
Authors: Annalee Baker, MD (EM Attending Physician, Aventura Hospital and Medical Center) and Thomas Yang, MD (EM Resident Physician, Aventura Hospital & Medical Center) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
A 75-year-old male with a history of atrial fibrillation on Eliquis presents to the ED with cough, congestion, and abdominal pain. He states that he has had a dry cough for the past seven days. He went to his primary care physician who prescribed azithromycin and Hycodan syrup, but his symptoms have not improved. Last night, the patient developed severe, constant, non-radiating lower abdominal pain. It is not associated with fever, nausea, vomiting, diarrhea, constipation, dysuria, or hematuria. He has taken Ibuprofen 800mg with no relief. The patient denies prior episodes of this pain, and he has no surgical history.
History & Risk Factors
Rectus sheath hematoma (RSH) is a rare cause of abdominal pain that is often overlooked when patients present for evaluation. The disease can mimic almost any other type of abdominal pathology, and thus the diagnosis is frequently delayed.
Though it was first described by Hippocrates and later noted by Galen, it would be 2500 years before a case of rectus sheath hematoma was formally reported in modern medical literature.1,2
As the name implies, the diagnosis is defined as an accumulation of blood in the fibrous sheath surrounding the rectus abdominis muscle. The hematoma arises when there is disruption of the superior or inferior epigastric artery, or a frank tear in the rectus muscle.
Most commonly, such disruption occurs following abdominal surgery or trauma.3 In these instances, the diagnosis may be easier to suspect and diagnose. However, in high-risk populations such as pregnant women and the elderly, rectus sheath hematoma can develop following relatively minor abdominal muscle strain such as occurs with coughing, straining, or defecation, and low clinical suspicion may lead to diagnostic delays. Recent use of antiplatelet and anticoagulant therapy confers additional risk.4,5
Pathophysiology – Know Your Anatomy
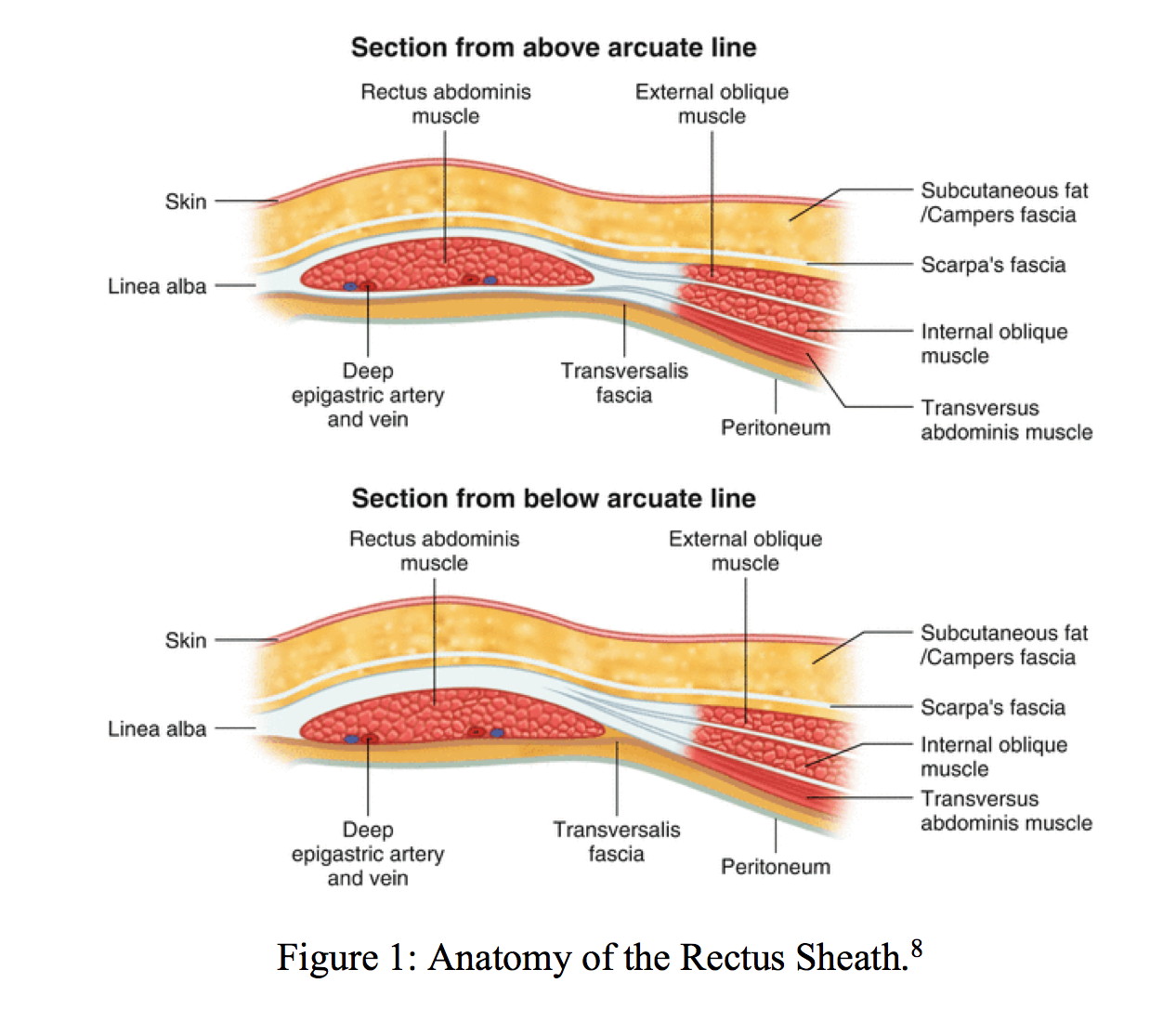
To comprehend the natural history of RSH, an understanding of the relevant anatomy is essential. The rectus abdominis muscles are two parallel, vertically aligned muscles running from ribs 5-7 (superiorly) down to the pubic bone (inferiorly). The rectus muscles and their blood supply are encased inside a fascial sheath, which has varied characteristics along its length.
The defining anatomic boundary within the sheath is the arcuate line, located one-third of the distance from the umbilicus to the pubic symphysis.6 Above this line, aponeuroses of the external oblique, internal oblique, and transversalis muscles form a strong layer of support encasing the rectus muscles. Rectus muscles are further supported and segmented by three or four transverse tendinous intersections (as in “6-pack abs”).6
