Authors: Anita Bhamidipati, MD (Attending Physician – Virtua Memorial Hospital, Mt Holly, NJ, Volunteer Faculty in Emergency Medicine, Cooper University Medical School); Sumaya Mekkaoui, MD (Attending Physician at Crozer Health, Upland, PA, Assistant Professor of Emergency Medicine, Assistant director of medical student education, Drexel University College of Medicine) // Reviewed by: Courtney Cassella, MD (EM Attending Physician, Reading Hospital Tower Health, PA); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case #1
An 80-year-old male with past medical history congestive heart failure (CHF), atrial flutter on aspirin, hypertension, type 2 diabetes, stroke with residual expressive aphasia presents with shortness of breath. He has been having shortness of breath for the past 1 week with associated lower extremity edema and fatigue. He notes dyspnea on exertion but denies chest pain. Prior to arrival he felt lightheaded and had an unwitnessed syncopal episode. He denies cough, fevers, leg pain, history of deep vein thrombosis (DVT) or pulmonary embolism (PE). When EMS arrived, his initial BP was 70/40. In the ED, the patient arrives awake and alert. His vitals were HR 170 BP 80/50 RR 18 T 98.9 02 95% on RA. Physical exam was significant for bilateral rales, mild tachypnea, an irregularly irregular rhythm, and bilateral lower extremity pitting edema. He was given a small fluid bolus and his BP responded; he was started on diltiazem for rate control of rapid atrial fibrillation found on his EKG below.
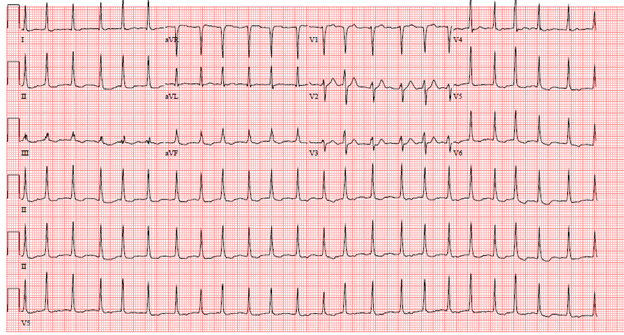
His chest x-ray was significant for pulmonary edema. Labs showed BNP > 25K, mildly elevated troponin and he subsequently was admitted to the hospital for a CHF exacerbation and rapid atrial fibrillation on a diltiazem and heparin infusion. His blood pressure improved as his heart rate was controlled. While upstairs, the admitting team ordered a d-dimer that was 21,000 ng/ml, the patient underwent CTA that showed large PE with RV strain pattern. He again became hypotensive and underwent fibrinolytic therapy while admitted.
Case #2
A 61-year-old female with past medical history of poorly-controlled diabetes, hypertension, hypothyroidism, multivessel coronary artery disease status post stent presents via EMS with chief complaint of generalized weakness, fatigue, malaise and nausea for the past few days. She reports “dizziness” and shortness of breath on exertion with minimal activity such as walking around her home. She denies any syncopal episodes, chest pain, abdominal pain, fever, cough, calf pain or swelling, prior DVT or PE, known malignancy, surgeries within the past month, prolonged immobilization or exogenous estrogen use. On arrival, her vital signs were HR 91, BP 121/79, RR 15, T 95.5, 94% on RA. She was briefly placed on 2L NC for comfort with reported shortness of breath upon moving about the bed. EKG showed normal sinus rhythm with T wave inversions in V1 and V2, no ST-segment deviation, old inferior Q-waves noted. Labs were notable for an elevated troponin at 1.0, BNP 154, lactate of 2.5, and a creatinine of 1.9. Bedside echo demonstrated increased RV:LV ratio, with septal bowing and TAPSE of 0.8 cm. No pericardial effusion was seen. Pt was started on heparin prior to CTA (which was delayed due to GFR). CTA ultimately revealed a large saddle embolus with extension to all lung fields. The patient was admitted to inpatient telemetry, where duplex of her left lower extremity revealed a DVT. She remained stable throughout her ED and hospital course and was discharged on Eliquis.
