Stroke and TIA: Pearls and Pitfalls
By William C. Ferguson, Daniel K. Crane MD, Alexander X. Lo MD/PhD
(University of Alabama at Birmingham, Department of Emergency Medicine)
Edited by Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Stephen Alerhand, MD (@SAlerhand)

Ischemic Stroke
The basics
- Approximately 800,000 new strokes per year or 2,300 per day in the U.S.
- Leading cause of disability and 4th leading cause of death in the U.S.
- Over 75% of all strokes in adults are ischemic
- 1996: recombinant tissue plasminogen activator (tPA) was approved by the FDA for acute ischemic stroke treatment within 3 hours of verified onset of deficits
- Fewer than 6% of all adults with acute ischemic strokes meet treatment protocol criteria and receive tPA
Facts and controversies surrounding tPA
- In 2013, the American College of Emergency Physicians and the American Academy of Neurology jointly published a clinical policy statement that “IV tPA should be offered to acute ischemic stroke patients who meet National Institute of Neurological Disorders and Stroke (NINDS) inclusion/exclusion criteria.” (of note: the ACEP policy is currently being updated)
- The 1995 NINDS Stroke Study clinical trial studied the efficacy of recombinant tissue plasminogen activator (r-tPA) and found a higher proportion with improved disability at 3 months among individuals treated with tPA within 3 hours of symptom onset than those receiving placebo (39% vs. 26%, p=0.008)
- The NINDS trial showed no benefit or harm to mortality risk with tPA, despite an increased risk of intracerebral hemorrhage (6% risk compared to 0.6% in the placebo group)
- Two additional trials of IV-tPA (ECASS II, ATLANTIS) using either the same dose but with an extended treatment window (6 hours) or a higher tPA dose of 1.1 mg/kg (ECASS I) did not show a treatment benefit
- The support for tPA benefit in the 3-hour window comes from
- Subgroup analysis of another trial limited to only those participants sharing the same treatment parameters (ATLANTIS Part B)
- Class II patient-level meta-analysis combining data from different trials (NINDS, ECASS, ATLANTIS and EPITHET)
- Two separate re-analyses of the original NINDS data
- Post-marketing efficacy studies, in the U.S. and other countries, showed treatment results no different than the original NINDS trial and with an ICH risk of 4.6 to 7.4%
- Critics of tPA point out that in actuality there has never been a dedicated clinical trial that replicated the original NINDS trial
Regionalization of stroke care
- Early access to Primary or Comprehensive Stroke Centers improves long-term outcomes
Interhospital transfer of acute stroke patients: “Drip and Ship”
- Interhospital transfer after intravenous tissue-type plasminogen activator (tPA) in acute stroke (drip and ship) accounts for 1 out of every 4 to 6 patients receiving tPA
- The evidence to date suggests that the “Drip and Ship” method is not associated with a significantly increased risk of ICH or death.
IV tPA for persons on warfarin with acute ischemic stroke
- Two large registry studies demonstrate that tPA is safe in persons on warfarin if INR <1.7
IV tPA for stroke mimics
- Between 1.5% and 4% of strokes treated with IV tPA were stroke mimics
- Stroke mimics were younger and with fewer stroke symptoms
- 1% of stroke mimics receiving tPA had a symptomatic ICH, although this estimate was based on numbers too small to provide an accurate description of safety or harm related to tPA in stroke mimics with any statistical confidence
G2b3a inhibitor bad for ischemic stroke
- Clinical trials involving GP IIb-IIIa inhibitors for treatment of acute ischemic stroke have all found no treatment benefit in terms of disability or death, and treatment was associated with a significantly increased risk of intracranial hemorrhage
Hypothermia for stroke
- Limited human clinical trial data but so far shows no evidence to support benefit in terms of improvement in death or disability. A large (N=1500) European trial is currently underway.
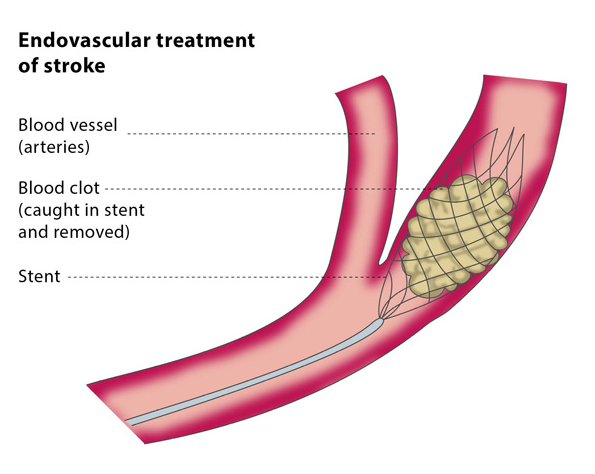
Endovascular Stroke Treatment
- Indicated for acute stroke patients within 6 hours of symptom onset and with large vessel occlusions identified on CT, CT-A, or perfusion imaging
- Patients with large vessel occlusions generally have a higher risk of death and severe disability compared to those with small vessel occlusions
- These patients also have poorer revascularization rates with TPA. (4,5)
- Four recent large, multi-center trials using a new generation of retrievable stents (MR CLEAN, ESCAPE, EXTEND-IA, and SWIFT PRIME) have shown a benefit of endovascular treatment over tPA alone (1,2,3)
- There was no difference in outcome in study patients who did or did not receive tPA.