Below the arcuate line however, two of these aponeuroses pass in front of the muscles, leading to a comparatively weak layer of support posteriorly, and there are no tendinous intersections. The inferior retrorectus space communicates with the prevesicular space of Retzius, generating a direct path for hemorrhage to dissect between the posterior rectus sheath and the bladder.5,6
The superior epigastric arteries arise from the external thoracic arteries and enter the sheath posteriorly near the 7th costal cartilage. The inferior epigastric arteries originate from the external iliac artery at the inguinal ligament and enter the rectus sheath at the arcuate line.6 Around the level of the umbilicus, the superior blood supply joins the inferior arteries in a rich anastomosis.
As the entire vascular network exists posterior to the rectus muscles, hematomas can be difficult to palpate on physical exam. Given the lack of posterior reinforcement inferiorly, injury to the inferior epigastric arteries leads to larger and more extensive hematoma. With no posterior sheath present to tamponade bleeding, an inferior hematoma can quickly cross the midline and dissect down behind the bladder.4,7
RSH occurs when one of these arteries is disrupted by direct trauma or shear forces, which can arise during surgery, external accidental trauma, or excessively vigorous contraction of the rectus muscles (as during valsalva such as coughing, vomiting, or straining to defecate).5,7 Lower quadrant hematomas are more common, and tend to be spherical and bilateral. RSH above the arcuate line is more typically small, spindle-shaped, and unilateral, owing to the strong fascial support and tendinous intersections.
Presentation
Although presentations of RSH vary, abdominal pain is the most common chief complaint (84-97% of cases).4 Patients often describe the pain as sharp, non-radiating, unilateral pain that worsens with movement.
Inferior hematomas may irritate the peritoneum, leading to gastrointestinal symptoms or peritoneal signs. Dissection into the prevesicular space of Retzius may lead the patient to complain of pelvic pain or a pelvic mass, or cite primarily urinary complaints. Indeed, RSH can present with almost any complaint on the spectrum of gastrointestinal and genitourinary disease.4 Depending on the location and severity of disease, patients can even present with shock.9
The key to recognizing RSH lies in suspecting it in the first place. Patient presentation may reveal subtle diagnostic clues, but these will only be elicited if the right questions are asked. Patients may be able to identify a certain RSH-inducing act that occurred prior to the onset of pain. Thus, the patient should be specifically asked about coughing, vomiting, constipation, or vigorous exercise.