Introduction
Pulmonary embolism (PE) is one of the most common entities Emergency physicians evaluate. In the United States, the estimated incidence of PE is 100-200 cases per 100,000 people. The annual deaths currently attributed to PE have been estimated as 100,000/year in the United States [1]. Failure to recognize and treat PE can account for significant morbidity and mortality among patients.
Despite the frequency with which we encounter pulmonary emboli, it still plagues us as a missed diagnosis. We have no issue pinning this down on the patients who neatly fit into the “classic” case. The patient who is in the post-operative state, on OCPs and presents with pleuritic chest pain and hypoxia is not the diagnostic dilemma. More often the challenge lies in the patient who has another etiology of his dyspnea or tachycardia that seems to be a reasonable alternative to PE; or those in whom the diagnosis of PE is not considered at all. With all the advances in emergency medicine, the diagnosis of this life threatening ailment remains a distinct and unique challenge for emergency providers.
Why does this matter?
So you don’t make the diagnosis of PE in your hemodynamically stable syncope or chest pain patient, what’s the big deal anyway? You admit them for their cardiac work up and someone else will catch it right? You didn’t discharge them so what’s the harm?
Delayed diagnosis = worse outcomes
In one prospective single center study, patients with a delayed diagnosis had a higher rate of in-hospital adverse events, equal or worse measures of PE severity, and higher rates of altered mental status while in the hospital [2].
Diagnostic Dilemmas
- Non-specific symptoms
- Patients don’t read the textbook. While it would be significantly easier if they did some casual browsing of Tintinalli prior to coming into the ED, this is rarely the case. Classic symptoms of pleuritic chest pain, acute onset of symptoms, hypoxia and leg swelling should prompt consideration of PE, however we must also investigate “vague” symptoms. In the PIOPED group, the most common presenting symptoms associated with PE are dyspnea either at rest or with exertion, followed by pleuritic chest pain, signs of DVT, and cough. Hemoptysis was present in only 13% of patients in this large prospective study. [3,4] Pleuritic chest pain and hemoptysis are generally signs of lung infarction, usually due to peripheral emboli. Hemoptysis occurs as a sequela of hemorrhage from the infarcted lung.
- We are classically taught that the onset of symptoms in PE is acute. But does acute mean seconds? Minutes? hours? Data from PIOPED 2 revealed that the onset of dyspnea was rapid, defined as seconds to minutes in 72% of patients with PE and no prior cardiopulmonary disease and 67% of all patients with PE. However, the onset was within hours in 87% of all patients with PE. [5]
- History is crucial and we need to be on the lookout for less common presentations including syncope, transient arrhythmias and fatigue, especially in the elderly. Elderly patients presented less frequently with dyspnea or tachypnea regardless of pre-existing cardiopulmonary disease [5]. Syncope has been found to be the initial symptom in only 5% or fewer cases; however, when present, it can be associated with a larger clot burden and a higher risk for hemodynamic compromise [6].
- Remember the physical exam?
- Some may say the art of physical examination has been lost recently due to the availability of CT imaging and ancillary testing. However, here we need to go back to basics. Tachypnea and tachycardia are the most common signs associated with pulmonary embolism at over 50% and 26% respectively in all patients with PE regardless of preexisting cardiopulmonary disease [5].
- Evidence of pulmonary hypertension on examination such as Jugular Venous Distension were also common at just under ¼ of all PE cases [5].
- The presence of dyspnea, tachypnea, tachycardia, JVD and certainly the combination of any of these should urge the emergency physician to consider PE.
- Anchoring bias:
- There is a tendency to attribute dyspnea and tachypnea to pre-existing conditions especially with our elderly patients with several comorbid conditions. Anchoring bias rings loud in these folks with underlying CHF or COPD whose dyspnea can be “easily” explained by an alternative diagnosis. We need to maintain an even higher clinical suspicion here as crackles and decreased breath sounds that are found in acute CHF exacerbations are the most common pulmonary findings seen in patients with new PE [5].
