Authors: James L Webb, MD (Internal Medicine, SAUSHEC, USAF) and Brit Long, MD (@long_brit) // Edited by: Erica Simon, DO, MHA (@E_M_Simon) & Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
A 20 year-old female presents to the ED after a witnessed fall. According to bystanders, the young woman was walking towards a gym treadmill when she collapsed to the floor below, convulsing for approximately1-2 minutes. Upon EMS arrival VS were within normal limits, GCS was noted as 14 (confusion, orientation only to self), EKG revealed NSR, and accucheck demonstrated a blood glucose of 134. Intravenous access was obtained en route to your facility.
As you interview and examine the patient, you note ABCs intact, a GCS of 15, an ample history remarkable only for report of a “rising feeling in the abdomen” prior to the event, and a secondary survey without obvious signs of trauma. ED evaluation, to include a CBC, CMP, EKG, and non-contrasted head CT are all within normal limits. Urine Hcg is negative.
Was this a seizure? What’s the appropriate patient disposition? If you’ve got questions, we’ve got important details on seizures and their mimics.
Background
Current data indicate that nearly 2 million U.S. residents are affected by Epilepsy.1-2 In addition to this population, approximately 150,000 Americans (age >18 years) present to healthcare providers annually following an apparent first seizure.1-2 As assigning a diagnosis a seizure or seizure disorder is not without significant health and quality of life implications (employment repercussions, driving restrictions, etc.1-5), emergency physicians must be aware of conditions that may mimic seizure activity: syncope, psychogenic non-epileptic seizures, metabolic derangements, stroke or TIA, sleep disorders, and migraines.
Seizures – A Review
Seizures result from abnormal neurologic electrical activity. This abnormal activity can occur in both hemispheres (generalized seizure) or within one hemisphere (focal seizure), which may spread to the entire brain. Generalized seizures are more common than focal seizures, and often have a genetic association.6 Generalized tonic-clonic seizures most frequently occur in adults – the motions of which consist of a tonic phase with muscle stiffening, followed by a clonic phase with rhythmic muscle contractions.6-7 Focal seizures often occur in the setting of cerebral insult.7 Unlike generalized seizures, symptoms of focal seizures vary according to the anatomic location of the abnormal electrical activity.6,8
Seizures can be classified as provoked or unprovoked. Provoked seizures are those with identifiable causes, which can be isolated to the brain, or are thought to occur secondary to a systemic disorder or illness. Such causes include: brain trauma, CNS infection (i.e. meningitis, encephalitis, brain abscess), anoxic brain injury, intracranial hemorrhage or surgery, metabolic disorders, illicit drug abuse or intoxication (most commonly tricyclic antidepressants and isoniazid), or alcohol withdrawal.9,10 Seizures may also occur in the setting of metabolic derangements (hypoglycemia or hyponatremia).9-12
Unprovoked seizures are those with no discernible cause, or those occurring greater than seven days following precipitating factors or events. What factors or events might the emergency physician identify through the H&P?
