal (chewing) aspects of the teeth. Small flaps can be excised.
Don’t miss the forest for the teeth. All patients with intraoral lacerations should have an evaluation of their face for dental trauma, midface fractures, and jaw fractures. Evaluate all lacerations that penetrate the oral mucosa for the presence of tooth fragments, especially if teeth are missing or chipped. Intensify the search if the patient returns with an infection of a sutured wound. Probe the wound with forceps to identify fragments not seen directly in the wound. In the setting of marked facial swelling, take an X-ray of the soft tissue to help identify embedded tooth fragments7.
For closure of oral mucosa lacerations, absorbable 4-0 or 5-0 simple interrupted sutures is the standard. Vicryl is preferred since it is soft, promotes less inflammation, resists breakdown by saliva, and is less abrasive than gut sutures, which become hard and traumatize adjacent mucosa7. In general, when possible, close muscle and mucosal layers separately. Sutures in the oral cavity easily become untied by the constant motion of the tongue. Tie each of these sutures with at least four square knots.
Through-and-through lacerations of the mouth should be closed in layers, beginning with the intraoral mucosa and working outward in layers toward the skin. Contamination can be considerable so thoroughly irrigate once nonviable tissue and foreign bodies are removed. After closure of the mucosal layer, copious irrigation of the external wound is indicated to remove lingering bacteria that otherwise would be incorporated into the wound.
The evidence on the use of prophylactic antibiotics is limited. In a small study involving 62 patients, prophylactic treatment with penicillin was associated with a decreased risk of infection after significant through-and-through lacerations8,9. This was further supported by retrospective study that also observed benefit to antibiotics. However, the benefit was only statistically significant in immunocompromised patients10.
Lacerations that approach the parotid (Stensen’s) or submandibular (Wharton’s) duct should be evaluated before intervention for ductal integrity (see Figure 1 and 2).


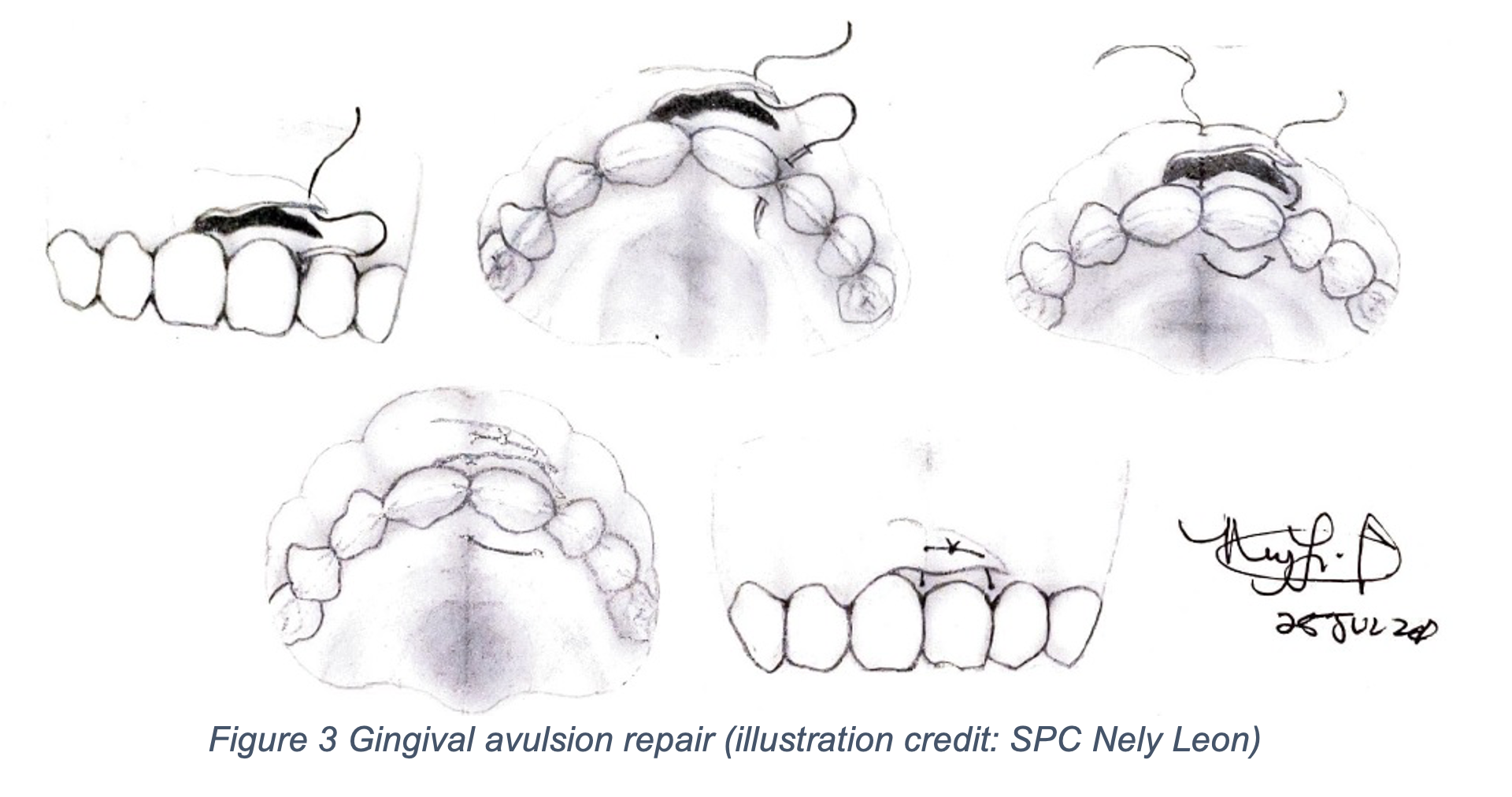
When glandular parotid tissue is involved in a wound, a clear fluid discharge can be seen. To test for ductal integrity, the inside of the buccal surface is dried, then the parotid is pressed. Saliva will appear at the duct’s opening, if it is intact. A laceration over the gland itself (with an intact duct) is repaired by simply closing the skin over the gland. If a duct is involved or there is any doubt, ENT or oral surgery should be consulted to stent the duct open and preserve its function6,9,11. Laceration of the maxillary labial frenulum does not require repair. Because of the vascularity, the lingual frenulum of the tongue may need repair. An absorbable 4-0 is appropriate1. For gingival avulsions, there is a limited amount of submucosa to anchor the stitch so use the mucosa on the inner side of the teeth as described below and depicted in Figure 3 below.