A detailed history of any recent trauma or surgery is essential to suspecting RSH in patients with an otherwise obscure presentation. Medication history is critical. Sudden abdominal pain in the setting of anticoagulation should always prompt consideration of RSH.
Based on the history of abrupt onset of pain following violent coughing, and the risk factor of the patient taking Eliquis, the emergency physician includes RSH on her differential diagnosis. The patient’s vital signs are HR 105, BP 145/80, RR 20, T 99.0, O2 98%. He is well-appearing, but clutching his abdomen in pain. The physician examines him fully and performs several specific diagnostic maneuvers to evaluate for RSH. The patient is asked to lift his head off the bed as the physician gently palpates the mass. Following this maneuver, she is even more suspicious of RSH. The medical students look on in awe.
A low-grade fever is common, but vital signs are often normal in RSH. Rarely, a large hematoma with significant hemorrhage may lead to tachycardia or hypotension. Although vital signs abnormalities are nonspecific, they will dictate the degree of initial resuscitation as the differential diagnosis is further explored.5
In addition to pain, many patients describe an abdominal mass, or the mass may be found on exam. As noted above, exam findings in RSH vary by the location of the hematoma, with larger, less circumscribed and often bilateral masses found in the case of inferior hematomas. Cullen’s sign of periumbilical ecchymosis may indicate retroperitoneal or abdominal wall hemorrhage, but these are not specific to RSH.10
In differentiating the mass of RSH from other intra-abdominal pathology, there are two maneuvers which may be helpful. Keep in mind these are not specific for RSH, but rather a mass in the fibrous sheath surrounding the rectus abdominis muscle.
To elicit Fothergill’s sign, the supine patient is asked to lift his/her legs or head while the examiner palpates the mass. If a RSH is present, the mass will become fixed and remain palpable (and tender) as the rectus muscles contract around the hematoma. Intra-abdominal masses will become less distinct as they are palpated through flexed abdominal muscles.11
Carnett’s sign involves a similar maneuver (flexion of the abdominal muscles) but is considered positive if pain is increased or unchanged. If pain is decreased during the maneuver, the mass is likely intra-abdominal.12
Although Fothergill and Cullen signs are negative, the patient clearly has increased pain on flexion of the abdominal muscles, indicating a positive Carnett’s sign. The mass is palpable but indistinct. An IV is started, and appropriate labs are sent. The patient is given IV Morphine, and a CT scan of the abdomen and pelvis with IV contrast is ordered. While waiting for CT, the team performs a bedside ultrasound. Ultrasound confirms the diagnosis, showing a heterogeneous mass beneath the rectus muscles, inferior to the arcuate line. The students, having been instructed in the principles of ALARA, question whether the CT scan is still indicated.
Evaluation
Laboratory Studies
Laboratory studies must include typical abdominal pain labs (CBC, chemistries, hepatic panel, lipase, and urinalysis) but should also include coagulation studies, as both inherited and acquired coagulopathies put patients at risk for RSH.
If the hematoma is large, patients may present with a significant drop in hemoglobin.13 If hemoglobin is normal but an expanding hematoma is suspected, serial hematocrit may aid in diagnosis as well as assess the need for transfusion.14 Leukocytosis may be present but is neither sensitive nor specific.13
Imaging
Although ultrasound is an inexpensive, easy, and safe method to diagnose RSH, it is only 80-90% sensitive, and does not provide information about extent of hemorrhage or alternative diagnoses.5,15,16
CT scan with IV contrast, on the other hand, has sensitivity and specificity approaching 100%, and provides detailed information about hematoma size, location, origin, and extension.4,5,14,16 Ultrasound may still be the screening test of choice in certain populations (pediatrics, pregnancy) and is useful in monitoring hematoma progression.5
Hatjipetrou et al proposed a useful diagnostic algorithm for RSH:5

Although the patient has a classic presentation, with physical exam and ultrasound findings suggestive of RSH, his hematoma is bilateral and inferior to the arcuate line, and the origin and extent of hematoma remain unknown. Additionally, his anticoagulation status puts him at risk for large and extensive disease. Thus, the experienced physician proceeds with CT scan. Lab results show a hemoglobin of 7 mg/dL (baseline 12 mg/dL). CT scan shows a large bilateral hematoma with extension into the prevesical space. The origin of the hemorrhage is unclear. Surgery is consulted, and pRBCs are ordered. The team considers whether to reverse his anticoagulation.