- Pregnant patient with a seizure –>evaluate for eclampsia
- Child with an recent illness –>evaluate for personal and familial history of febrile seizures
- In all patients –>inquire regarding a history of recent head trauma (occurring within 1 week prior to presentation)
It is particularly important to perform a thorough H&P in this patient population, as 50% of individuals experiencing an unprovoked seizure will experience a recurrence.11
Approach
Patients presenting with altered mental status (AMS)/seizure concern should be quickly assessed10,13-15,17:
- ABCs
- Consider obtaining a POC glucose level
- First line treatment for seizure activity: benzodiazepines (lorazepam 0.1 mg/kg IV)
- Second line agents: phenytoin, fosphenytoin, levetiracetam, or valproic acid
- Intubation with propofol or ketamine with contiguous EEG (in consultation with neurology) may be required.14-17
- After addressing ABCs, perform an H&P, complete a physical examination (PE), and obtain IV access. Consider: CBC, CMP, EKG, serum Hcg, anticonvulsant level if applicable, imaging as appropriate (CT recommended in the setting of new focal deficits, head trauma, continued AMS, immunocompromised state, history of cancer, persistent fever, focal seizures, history of stroke, or anticoagulation), +/- an LP.13,15-19
- Note: neuroimaging should be performed in patients with suspected new-onset seizures, but may occur in the outpatient setting for those with a first time generalized tonic-clonic seizure with a normal neurologic exam. MRI is preferable with a higher yield of identifying abnormalities in the non-emergent setting.13,15-19
- Disposition is often determined in conjunction with specialty consultation. Admission may be required in the setting of persistent neurologic deficit, persistent AMS, or poor social situation.13,15-19 Patients who return to mental status baseline, possess a normal neurologic exam, and whose labs and imaging are without pathology, may be discharged with outpatient follow-up.13,19
- Second line agents: phenytoin, fosphenytoin, levetiracetam, or valproic acid
For an in-depth discussion of seizure evaluation and management, see: http://www.emdocs.net/treatment-of-seizures-in-the-emergency-department-pearls-and-pitfalls/
Evaluating Seizure Activity in Patients with Return to Mental Status Baseline
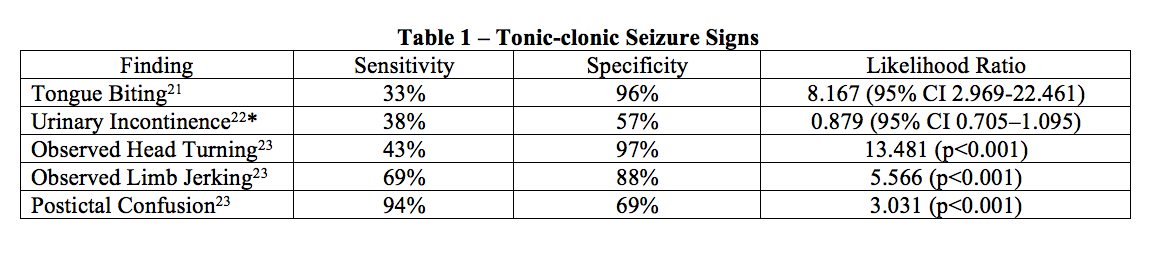
A definitive diagnosis of seizure is made by EEG interpretation during seizure activity. As this is often times impossible in the ED setting, the emergency physician must seek out signs and symptoms commonly associated with seizure activity9,13,20:
- HPI significant for aura: déjà vu, a rising sensation in the abdomen, abnormal taste or smell, or autonomic changes.
- Activity commonly associated with a true seizure: witnessed tonic/clonic movements or observed head turning in the setting of a generalized seizure, or the abrupt onset of limb movements, abnormal sensations, or hallucinations in the setting of a focal seizure. 6,7,20
- A postictal period occurring for minutes to hours with confusion, disorientation, and drowsiness.
- Physical exam remarkable for tongue biting.
See Table 1 for signs and symptoms related to seizure activity in studies comparing seizures versus syncope. *Urinary incontinence was demonstrated to lack clinical significance.
What about laboratory studies?
A lactate level may be useful in differentiating seizures from psychogenic non-epileptic seizures and syncope (sensitivity of 88%, specificity 87% for true seizure activity), 24 while an elevated CK is suggestive of epileptic seizures (specificity 85-100%), but demonstrates variable sensitivity (15-88%).25
Seizure Mimics
Studies indicate that approximately 20% of patients presenting for evaluation of seizure are misdiagnosed as having epilepsy.26 Conditions most commonly mistaken for epitileptiform seizure activity include syncope and psychogenic non-epileptic seizures.5 Detailed below is a review of seizure mimics with tips and tricks for ED evaluation and disposition.
Syncope
Syncope is a sudden loss of consciousness (LOC) due to decreased cerebral perfusion, resulting in loss of postural tone, with rapid return to mental status baseline. Syncope may be cardiac, orthostatic, or neurocardiogenic (vasovagal) in origin.
Historical evidence favoring a syncopal episode versus a seizure27-34:
- Presentation –>LOC with rapid return to mental status baseline.