- These results may lead to a change in standard of care where stroke patients receive tPA (if eligible) and then undergo further imaging to determine eligibility for endovascular therapy
- If endovascular management is not available at that facility, eligible patients should be transferred to the nearest endovascular treatment facility
http://cirse.org/index.php?pid=1043
Transient Ischemic Attacks (TIA)
Definition of TIA
- TIA was traditionally defined as focal neurological symptoms or signs lasting 24 hours
- However, improved imaging studies have shown an infarction in many cases (6)
- As a result, there is a now a tissue-based definition of TIA: a transient episode of neurological dysfunction caused by focal brain, spinal cord, or retinal ischemia, without acute infarction. (7)
- Patients with TIAs are at high risk for early stroke, as high as nearly 15% risk of stroke in the 90 days after a TIA (8)
ED management of the person with TIA
- All TIA patients should undergo risk stratification using the ABCD2 score (not great tool but current go-to):
- Age > 60 years (1 point)
- Blood Pressure > 140/90 mm Hg (1 point)
- Clinical Symptoms
- Unilateral focal weakness (2 points)
- Speech impairment without weakness (1 point)
- Other symptoms (0 point)
- Duration
- 60 minutes (2 points)
- 10 to 59 minutes (1 point)
- <10 minutes (0 point)
- History of Diabetes (1 point)
- The ABCD2 score provides a validated 2-day risk of stroke:
- Score of 0 or 1: Risk of stroke <1%
- Score of 2 or 3: Risk of stroke 1.3%
- Score of 4 or 5: Risk of stroke 4.1%
- Score of 6 or 7 (9): Risk of stroke 8.1%
- AHA/ASA recommends hospitalization for score > 2 (6)
- The TIA work-up as recommended by the American Heart Association and American Stroke Association includes (6)
- Neuroimaging evaluation within 24 hours of symptom onset, preferably MRI with diffusion weighted imaging
- Noninvasive imaging (US, MRA, CTA) of the cervical vessels and optional recommended noninvasive imaging of intracranial vessels
- Electrocardiography and cardiac monitoring
- Routine blood tests
Selected References / Further Reading
– American College of Emergency Physicians; American Academy of Neurology. Clinical Policy: Use of intravenous tPA for the management of acute ischemic stroke in the emergency department. Ann Emerg Med. 2013 Feb;61(2):225-43. doi: 10.1016/j.annemergmed.2012.11.005.
– Millard WB. New guidelines on tPA in stroke: putting out fires with gasoline? Ann Emerg Med. 2013 Jul;62(1):A13-8. doi: 10.1016/j.annemergmed.2013.05.010.
– Alberts MJ1, Latchaw RE, Selman WR, Shephard T, Hadley MN, Brass LM, Koroshetz W, Marler JR, Booss J, Zorowitz RD, Croft JB, Magnis E, Mulligan D, Jagoda A, O’Connor R, Cawley CM, Connors JJ, Rose-DeRenzy JA, Emr M, Warren M, Walker MD; Brain Attack Coalition. Recommendations for comprehensive stroke centers: a consensus statement from the Brain Attack Coalition. Stroke. 2005 Jul;36(7):1597-616. Epub 2005 Jun 16.
– Sheth KN, Smith EE, Grau-Sepulveda MV, Kleindorfer D, Fonarow GC, Schwamm LH. Drip and ship thrombolytic therapy for acute ischemic stroke: use, temporal trends, and outcomes. Stroke. 2015 Mar;46(3):732-9. doi: 10.1161/STROKEAHA.114.007506. Epub 2015 Feb 11.
– Mazya MV1, Lees KR, Markus R, Roine RO, Seet RC, Wahlgren N, Ahmed N; Safe Implementation of Thrombolysis in Stroke Investigators. Safety of intravenous thrombolysis for ischemic stroke in patients treated with warfarin. Ann Neurol. 2013 Aug;74(2):266-74. doi: 10.1002/ana.23924. Epub 2013 Sep 4.