- In patients with acute COPD exacerbations with no clear trigger, such as acute respiratory illness, the prevalence of PE was 16.1%, and commonly, patients complained of pleuritic chest pain [7].
- One meta-analysis in CHEST found that 1 in 4 patients admitted for acute COPD exacerbations were found to have PE, though it should be mentioned that only 1 study included in the meta-analysis utilized a clinical decision rule (Geneva) to determine pre-test probability. Even in the low risk group, the prevalence of PE was 9%. [8]
- There is a tendency to attribute dyspnea and tachypnea to pre-existing conditions especially with our elderly patients with several comorbid conditions. Anchoring bias rings loud in these folks with underlying CHF or COPD whose dyspnea can be “easily” explained by an alternative diagnosis. We need to maintain an even higher clinical suspicion here as crackles and decreased breath sounds that are found in acute CHF exacerbations are the most common pulmonary findings seen in patients with new PE [5].
We think it is fair to say, it’s time to drop the anchor.
- Lack of classic risk factors: We are taught that assessing pre-test probability is critical to effective and efficient diagnosis of pulmonary embolism in the emergency department. As such, we have several decision making rules to help us with this including Geneva, Wells, Perc, etc. But more on those later. These rules focus on “classic” risk factors including recent immobilization or surgery, tachycardia, hemoptysis, active malignancy and the fan favorite “PE is the number 1 diagnosis.” While these decision rules are designed to help us risk stratify patients, it is critical to remember that they are designed to aid us and not replace clinical judgement. Furthermore, the lack of some of these risk factors, does not exclude PE especially in a patient with unexplained dyspnea. The number of idiopathic PE ranged from 26% to 47% in several separate studies [9,10].
- Lack of high enough clinical suspicion
- One of the biggest reasons PE is missed is failure to consider it as a diagnosis.
How do we improve?
- Appropriate use of risk stratification tools: PERC, WELLS’, Geneva, YEARS
- Remember they are tools, not “rules”. They do not supersede clinical judgement. They do not account for all historical features and are used as an adjunct to your clinical decisions when applied appropriately. Of note, this discussion does not include risk-stratification or evaluation of pregnant patients, which is an extensive topic, not addressed by these tools in isolation.
- Wells’ Score: Decision tool that risk stratifies patients into high, moderate or low-risk categories. Can alternatively be used to risk stratify into two-tiers of either high-risk or low-risk. Based on the score, you can then decide to either proceed with CTA or determine if the patient is appropriate for a d-dimer. If they are low-risk, you may also proceed to the PERC rule to help determine whether they warrant a d-dimer or can safely be excluded from having a PE without additional testing. [11]
- High Risk (37.5% incidence of PE): CTA (skip the d-dimer)
- Moderate Risk (16.2% incidence of PE): consider d-dimer or CTA
- Low Risk (<1.3% incidence of PE): consider d-dimer or application of PERC
OR
-
- High Risk (“PE likely”, 37.1% incidence): CTA
- Low Risk (“PE Unlikely”, 12.1% incidence): consider d-dimer or application of PERC
- The major caveat of this tool is that one of the elements of the scoring system is “PE is #1 diagnosis” which is weighted more heavily than other questions in the tool; thus, this tool like many others still relies on clinical gestalt to generate a score. Maintaining a high clinical suspicion is paramount.