- History –>Remarkable for precipitating factors: recent illness (emesis/diarrhea – hypovolemia), recent medication changes (i.e. B-blockers and bradycardia, diuretics causing hypovolemia, etc.), LOC following increased vagal tone (coughing, defecation, shaving). LOC during physical exertion. In obtaining the HPI, it is important to note that myoclonic jerking occurs in up to 90% of patients experiencing syncope.27
Management and Disposition Pearls:
- Evaluation –> EKG for dysrhythmias, consider a CBC and CMP to assess for anemia and electrolyte derangement, consider cardiac markers as indicated.
- Disposition–>As appropriate. Referral for tilt-table testing in the setting of neurocardiogenic syncope may be considered after ruling out life-threatening conditions.
Notes on Syncope of Cardiac Origin
Syncope secondary to cardiac dysrhythmias or structural heart disease may present similarly to a seizure, however, the following suggest cardiac origin27-29, 33,34:
- Presentation –>Most commonly an elderly patient.
- History –>The absence of a prodrome; ROS positive for palpitations prior to LOC; CP or LOC during exertion.
Management and Disposition Pearls:
- Evaluation –>PE for murmurs, rubs, gallops and s/s of heart failure (JVD, peripheral edema, hepatojugular reflex, etc.); EKG for dysrhythmias: SVT, VT, Mobitz type II second-degree, or third-degree AV block, bundle branch blocks, Long QT Syndrome, Brugada Syndrome, WPW Syndrome, Right Ventricular Dysplasia, and pacemaker malfunction have all been associated with syncopal episodes.33 Consider bedside POCUS or formal echocardiogram to evaluate for cardiac structural anomalies.
- Disposition –>As appropriate. In the large majority of cases admission is required for adjunct testing.
Psychogenic Non-Epileptic Seizure (PNES) Disorder
PNES, a condition characterized by the presence of seizure-like activity occurring in the absence of EEG changes, is difficult to differentiate from a true seizure in the emergency setting; even more so as nearly 40% of patients with epilepsy suffer from the disorder.35 Characteristics that make PNES more likely include35-39:
- Presentation –>Patient in their 20s-30s,35 experiencing an event characterized by asynchronous extremity movements, rapid head turning, pelvic thrusting, eye closing, or geotropic eye movements. Clinical clues useful for the provider: the absence of tongue biting, a prolonged duration (>2 mins), a patient who can recall the event, or a patient who was witnessed to have been crying during the seizure-like activity.
- History –>Approximately 70% have a PMHx of a psychiatric disorder (depression, PTSD, personality disorder).36,37
Management and Disposition Pearls:
- Evaluation –>When in doubt: treatment as appropriate (ABCs +/- benzodiazepines). Video EEG is the gold standard for diagnosis, therefore specialty consultation is required.
- Disposition –>In consultation with neurology/neuropsychiatry. Treatment is often targeted to the underlying psychiatric disorder.39
Metabolic Derangements
Metabolic disorders are identified in 2.4-8% of patients presenting with first generalized seizure.9,10,13 Hypoglycemia and hyponatremia are the most common, but other disorders may include hypernatremia, hyperglycemia, hypercalcemia, and uremia.9,10,13
Management and Disposition Pearls:
- Evaluation –>Accucheck for all patients with AMS/seizure activity. CMP as appropriate.
- Disposition –>Treatment and admission requirements based upon laboratory findings.
Stroke and TIA
Stroke/TIA can be confused with a seizure when there is resolution of the neurologic deficit previously caused by cerebral ischemia. Characteristics of Stroke/TIA18,40,41:
- Presentation –>Most commonly a middle-aged or elderly patient. HPI remarkable for negative symptoms: numbness, weakness, or blindness.
- History –>PMHx significant for HTN, HLD, cardiac arrhythmia, family history of CVA
Management and Disposition Pearls:
- Evaluation –>PE: focused neurological examination, accucheck, EKG for dysrhythmias, performance of risk stratification to determine the requirement for cerebral vasculature imaging.
