
Originally published at R.E.B.E.L. EM on May 26, 2022. Reposted with permission. Follow Salim R. Rezaie at @srrezaie
Background: Monkeypox is a poxviridae virus closely related to smallpox (variola). It was first described in humans in 1970 and has since become endemic in parts of Africa. In recent weeks, clusters of cases have been described in several countries prompting us to revisit this topic as it is not one we typically deal with in the ED.
The Virus:
- Family: Poxviridae
- Subfamily: Chordopoxvirinae
- Genus: Orthopoxvirus
- Species: Monkeypox virus
- Brick-shaped virus , surrounded by a lipoprotein envelope with linear double-stranded DNA genome
- Genetically distinct from other viruses of the Poxviridae family (i.e. variola, vaccinia, ectromelia, camelpox, and cowpox)
- There are two distinct clades of monkeypox virus [3]
- West African: More favorable prognosis with case fatality rate <1%
- Central Basin: more lethal, with a case fatality rate of up to 11% in unvaccinated children
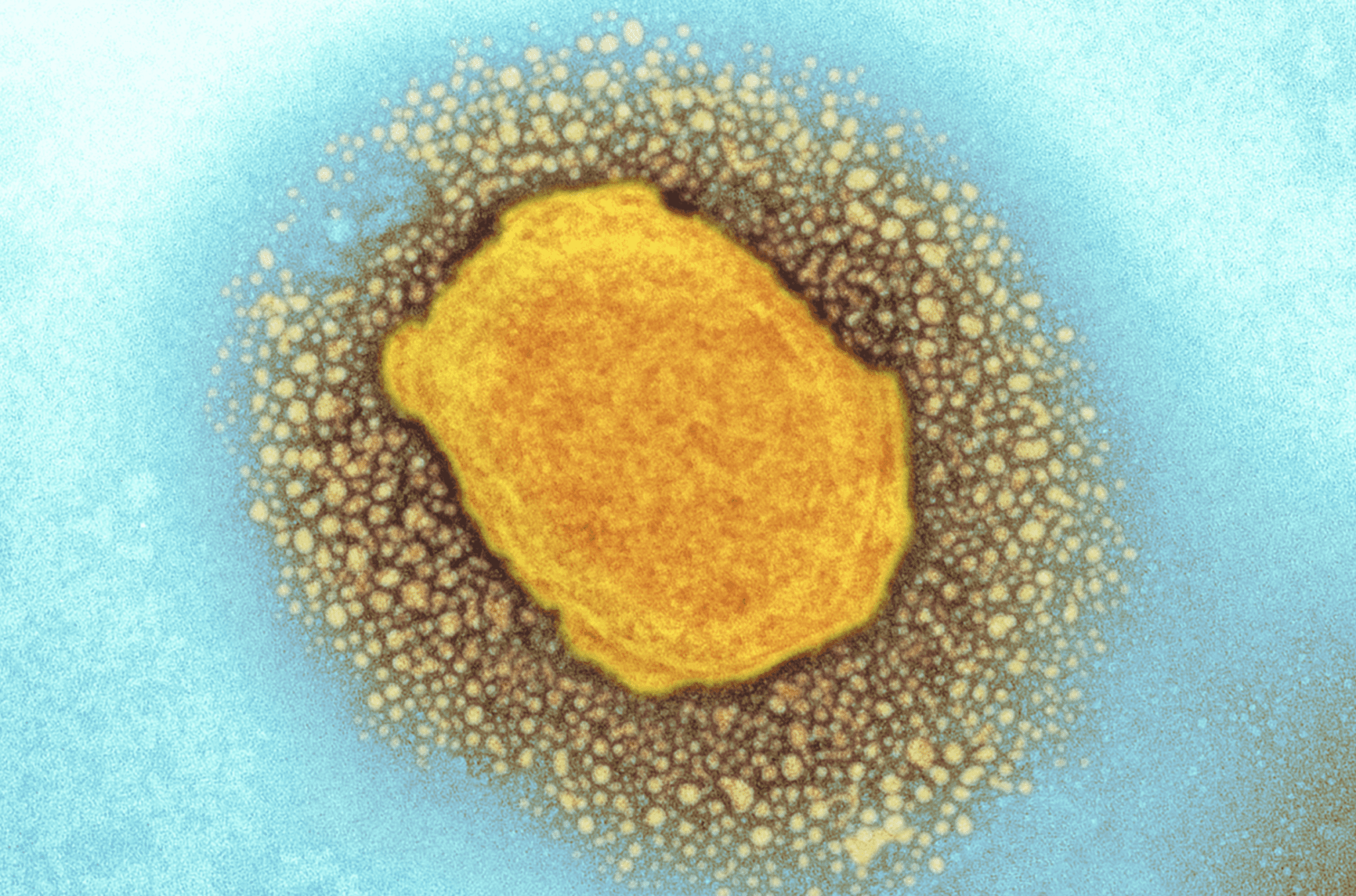
Image from Science Website [Link is HERE]
Epidemiology/Transmissibility:
- 1st identified in monkeys in 1958
- 1st human case reported in 1970
- Endemic in areas of Africa
- Typically, only see sporadic cases outside of Africa in people who have traveled to certain regions or have been in close contact with those travelers
- From the 1970s up until 2003, sporadic cases were identified in central and western Africa
- Before 1980, case-fatality rate was 17% and secondary transmission was the cause in 9% of cases
- From 1981 to 1986, the case-fatality rate was 10% and secondary transmission was the cause in 28%
- From 1996 to 1997, the largest outbreak of human monkeypox occurred, which had a case-fatality rate of 1.5% and secondary transmission was the cause in 78%
- The 2003 outbreak, was the first documented cases in the western hemisphere with a case-fatality rate of 0% and secondary transmission was the cause in 0%
- Cases of Monkeypox in 2022 from May 6th – 20th [2]:
- UK: 20 (Confirmed)
- Spain: 23 (Unconfirmed)
- Portugal 5 (Confirmed) + 15 (Unconfirmed)
- US 1 (Confirmed)
- Precise prevalence and incidence are limited (But both have increased since the discontinuation of routine smallpox vaccination)