– Zinkstok SM1, Engelter ST, Gensicke H, Lyrer PA, Ringleb PA, Artto V, Putaala J, Haapaniemi E, Tatlisumak T, Chen Y, Leys D, Sarikaya H, Michel P, Odier C, Berrouschot J, Arnold M, Heldner MR, Zini A, Fioravanti V, Padjen V, Beslac-Bumbasirevic L, Pezzini A, Roos YB, Nederkoorn PJ. Safety of thrombolysis in stroke mimics: results from a multicenter cohort study. Stroke. 2013 Apr;44(4):1080-4. doi: 10.1161/STROKEAHA.111.000126. Epub 2013 Feb 26.
– Ganti L. Do Glycoprotein IIb/IIIa Inhibitors Improve Outcomes in Acute Ischemic Stroke? Ann Emerg Med. 2015 Feb 25. pii: S0196-0644(15)00090-6. doi: 10.1016/j.annemergmed.2015.02.002
– Wu TC, Grotta JC. Hypothermia for acute ischaemic stroke. Lancet Neurol. 2013 Mar;12(3):275-84. doi: 10.1016/S1474-4422(13)70013-9. Review.
– Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, Schonewille WJ, Vos JA, Nederkoorn PJ, Wermer MJ, van Walderveen MA, Staals J, Hofmeijer J, van Oostayen JA, Lycklama à Nijeholt GJ, Boiten J, Brouwer PA, Emmer BJ, de Bruijn SF, van Dijk LC, Kappelle LJ, Lo RH, van Dijk EJ, de Vries J, de Kort PL, van Rooij WJ, van den Berg JS, van Hasselt BA, Aerden LA, Dallinga RJ, Visser MC, Bot JC, Vroomen PC, Eshghi O, Schreuder TH, Heijboer RJ, Keizer K, Tielbeek AV, den Hertog HM, Gerrits DG, van den Berg-Vos RM, Karas GB, Steyerberg EW, Flach HZ, Marquering HA, Sprengers ME, Jenniskens SF, Beenen LF, van den Berg R, Koudstaal PJ, van Zwam WH, Roos YB, van der Lugt A, van Oostenbrugge RJ, Majoie CB, Dippel DW; MR CLEAN Investigators. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015 Jan 1;372(1):11-20. doi: 10.1056/NEJMoa1411587
– Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, Roy D, Jovin TG, Willinsky RA, Sapkota BL, Dowlatshahi D, Frei DF, Kamal NR, Montanera WJ, Poppe AY, Ryckborst KJ, Silver FL, Shuaib A, Tampieri D, Williams D, Bang OY, Baxter BW, Burns PA, Choe H, Heo JH, Holmstedt CA, Jankowitz B, Kelly M, Linares G, Mandzia JL, Shankar J, Sohn SI, Swartz RH, Barber PA, Coutts SB, Smith EE, Morrish WF, Weill A, Subramaniam S, Mitha AP, Wong JH, Lowerison MW, Sajobi TT, Hill MD; ESCAPE Trial Investigators. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 2015 Mar 12;372(11):1019-30. doi: 10.1056/NEJMoa1414905
– Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, Yan B, Dowling RJ, Parsons MW, Oxley TJ, Wu TY, Brooks M, Simpson MA, Miteff F, Levi CR, Krause M, Harrington TJ, Faulder KC, Steinfort BS, Priglinger M, Ang T, Scroop R, Barber PA, McGuinness B, Wijeratne T, Phan TG, Chong W, Chandra RV, Bladin CF, Badve M, Rice H, de Villiers L, Ma H, Desmond PM, Donnan GA, Davis SM; EXTEND-IA Investigators. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015 Mar 12;372(11):1009-18. doi: 10.1056/NEJMoa1414792. Epub 2015 Feb 11
– Easton JD, Saver JL, Albers GW, et al. Definition and evaluation of transient ischemic attack. Stroke. 2009;40(6):2276.
– Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet. 2007;369: 283–292
– http://www.ncbi.nlm.nih.gov/pubmed/25805113





4 thoughts on “Stroke and TIA: Pearls and Pitfalls”
Here is something I did to summarize tPA for acute CVA
http://thesgem.com/2014/04/thrombolysis-for-acute-stroke/
And the SGEM Classic review of NINDS with Swami
http://thesgem.com/2014/04/sgem70-the-secret-of-ninds-thrombolysis-for-acute-stroke/
Here is something I did to summarize tPA for acute CVA
http://thesgem.com/2014/04/thrombolysis-for-acute-stroke/
And the SGEM Classic review of NINDS with Swami
http://thesgem.com/2014/04/sgem70-the-secret-of-ninds-thrombolysis-for-acute-stroke/
Pingback: Global Intensive Care | AIR Series: Neurology Module 1 – Bleeds and Strokes
Pingback: Stroke; the best reviews – Poor Evidence