- Disposition –>As appropriate. Inpatient admission may be required for MRI, carotid ultrasonography, echocardiography, and medication optimization.
Sleep Disorders
Narcolepsy with cataplexy may present similarly to seizures. Narcolepsy is defined by excessive daytime sleepiness, lapses into sleep, or multiple naps during the same day at least 3 times per week for a duration of 3 months time. Cataplexy is the sudden loss of tone in response to emotion. 42-45
- Presentation –>Patient suddenly collapses, but rapidly recovers to mental status baseline with complete recollection of the event. 42-45
Management and Disposition Pearls:
- Evaluation –>Thorough history-taking often allows differentiation from seizure activity.
- Disposition –>Specialty referral for overnight polysomnography and sleep latency testing. Driving restriction is often state-mandated if the condition is suspected. 42-45
Migraines
Migraines are recurrent headaches with or without aura (visual or sensory symptoms). Symptoms include throbbing headache, nausea, vomiting, and sensitivity to light and sound. Auras are often positive visual symptoms. Migraines with aura are similar to certain focal seizures with visual symptoms (hallucinations) or generalized seizure prodrome (aura). Signs and symptoms making a diagnosis of migraine more likely19, 50-52:
- Presentation –>headache characterized by unilateral pain, throbbing pain, moderate-severe pain, and aggravated by physical activity, +/- nausea/vomiting or photo-/phonophobia
- History –>PMHx significant for migraines.
Keep in mind, complex migraines may present with neurologic symptoms causing weakness, alteration in consciousness, or LOC.
Management and Disposition Pearls:
- Evaluation –>PE: focused neurological examination. Rule out intracranial pathology as appropriate (CVA/SAH/meningitis/encephalitis – CT, LP, etc.)
- Disposition –>As appropriate. In the setting of negative imaging (+/- negative LP), neurology consultation is appropriate as prophylactic medications (TCAs, B-blockers, anti-epileptics) may be considered for outpatient therapy.
Summary
– Seizures are caused by abnormal neurologic electrical activity resulting in motor, sensory, and behavioral symptoms.
– In all patients presenting with AMS or actively seizing: ABCs, accucheck, initiate therapy as appropriate (benzodiazepines first line).
– For patients presenting after return to baseline mental status: a thorough history and physical examination are key to differentiating between a true seizure and its mimic.
– If a seizure is not suspected, consider syncope, psychogenic non-epileptic seizures, stroke or TIA, sleep disorders, and migraines.
References/Further Reading
- Hauser WA, Beghi E. First seizure definitions and worldwide incidence and mortality. Epilepsia. 2008;49 Suppl 1:8-12.
- Krumholz A, Wiebe S, Gronseth GS, et al. Evidence-Based Guideline: Management of an Unprovoked First Seizure in Adults: Report of the Guideline Development Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Epilepsy Curr. 2015 May-Jun;15(3):144-52.
- Lowenstein DH, Alldredge BK. Status epilepticus. N Engl J Med. 1998 Apr 2;338(14):970-6.
- England MJ, Livermari CT, Schultz AM, Strawbridge LM Institute of Medicine (US) Committee on the Public Health Dimensions of the Epilepsies; England MJ, Livermari CT, Schultz AM, Strawbridge LM, editors. Epilepsy Across the Spectrum: Promoting Health and Understanding. Washington, DC: The National Academies Press; 2012.
- Xu Y, Nguyen D, Mohamed A, et al. Frequency of a false positive diagnosis of epilepsy: A systematic review of observational studies. 2016 Aug 23;41:167-174.
- Berg AT, Berkovic SF, Brodie MJ, et al. Revised terminology and concepts for organization of seizures and epilepsies: report of the ILAE Commission on Classification and Terminology, 2005-2009. Epilepsia. 2010 Apr;51(4):676-85.
- Chang BS, Lowenstein DH. Epilepsy. N Engl J Med. 2003 Sep 25;349(13):1257-66.
- Fisher RS, Acevedo C, Arzimanoglou A, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. 2014;55(4):475.