- Wide range of hosts which has allowed a reservoir in wild animals and some sporadic cases in humans
- In contrast to smallpox, monkeypox associated with low transmissibility between human beings
- Mode of transmission remains poorly characterized:
- Large respiratory droplets most likely mode of transmission
- Direct contact through bodily fluids also possible
- The likelihood of transmission between individuals without prolonged close contact is considered to be low
Hosts/Reservoirs:
- Primary reservoir is thought to be squirrels, non-human primates, prairie dogs, rabbits, and rats
- Primary reservoir for human infection remains unknown
Who to Suspect:
- Travelers to known endemic areas
- Anyone in contact with a traveler to a known area
Clinical Features:
- Clinically monkeypox is almost indistinguishable from smallpox, chickenpox, and other causes of vesiculopustular rashes
- Typical incubation period 10 – 14 days (up to 21 days)
- Infectious period occurs during the 1st week of the rash
- 2-day prodrome manifested by fever, malaise, and lymphadenopathy typically occurs before development of rash
- Lymphadenopathy is key distinguishing characteristic of human monkeypox compared to smallpox
- 90% of patients infected with monkeypox develop lymphadenopathy (Typically in submandibular, cervical, postauricular, axillary, or inguinal areas)
- Rash begins as maculopapular lesions of 2 to 5mm in diameter
- Typically, centrifugal pattern (from the torso outwards)
- Can be monomorphic (like smallpox) or pleiomorphic (like chickenpox)
- Skin lesions typically progress from popular, to vesicular, to pustular, and crust phases over a 14-to-21-day period
- In patients with smallpox vaccination the rash will be milder and only ≈50% will have lymphadenopathy
- Most patients will not become seriously ill
- In the 2003, US outbreak (81 confirmed cases) there were zero deaths [1]
- Mortality seems to be higher in children, young adults, and immunocompromised individuals
- Generally, cases are mild, and people tend to recover within weeks
 Image from [1]
Image from [1]
 Image from [1]
Image from [1]
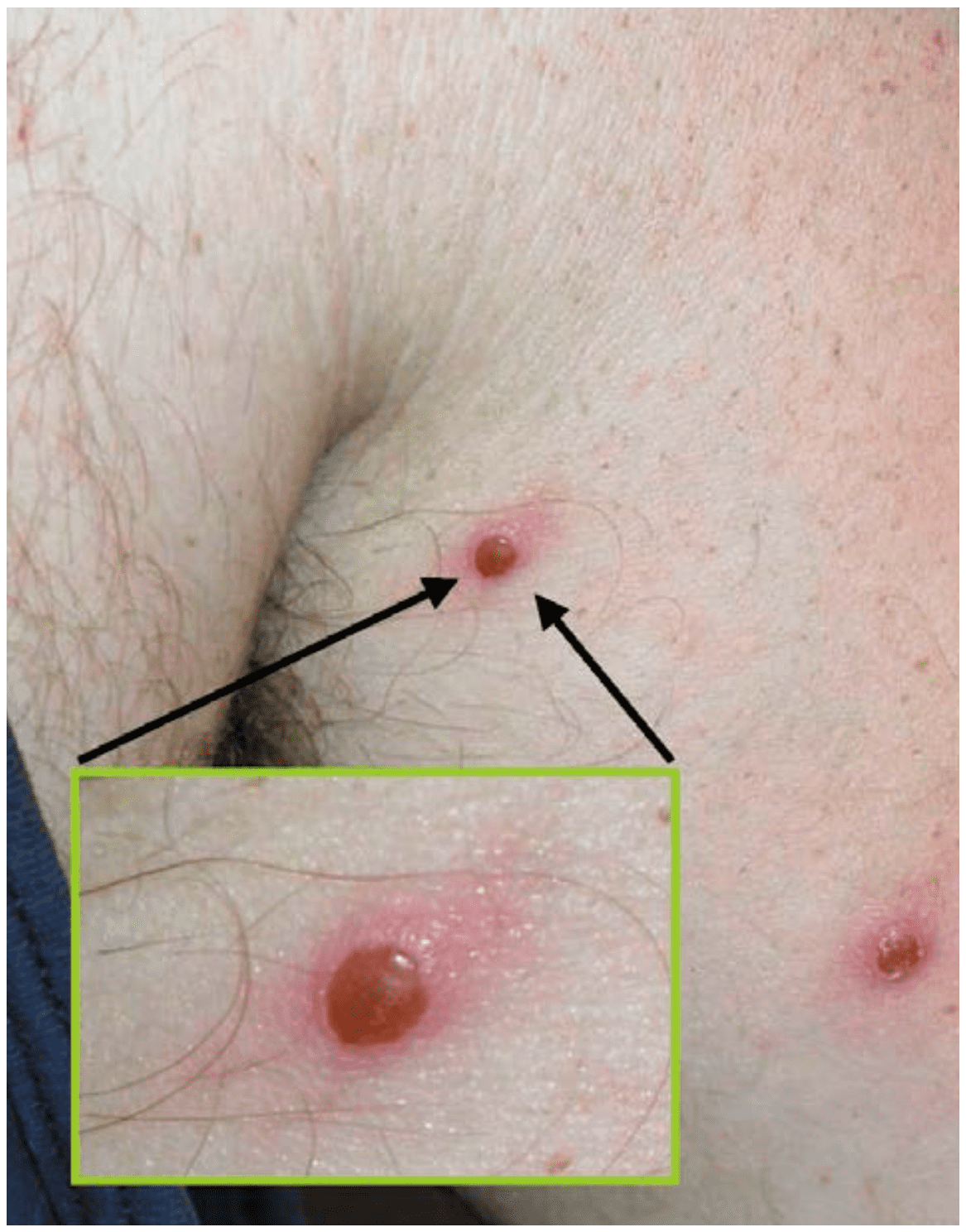 Image from [1]
Image from [1]
Monkeypox vs Chickenpox vs Measles

Complications:
- Bacterial superinfection of skin
- Skin scarring
- Corneal scarring/vision loss
- Pneumonia
- Dehydration (secondary to painful oral lesions and insensible fluid loss)
- Encephalitis
- Death (Very rare)
Diagnosis:
- Skin biopsy tissue and/or blood
- At a minimum, 2 scabs or material from vesicles should be collected in separate sterile containers
- DNA-based tests, such as PCR with sequencing, is the most precise method available for orthopoxvirus identification and species assignment
- Serological testing for monkeypox antigens is difficult because of close antigenic relation between surface antigens among orthopoxviruses
Treatment/Management:
- There is no proven treatment for monkeypox
- For contacts of a case, recommend twice daily fever/symptom monitoring for 21 days + Isolation recommended
- Currently, CDC recommending airborne and contact precautions (i.e. negative pressure room, N95, gloves, and eye shield)
- Pre-exposure smallpox vaccination has been shown to confer 85% protection against monkeypox [1]
- Role of post-exposure smallpox vaccination is less clear
- According to the CDC, vaccination within 4 days of exposure may prevent disease onset and vaccination within 14 days may reduce disease severity [3]
- Vaccinia immune globulin has no available data on effectiveness in the treatment of monkeypox
- For severe cases, antiviral agents with known activity against orthopoxviruses in animal studies (No published data on its effectiveness for treatment on human monkeypox)
- Cidofovir a broad-spectrum antiviral agent with in-vitro activity against virtually all DNA virsuses
- Brincidofovir an oral DNA polymerase inhibitor
- Tecovirmat an oral intracellular viral release inhibitor
References:
- Di Giulio DB et al. Human Monkeypox: An Emerging Zoonosis. Lancet Infect Dis 2004. PMID: 14720564
- Mahase E. Monkeypox: What do we Know About the Outbreaks in Europe and North America? BMJ 2022. PMID: 35595274
- Moore M et al. Monkeypox. StatPearls 2021. [Link is HERE]
For More on this Topic Checkout:
- First10EM: Monkeypox
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)
Cite this article as: Salim Rezaie, “Monkeypox…The Basics”, REBEL EM blog, May 26, 2022. Available at: https://rebelem.com/monkeypoxthe-basics/.