1) Pass the needle and 4-0 or 5-0 absorbable suture through the tip of the flap and between the teeth to the palatal portion of the gums. If the teeth are too close together to permit passage of the needle, floss the suture between the teeth and then take a bite through the palatal portion of the gums.
2) Pass the needle circumferentially around the tooth so that it comes out through the flap on the facial portion of the gums and tie. If the teeth are too close to permit passage of the needle, floss the suture between the teeth to the facial portion of the gums and then take a bite of tissue and tie.
3) Repeat as needed until the flap is approximated.
4) For edentulous patients be sure that the suture knots and loops are not located in regions of contact with the bridge of the denture6.
In terms of discharge instructions after repair, patients should be on a soft diet for two to three days and rinse their mouth with water after eating. Avoid spicy or salty foods until the wound is healed. Avoid the use of straws (negative pressure may increase ecchymosis or bleeding at the wound site). Wounds should heal rapidly (within three to five days). Patients with risk factors for infection (eg, diabetes mellitus, immunocompromised) should undergo reevaluation 48 to 72 hours after repair to ensure proper healing12. Whether or not any intraoral laceration is repaired, discharge the patient with chlorhexidine 0.12% oral rinse, 15 mL, swish and spit for 30 seconds every 12 hours9.
Stay tuned for our next piece in the series on repair of lip lacerations.
References/Further Reading
- Tintinalli JE, Ma OJ, Yealy DM, et al. Tintinalli’s emergency medicine: a comprehensive study guide. 2020.
- Hollander JE, Richman PB, Werblud M, Miller T, Huggler J, Singer AJ. Irrigation in facial and scalp lacerations: does it alter outcome? Ann Emerg Med 1998;31:73-7.
- Singer AJ, Gulla J, Hein M, Marchini S, Chale S, Arora BP. Single-layer versus double-layer closure of facial lacerations: a randomized controlled trial. Plast Reconstr Surg 2005;116:363-8; discussion 9-70.
- Farion KJ, Russell KF, Osmond MH, et al. Tissue adhesives for traumatic lacerations in children and adults. Cochrane Database of Systematic Reviews 2002.
- Holger JS, Wandersee SC, Hale DB. Cosmetic outcomes of facial lacerations repaired with tissue-adhesive, absorbable, and nonabsorbable sutures. Am J Emerg Med 2004;22:254-7.
- Armstrong BD. Lacerations of the mouth. Emerg Med Clin North Am 2000;18:471-80, vi.
- Roberts JR, Custalow CB. Roberts and Hedges’ clinical procedures in emergency medicine and acute care. 2019.
- Steele MT, Sainsbury CR, Robinson WA, Salomone JA, 3rd, Elenbaas RM. Prophylactic penicillin for intraoral wounds. Ann Emerg Med 1989;18:847-52.
- Walls RM, Hockberger RS, Gausche-Hill M. Rosen’s emergency medicine: concepts and clinical practice2018.
- Katsetos SL, Nagurka R, Caffrey J, Keller SE, Murano T. Antibiotic prophylaxis for oral lacerations: our emergency department’s experience. Int J Emerg Med 2016;9:24.
- Wedmore I. Wound Care: Modern Evidence In The Treatment Of Man’s Age-Old Injuries. Emergency Medicine Practice 2005;7.
- Assessment and Management of Intra-Oral Lacerations. 2020. (Accessed 25 JUL, 2020, at https://www.uptodate.com/contents/assessment-and-management-of-intra-oral-lacerations?search=Assessment%20and%20Management%20of%20Intraoral%20Lacerations&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1.)