- Beghi E, Carpio A, Forsgren L, et al. Recommendation for a definition of acute symptomatic seizure. Epilepsia. 2010;51(4):671.
- Fields MC, Labovitz DL, French JA. Hospital-onset seizures: an inpatient study. JAMA Neurol. 2013 Mar;70(3):360-4.
- Riggs JE. Neurologic manifestations of electrolyte disturbances. Neurol Clin. 2002 Feb;20(1):227-39.
- D’Onofrio G, Rathlev NK, Ulrich AS, et al. Lorazepam for the prevention of recurrent seizures related to alcohol. N Engl J Med. 1999 Mar 25;340(12):915-9.
- Dunn MJ, Breen DP, Davenport RJ, Gray AJ. Early management of adults with an uncomplicated first generalised seizure. Emerg Med J. 2005 Apr;22(4):237-42.
- Pillow MT. Seizure Assessment in the Emergency Department. Emedicine: Medscape. http://emedicine.medscape.com/article/1609294-overview. Accessed 11 August 2016.
- American College of Emergency Physicians. Clinical policy: Critical issues in the evaluation and management of adult patients presenting to the emergency department with seizures. Ann Emerg Med. 2014 Apr;63(4):437-47.e15.
- Shorvon S, Ferlisi M. The treatment of super-refractory status epilepticus: a critical review of available therapies and a clinical treatment protocol. Brain. 2011 Oct;134(Pt 10):2802-18.
- Brophy, Gretchen M., Claassen J, et al. Guidelines for the evaluation and management of status epilepticus. Neurocrit Care 2012 Aug;17(1):3-23.
- Harden CL, Huff JS, Schwartz TH, et al. Reassessment: neuroimaging in the emergency patient presenting with seizure (an evidence-based review): report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2007 Oct 30;69(18):1772-80.
- French JA, Pedley TA. Clinical practice. Initial management of epilepsy. N Engl J Med. 2008 Jul 10;359(2):166-76.
- Manford M. Assessment and investigation of possible epileptic seizures. J Neurol Neurosurg Psychiatry. 2001;70(Suppl 2):ii3–ii8.
- Brigo F, Nardone R, Bongiovanni LG. Value of tongue biting in the differential diagnosis between epileptic seizures and syncope. Seizure. 2012 Oct;21(8):568-72.
- Brigo F, Nardone R, Ausserer H, et al. The diagnostic value of urinary incontinence in the differential diagnosis of seizures. Seizure. 2013 Mar;22(2):85-90.
- Sheldon R, Rose S, Ritchie D, et al. Historical criteria that distinguish syncope from seizures. J Am Coll Cardiol. 2002 Jul 3;40(1):142-8.
- Matz O, Zdebik C, Zechbauer S, et al. Lactate as a diagnostic marker in transient loss of consciousness. Seizure. 2016 Aug;40:71-5.
- Brigo F, Igwe SC, Erro R, Bongiovanni LG, et al. Postictal serum creatine kinase for the differential diagnosis of epileptic seizures and psychogenic non-epileptic seizures: a systematic review. J Neurol. 2015 Feb;262(2):251-7.
- Smith PE. Epilepsy: mimics, borderland and chameleons. Pract Neurol. 2012 Oct;12(5):299-307.
- Chen LY, Benditt DG, Shen WK. Management of syncope in adults: an update. Mayo Clin Proc. 2008 Nov;83(11):1280-93.
- Walsh K, Hoffmayer K, Hamdan MH. Syncope: diagnosis and management. Curr Probl Cardiol. 2015 Feb;40(2):51-86.
- Huff JS, Decker WW, Quinn JV, et al.; American College of Emergency Physicians. Clinical policy: critical issues in the evaluation and management of adult patients presenting to the emergency department with syncope. Ann Emerg Med. 2007 Apr;49(4):431-44.
- Grubb BP. Clinical practice. Neurocardiogenic syncope. N Engl J Med. 2005 Mar 10;352(10):1004-10.
- Lempert T, Bauer M, Schmidt D. Syncope: a videometric analysis of 56 episodes of transient cerebral hypoxia. Ann Neurol 1994 Aug;36(2):233–7.
