Originally published at R.E.B.E.L. EM on March 24, 2016. Reposted with permission.
Follow Dr. Salim R. Rezaie at @srrezaie and Sam Ghali at @EM_RESUS
Post Written By: Sam Ghali (Twitter: @EM_RESUS)
 In cardiac arrest care there has been a lot of focus over the years on limiting interruptions in chest compressions during CPR. In fact, this concept has become a major focus of the current AHA Guidelines. Why? Because we know interruptions are bad [1,2]. One particular aspect of CPR that has gotten a lot of attention in this regard is the peri-shock period. It has been well established that longer pre- and peri-shock pauses are independently associated with decreased chance of survival [3,4].
In cardiac arrest care there has been a lot of focus over the years on limiting interruptions in chest compressions during CPR. In fact, this concept has become a major focus of the current AHA Guidelines. Why? Because we know interruptions are bad [1,2]. One particular aspect of CPR that has gotten a lot of attention in this regard is the peri-shock period. It has been well established that longer pre- and peri-shock pauses are independently associated with decreased chance of survival [3,4].
Traditionally when a shockable rhythm is encountered at the rhythm check, providers will charge the uncharged defibrillator at that time. In the meantime, chest compressions are typically resumed while waiting for the defibrillator to charge. Once the defibrillator has finished charging, providers are then forced to pause yet again in order to deliver the shock.
Realizing the vital importance of minimizing pauses in chest compressions, it has recently become popular for providers to go as far as continuing to perform chest compressions during defibrillation (“hands-on defibrillation”) – the goal being to effectively eliminate the additional interruption. There has been much debate as to whether this practice is safe for the provider or not. I am not going to get into this debate here as it has already been discussed on REBEL EM.
Instead, I would like to focus on what I believe to be a simple maneuver that based on existing evidence and simple logic should be implemented as standard care:
Pre-charging the defibrillator during the active chest compression phase of CPR, in anticipation of a shockable rhythm at the rhythm check.
Why should we wait until a shockable rhythm is encountered at the rhythm check to charge the defibrillator? This makes very little sense. Charging the defibrillator prior to the rhythm check is far more logical. With the defibrillator already charged and ready to go, if a shockable rhythm is encountered at rhythm check, the shock can be delivered immediately without any delay and importantly – a second interruption can be averted entirely.
So why has an illogical sequence of events become standard care in CPR? The answer is simple: it’s because that’s the way CPR has always been taught per ACLS. From the 2010 AHA/ACC guidelines:
“When a rhythm check by a manual defibrillator reveals VF/VT, the first provider should resume CPR while the second provider charges the defibrillator. Once the defibrillator is charged, CPR is paused to ‘clear’ the patient for shock delivery. After the patient is ‘clear,’ the second provider gives a single shock as quickly as possible to minimize the interruption in chest compressions (‘hands-off interval’).”
This is how this plays out during CPR:

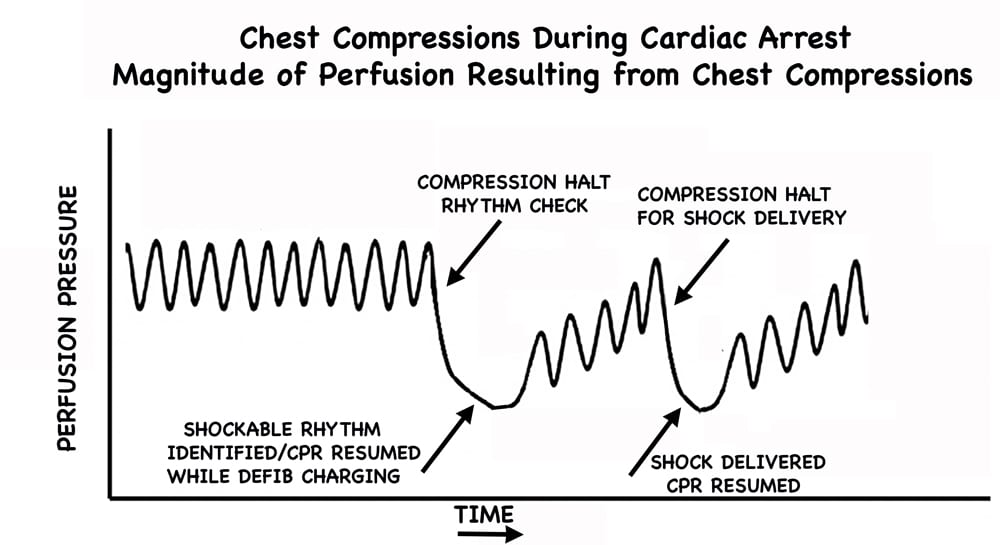
Image Modified from [2] The exact decrease in perfusion pressure for a specific time period is obviously variable, but this pictorial gives you an idea of the sequence of events and highlights the delay in shock delivery and the resulting detriment in not just one, but two interruptions in chest compressions.
By pre-charging the defibrillator during the active chest compression phase of CPR, encountering a shockable rhythm at the rhythm check plays out like this:

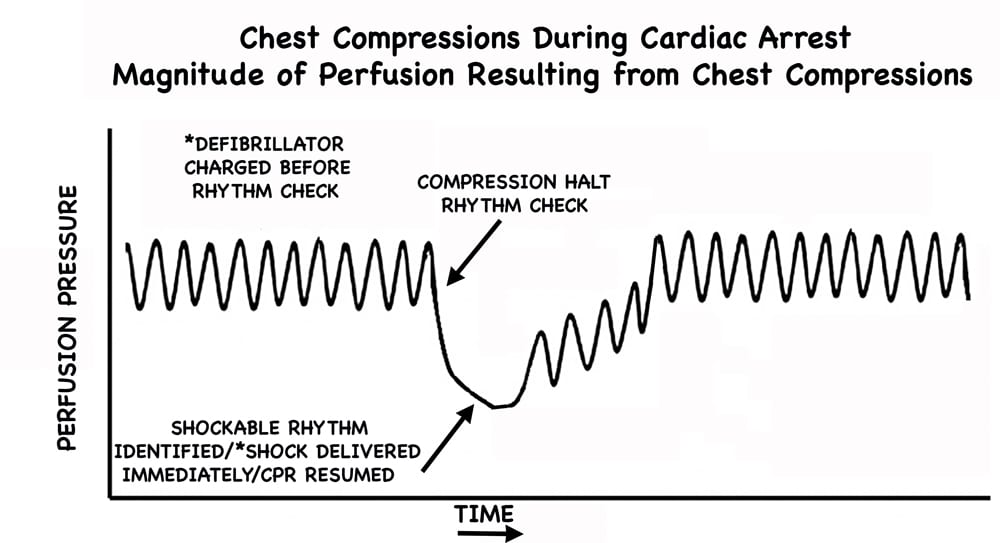
Image Modified from [2] Note: not only is the shock delivered earlier but the second interruption is avoided completely.
If the rhythm check happens to reveal a non-shockable rhythm, CPR can continue as per usual without any alteration. Of note, current defibrillators will “hold” the shock for some time (~60 seconds), and if the shock is not delivered in this time frame, the charge will dissipate and require re-charging. Therefore pre-charging should take place within this set time frame prior to a rhythm check. (Simply test your particular defibrillator to figure out exactly how long it holds the charge).
The only arguments I have ever heard against the implementation of this strategy is that it may increase the incidence of inappropriate or inadvertent shocks. The only study I know of looking at this method was a multi-center retrospective study from 2010 from Edelson et al [5]. Data were gathered from CPR-sensing defibrillator transcripts over a 3-year period. They looked at a total of 680 charge-cycles from 244 cardiac arrests. There was no difference in inappropriate shocks and there was only one instance of inadvertent shock administration during compressions (which went unnoticed by the compressor).
There will likely never be robust data looking at this particular aspect of CPR. It’s a small thing, but with potentially huge impact. I have personally been practicing CPR this way for years now. It has been my experience that it is an incredibly smooth process. All it takes is a little practice and team de-briefing to ensure all providers are on the same page. Does it improve outcomes? We may never definitively know. Will it ever make the guidelines? I suspect that eventually it will, perhaps with verbiage similar to something like this:
“It is reasonable to consider pre-charging the defibrillator during chest compressions…”
Until then, it is my opinion that based on data we do have, logic, and reasoning that pre-charging the defibrillator in anticipation of a shockable rhythm at the rhythm check is how we should be running our codes.
Clinical Bottom Line: Pre-charging the defibrillator during chest compressions in anticipation of a shockable rhythm at the rhythm check, decreases time to defibrillation and minimizes the number of pauses in chest compressions during CPR.
References:
- Berg RA et al. Adverse hemodynamic effects of interrupting chest compressions for rescue breathing during cardiopulmonary resuscitation for ventricular fibrillation cardiac arrest. Circulation 2001; 104 (20): 2465 – 70. PMID: 11705826.
- Cunningham LM et al. Cardiopulmonary resuscitation for cardiac arrest: the importance of uninterrupted chest compressions in cardiac arrest resuscitation. Am J Emerg Med 2012; 30 (8): 1630 – 8. PMID: 22633716
- Brouwer TF et al. Association Between Chest Compression Interruptions and Clinical Outcomes of Ventricular Fibrillation Out-of-Hospital Cardiac Arrest. Circulation 2015;132(11):1030-7. PMID: 26253757
- Cheskes S et al. Perishock pause: an independent predictor of survival from out-of-hospital shockable cardiac arrest. Circulation 2011; 124 (1): 58 – 66. PMID: 21690495
- Edelson DP et al. Safety and efficacy of defibrillator charging during ongoing chest compressions: a multi-center study. Resuscitation 2010; 81(11):1521-6. PMID: 20807672
Post Peer Reviewed By: Salim R. Rezaie (Twitter: @srrezaie) and Anand Swaminathan (Twitter: @EMSwami)








2 thoughts on “R.E.B.E.L. EM – Beyond ACLS: Pre-Charging the Defibrillator”
Guidelines. For the guidance of wise men and the obedience of fools.
We have been practicing like this in the hospital I currently work at for a while too – it makes shock delivery and compression resumption almost seamless. I wholeheartedly endorse and promote this approach amongst those I teach.
Great article – thanks.
Guidelines. For the guidance of wise men and the obedience of fools.
We have been practicing like this in the hospital I currently work at for a while too – it makes shock delivery and compression resumption almost seamless. I wholeheartedly endorse and promote this approach amongst those I teach.
Great article – thanks.