- PERC Rule:
- This is a “rule-out” tool and is used to determine if low-risk patients need to get a d-dimer rather than jumping right to CTA, with the goal of reducing the number of CTAs being ordered. D-dimer has a high sensitivity and a low specificity, which is why it makes it a good “rule-out” tool. This is applied to patients in whom you’ve considered PE in the diagnosis, but you deem to be low-risk for PE (i.e. pre-test probability of <15%). If the patient screens negative (answer “no” to all of the questions in the rule), then they have been “ruled-out” for PE and do not require a d-dimer or CTA. In low-risk patients with a pre-test probability of PE <15%, who screen negative by the PERC rule, the post-test probability of a PE is <2% which is below the threshold of detection with imaging. If properly applied, the thought is that obtaining further testing for PE may pose greater harm than benefit to the patient. [12]
-
- While there may be practice variations in how clinicians decide to apply such decision tools, one thing to consider is that the Wells’ Score helps you determine if the patient is in the low risk category and even appropriate for application of PERC. Furthermore, PERC doesn’t include several pertinent common risk factors such as long-distance travel, prolonged immobilization, active cancer or treatment. Therefore it makes sense to first apply Wells’ and then, if low risk, proceed to PERC. Additionally, using Wells’ prior to PERC comes in hand to help you determine your pre-test probability as an alternative to your gestalt alone. If you are an experienced practitioner, it’s possible that you may rely on your gestalt alone to determine pre-test probability; however, applying Wells’ can ground this decision-making some and then you can proceed to PERC. [12]
- YEARS Algorithm:
- Another algorithm with two-tiered d-dimer threshold based on level of suspicion/pre-test probability for PE in order to reduce the high number of CTAs that are ordered.
- The criteria are:
- Clinical signs of DVT
- Hemoptysis
- PE most likely diagnosis
-
- 1 or more criteria present → d-dimer threshold of 500ng/ml
- 0 Years criteria → increased d-dimer threshold of 1000ng/ml
- This algorithm states even if high clinical suspicion for PE, can rule-out based on d-dimer <500 ng/mL. The study reported a 14% reduction in CTAs with application of their algorithm[13,14]. However, there were several limitations in the study, including clinicians being unblinded to d-dimer results prior to risk-stratifying patients.
- Maintaining a high clinical suspicion
- Consider the risk factors as discussed and adjuncts to history and physical exam as below. PE should always be considered in patients with chest pain, just as aortic dissection and acute coronary syndrome are considered. It may quickly be ruled-out during history, but it is necessary to maintain a high index of suspicion in patients who have unexplained dyspnea/ “breathlessness” and hypoxia, as dyspnea and fatigue are more commonly reported than chest pain. Additionally, the absence of significant findings on chest x-ray that can explain the breathlessness should prompt consideration of PE. Remember not all that wheezes is COPD/asthma, pulmonary embolism can commonly cause wheezing!
- Use of all the tools in the toolbox.
- Emergency medicine physicians are often looked at as the “jack of all trades.” However, it is impossible to be a MacGyver of sorts without using all the tools in our armamentarium.
- Bedside Ultrasound
- The scope and utility of bedside ultrasound in the ED is constantly expanding. When performed adequately, ultrasound can give us some clues to help with the diagnosis of elusive PEs.
-
- Most of the bedside echocardiographic findings used to aid in diagnosis of PE are aimed at looking for signs of RV dysfunction and thus, do not have much utility in finding subsegmental PE. But the former are the PE’s we really care about the most as these are the patients with higher mortality, length of stay and progression to pulmonary hypertension.
-
-
- McConnell’s sign: Akinesia of RV free wall with apical sparing on Apical 4 chamber view. Specificity of 94% and Sensitivity of 77% [16]. Originally thought to distinguish acute PE from chronic pulmonary hypertension however more recent data suggests this is not the case.
-
-
-
- “D sign”: Flattening of intraventricular septum on parasternal short axis view
-
-
-
- TAPSE: Tricuspid annular plane systolic excursion has been used by cardiologists to evaluate for right ventricular dysfunction. Performed on an apical 4 chamber view, this measures the movement of tricuspid annulus over a contraction. More on how to do this in separate post on TAPSE
- While TAPSE has a lower specificity for PE, it has a higher sensitivity than other signs such as McConnell’s (SN 72%, SP 66% using a cutoff of 2.0cm). It seems that this sign becomes more useful in the critically ill or hypotensive patient [17].