- McKeon A, Vaughan C, Delanty N. Seizure versus syncope. Lancet Neurol. 2006 Feb;5(2):171-80.
- Morag R. Syncope. Emedicine: Medscape. http://emedicine.medscape.com/article/811669-overview. Accessed 15 August 2016.
- Moya A, Sutton R, Ammirati F, et al. Guidelines for the diagnosis and management of syncope (version 2009). the task force for the diagnosis and management of syncope of the European Society of Cardiology (ESC). Eur Heart J. 2009 Nov;30(21):2631-71.
- Alsaadi TM, Marquez AV. Psychogenic nonepileptic seizures. Am Fam Physician. 2005 Sep 1;72(5):849-56.
- Panagos PD, Merchant RC, Alunday RL. Psychogenic seizures: a focused clinical review for the emergency medicine practitioner. Postgrad Med. 2010 Jan;122(1):34-8.
- Shaibani A, Sabbagh MN. Pseudoneurologic syndromes: recognition and diagnosis. Am Fam Physician. 1998 May 15;57(10):2485-94.
- LaFrance WC Jr, Baker GA, Duncan R, et al. Minimum requirements for the diagnosis of psychogenic nonepileptic seizures: a staged approach: a report from the International League Against Epilepsy Nonepileptic Seizures Task Force. 2013 Nov;54(11):2005-18.
- Siket MS, Merchant RC. Psychogenic seizures: A review and description of pitfalls in their acute diagnosis and management in the emergency department. Emerg Med Clin North Am. 2011 Feb;29(1):73-81.
- Johnston SC. Clinical practice. Transient ischemic attack. N Engl J Med 2002 Nov 21; 347(21):1687-92.
- Nanda A. Transient Ischemic Attack. Emedicine: Medscape. http://emedicine.medscape.com/article/1910519-overview. Accessed 22 August 2016.
- American Academy of Sleep Medicine. The International Classification of Sleep Disorders-Revised: Diagnostic and Coding Manual. 3rd ed. Rochester, MN: American Academy of Sleep Medicine; 2014.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American Psychiatric Association; 2013. 372-78.
- Bozorg, A. Narcolepsy. Emedicine: Medscape. http://emedicine.medscape.com/article/1188433-overview. Accessed 22 August 2016.
- Scammell TE. Narcolepsy. N Engl J Med. 2015 Dec 31;373(27):2654-62.
- Tarsy D, Simon D. Dystonia. N Engl J Med. 2006 Aug 24;355(8):818-29.
- Smith PE. If it’s not Epilepsy. J Neurol Neurosurg Psychiatry 2001;70:9-14.
- Moberg-Wolff EA. Dystonias. Emedicine: Medscape. http://emedicine.medscape.com/article/312648-overview. Accessed 22 August 2016.
- Albanese A, Barnes MP, Bhatia KP, et al. A systematic review on the diagnosis and treatment of primary (idiopathic) dystonia and dystonia plus syndromes: report of an EFNS/MDS-ES Task Force. Eur J Neurol. 2006 May;13(5):433-44.
- Sances G, Guaschino E, Perucca P, et al. Migralepsy: a call for a revision of the definition. Epilepsia 2009;50:2487–96.
- Goadsby PJ, Lipton RB, Ferrari MD. Migraine–current understanding and treatment. N Engl J Med. 2002 Jan 24;346(4):257-70.
- Chawla J. Migraine. Emedicine: Medscape. http://emedicine.medscape.com/article/1142556-overv





3 thoughts on “Seizure Mimics: Pearls & Pitfalls”
Pingback: Länkar v52-1 | Internmedicin
Pingback: emDOCs.net – Emergency Medicine EducationThe EM Educator Series: Subtleties of Seizures - emDOCs.net - Emergency Medicine Education
Pingback: Nerdfallmedizin.de - NERDfall Nr. 15 – Teil 2: Dissoziative Krampfanfälle – gar nicht so selten und häufig fehlinterpretiert