- TAPSE: Tricuspid annular plane systolic excursion has been used by cardiologists to evaluate for right ventricular dysfunction. Performed on an apical 4 chamber view, this measures the movement of tricuspid annulus over a contraction. More on how to do this in separate post on TAPSE
-
- Multi-organ US for PE: Consider the utility of multi-organ ultrasound in risk-stratifying patients in whom you are considering the diagnosis of PE. This may be helpful in patients with multiple differential considerations with delays in imaging, a crashing patient or someone you want to consider heparinizing before CT scan. A study published in CHEST in 2014 demonstrated increased accuracy of PE diagnosis with use of multi-organ POCUS [18]. In this study, patients with increased likelihood of PE based on risk stratification tools underwent POCUS of:
- Their study found multiorgan ultrasound to have a sensitivity of 90% (82.8-94.9) and specificity of 86.2% (81.3-90.3). Notable additional findings (from which unable to draw conclusions) were that none of the patients in the study with negative US and negative d-dimer were found to have a PE; 74.4% of patients with positive US were found to have a PE on CTA and alternative diagnoses were made on US such as pleural and pericardial effusions, interstitial edema, pneumonia, and dissection [18, 21]. Bottom-line, put that US probe to good use!
- ECG findings in PE
- ECG- the emergency physician’s best friend. This “quick and dirty” test can prove useful in the diagnosis of PE. Common findings that can increase your suspicion of PE are:
-
-
- Sinus Tachycardia
- T wave inversions anteriorly and inferiorly
- S1Q3T3
- Right axis deviation
- RBBB
- Dominant R wave in V1
- STE in V1
- Atrial tachyarrhythmias
- T wave inversions anteroinferiorly are the most specific ECG finding in PE. Interestingly, TWI in lead 3 and V1 were observed in only 1% of patients with ACS but 88% of patients with PE. This can be a useful distinguishing factor between the two conditions that often mimic each other, with a reported specificity of 88% for PE [22].
-
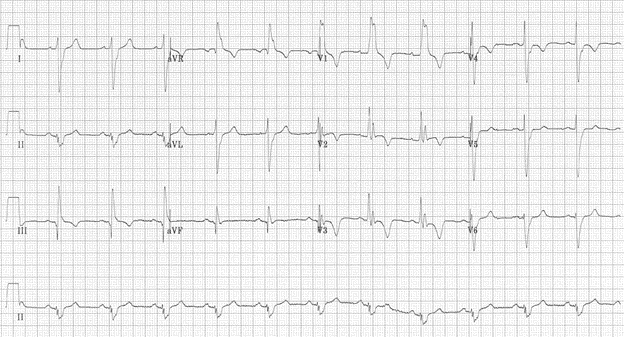
TWI seen in V1-V4, lead 3 + right axis deviation + s1q3t3 with bilateral PE [23]
Back to the Cases
#1: Bedside echo can provide a lot of pertinent diagnostic information especially in the unstable patient. While no single US finding is significantly specific or sensitive alone, when used in conjunction with history and other clinical data, can be critical in diagnosis. In this case, ultrasound very well could have shown a reduced TAPSE or septal flattening/D sign that would have led the clinician to consider CTA or D dimer sooner. We know that multiorgan ultrasound has higher sensitivity and specificity of single system US and should be undertaken when possible based on clinical suspicion.
Beware of any syncopal patient who is unstable! Even if “fluid responsive” you need to at least consider PE in your differential and keep a high index of suspicion.
Anchoring on CHF or alternate diagnoses can delay diagnosis of PE and lead to higher mortality and higher incidence of complications including pulmonary hypertension. A “new diagnosis” of CHF should always prompt consideration of why the patient suddenly developed this pathology. If secondary to a new or uncontrolled tachyarrhythmia, especially in the absence of clear anticoagulation, pulmonary embolism should come to mind.
#2: For this case, highest on the differential may be ACS given history of multivessel CAD in a poorly controlled diabetic with new TWIs, complicated by no prior cath report available to determine previous disease. Differential diagnosis also included infection- due to malaise fatigue (and only previous admission to this hospital were for sepsis and pericardial effusion (hypothyroidism not on her medication). While PE was initially considered, it was lower on the differential. It would have been easily to admit this patient for ACS or even sepsis with her complaints and an elevated troponin and lactate. With her low GFR, she may not have had a CTA performed at all if it were not for the astute ER physician who uses POCUS as an adjunct to his physical exam and who was able to make the diagnosis within minutes.
Take Home Points
- Patients may present with vague symptoms. The most common symptom of PE is dyspnea. This is more common than chest pain or hemoptysis. Pay attention to unexplained dyspnea or breathlessness.
- Delayed diagnosis leads to worse outcomes even in patients that are admitted to the hospital.
- Physical exam most commonly reveals tachypnea, followed by tachycardia. PE should also be on your differential when you note JVD, tachypnea and tachycardia on exam.
- POCUS is a great adjunct to the clinical exam and is helpful in determining if there are signs of right ventricular strain (RV-strain). POCUS can assist in making important decisions regarding diagnosis and treatment sometimes faster than CT scans. Use this to your advantage!
- Certain EKG findings may help you to consider the diagnosis in the right clinical context. The most common EKG finding in PE is tachycardia. The most specific EKG finding is anteroinferior TWIs. STE in V1, RBBB and right-axis deviation are among others.
- Clinical decision tools are just that: they are “tools,” not “rules” and should not replace clinical judgment. Do not anchor on a diagnosis. Rely on your clinical history and exam and use these as adjuncts.
References/Further Reading
- Giordano NJ, Jansson PS, Young MN, Hagan KA, Kabrhel C. Epidemiology, Pathophysiology, Stratification, and Natural History of Pulmonary Embolism. Tech Vasc Interv Radiol. 2017;20(3):135-140. doi:10.1053/j.tvir.2017.07.002
- Kline JA, Hernandez-Nino J, Jones AE, Rose GA, Norton HJ, Camargo CA Jr. Prospective study of the clinical features and outcomes of emergency department patients with delayed diagnosis of pulmonary embolism. Acad Emerg Med. 2007;14(7):592-598. doi:10.1197/j.aem.2007.03.1356
- PIOPED Investigators. Value of the ventilation/perfusion scan in acute pulmonary embolism. Results of the prospective investigation of pulmonary embolism diagnosis (PIOPED).JAMA. 1990; 263 (20): 2753-2759. https://www.ncbi.nlm.nih.gov/pubmed/2332918. doi:10.1001/jama.1990.03440200057023.
- Stein PD, Terrin ML, Hales CA, et al. Clinical, laboratory, roentgenographic, and electrocardiographic findings in patients with acute pulmonary embolism and no pre-existing cardiac or pulmonary disease. Chest. 1991;100(3):598-603. doi:10.1378/chest.100.3.598
- Stein PD, Beemath A, Matta F, et al. Clinical characteristics of patients with acute pulmonary embolism: data from PIOPED II. Am J Med. 2007;120(10):871-879.doi:10.1016/j.amjmed.2007.03.024
- Pollack CV, Schreiber D, Goldhaber SZ, Slattery D, Fanikos J, O’Neil BJ, Thompson JR, Hiestand B, Briese BA, Pendleton RC, Miller CD, Kline JA. Clinical characteristics, management, and outcomes of patients diagnosed with acute pulmonary embolism in the emergency department: initial report of EMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the Real World Registry). J Am Coll Cardiol. 2011 Feb 8;57(6):700-6. doi: 10.1016/j.jacc.2010.05.071. PMID: 21292129.
- Aleva FE, Voets LWLM, Simons SO, de Mast Q, van der Ven AJAM, Heijdra YF. Prevalence and Localization of Pulmonary Embolism in Unexplained Acute Exacerbations of COPD: A Systematic Review and Meta-analysis. Chest. 2017;151(3):544-554. doi:10.1016/j.chest.2016.07.034
- Rizkallah J, Man SFP, Sin DD. Prevalence of pulmonary embolism in acute exacerbations of COPD: a systematic review and metaanalysis. Chest. 2009;135(3):786-793. doi:10.1378/chest.08-1516
- Cushman M, Tsai AW, White RH, et al. Deep vein thrombosis and pulmonary embolism in two cohorts: the longitudinal investigation of thromboembolism etiology. Am J Med. 2004;117(1):19-25. doi:10.1016/j.amjmed.2004.01.018
- White RH. The epidemiology of venous thromboembolism. 2003;107(23 Suppl 1):I4-I8. doi:10.1161/01.CIR.0000078468.11849.66
- Wells PS, Anderson DR, Rodger M, Stiell I, Dreyer JF, Barnes D, Forgie M, Kovacs G, Ward J, Kovacs MJ. Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and d-dimer. Ann Intern Med. 2001 Jul 17;135(2):98-107. PubMed PMID: 11453709.
- Kline JA, et al. Clinical criteria to prevent unnecessary diagnostic testing in emergency department patients with suspected pulmonary embolism. J Thromb Haemost 2004; 2: 1247–55.
- Van der Hulle T, Cheung WY, Kooij S, et al. Simplified diagnostic management of suspected pulmonary embolism (the YEARS study): a prospective, multicentre, cohort study. Lancet. 2017;
- Kabrhel C, Van hylckama vlieg A, Muzikanski A, et al. Multicenter Evaluation of the YEARS Criteria in Emergency Department Patients Evaluated for Pulmonary Embolism. Acad Emerg Med. 2018;25(9):987-994.
- TPA. https://www.thepocusatlas.com/echocardiography/rv-thrombus-mcconnells-sign. Accessed April 22, 2021.
- McConnell MV, Solomon SD, Rayan ME, Come PC, Goldhaber SZ, Lee RT. Regional right ventricular dysfunction detected by echocardiography in acute pulmonary embolism. Am J Cardiol. 1996;78(4):469-473. doi:10.1016/s0002-9149(96)00339-6
- Daley J, Grotberg J, Pare J, et al. Emergency physician performed tricuspid annular plane systolic excursion in the evaluation of suspected pulmonary embolism. Am J Emerg Med. 2017;35(1):106-111. doi:10.1016/j.ajem.2016.10.018
- Nazerian P, Vanni S, Volpicelli G, et al. Accuracy of point-of-care multiorgan ultrasonography for the diagnosis of pulmonary embolism. Chest. 2014;145(5):950-957. doi:10.1378/chest.13-1087
- Avila, J. Pulmonary embolism (pulmonary findings). Core Ultrasound. Published on February 14, 2020. Accessed on April, 10, 2021. Available at https://www.coreultrasound.com/pulmonary-embolism-pulmonary-findings/.
- Avila, J. Pulmonary embolism (pulmonary findings). Core Ultrasound. Published on February 14, 2020. Accessed on April, 10, 2021. Available at https://www.coreultrasound.com/pulmonary-embolism-pulmonary-findings/.
- Prats, M. Multiorgan Ultrasound for Pulmonary Embolism. Ultrasound G.E.L. Podcast Blog. Published on September 26, 2016. Accessed on April 10, 2021. Available at https://www.ultrasoundgel.org/3.
- Kosuge M, Kimura K, Ishikawa T, et al. Electrocardiographic differentiation between acute pulmonary embolism and acute coronary syndromes on the basis of negative T waves. Am J Cardiol. 2007;99(6):817-821. doi:10.1016/j.amjcard.2006.10.043
- Buttner, E., 2021. ECG changes in Pulmonary Embolism • LITFL • ECG Library. [online] Life in the Fast Lane • LITFL. Available at: <https://litfl.com/ecg-changes-in-pulmonary-embolism/> [Accessed 21 April 2021].








1 thought on “Pulmonary embolism: Why do we miss it, and how do we get better?”
Pingback: ECG changes in Pulmonary Embolism • LITFL • ECG Library