Management
The vast majority of RSH are self-limited and can be treated conservatively.17 Conservative management includes rest, analgesia, management of precipitating factors (ie stool softeners), compression or ice treatment of the hematoma, and if needed, reversal of anticoagulation and fluid resuscitation or transfusion.4,15,18
If a hematoma is small and unilateral, a patient’s pain is controlled, and there is no coagulopathy or hemodynamic compromise, RSH can be managed in the outpatient setting. These patients will require follow up, and hematomas will typically resolve in about a month.19
Hematomas that are large or bilateral, or patients with coagulopathy, hemodynamic compromise, dropping hematocrit, or uncontrolled pain will require admission and close observation. Some patients will require transfusion or surgery, but most patients will do well and be discharged within a few days; their hematomas will resolve over 2-4 months.19
In the most severe cases of RSH, blood extends between the transversalis fascia and the muscle and into the prevesical space. It may even violate the peritoneum. Generally speaking, RSH of this degree occurs in patients taking anticoagulants.7
Thus, these patients are certainly admitted, and often require reversal of anticoagulation and blood transfusion. Still, most remain hemodynamically stable. In a stable patient with a small hematoma that is not expanding, reversal of anticoagulation is not always indicated. The decision to reverse anticoagulation is made clinically, considering patient factors, primarily the size and hemodynamic status of the patient. In patients who become unstable, have rapidly enlarging hematomas, or show evidence of abdominal compartment syndrome, surgery (ligation of bleeding vessels) or interventional radiology procedures (embolization) are required.4,13,18-20
The patient is admitted to the ICU. His Eliquis is held, but not reversed, as he is hemodynamically stable. Serial abdominal exams and CBCs are performed throughout his stay. His hematocrit stabilizes, and his pain is controlled. He is treated with stool softeners and cough suppressants to lower the risk of re-bleeding. Repeat ultrasounds on days 2, 3, and 4 show the hematoma to be unchanged. The patient is discharged on day 5 and instructed to hold his Eliquis and return to surgery clinic for weekly examination and ultrasound. One month later, his anticoagulation is restarted. Three months later, his hematoma has completely disappeared.
Summary
As the population ages, and more patients are taking prescription anticoagulants, it is likely that the incidence of RSH will continue to rise. Emergency physicians must include RSH on the differential of acute abdominal pain with a palpable mass, particularly if predisposing risk factors are present.5 Ultrasound may be a useful screening test, particularly in unstable, pediatric, or pregnant patients, but CT scan should be employed if there is no contraindication.
Clinical factors such as the extent of hematoma, degree of coagulopathy or anemia, and level of hemodynamic compromise should be used to guide management and disposition. IV fluid resuscitation, pain control, and when indicated, reversal of anticoagulation and blood transfusion, should be initiated in the emergency department. All but the smallest hematomas will require admission and surgical consultation, though patients can be reassured that the condition is treatable and most often self-limited.
Reference/Further Reading:
- Manier J.W. Rectus Sheath Hematoma. Am J Gastroenterol. 1972; 57 443-452.
- Richardson SB. Rupture of the Right Rectus Abdominis Muscle from Muscular Efforts: Operation and Recovery, with Remarks. The American Journal of the Medical Sciences. 1857;65(1):41-44.
- Kapan S, Turhan AN, Alis H, et al. Rectus sheath hematoma: three case reports. Journal of Medical Case Reports. 2008;2(1).
- Cherry WB, Mueller PS. Rectus Sheath Hematoma. Medicine. 2006;85(2):105-110.
- Hatjipetrou A, Anyfantakis D, Kastanakis M. Rectus sheath hematoma: A review of the literature. International Journal of Surgery. 2015;13:267-271.
- Netter FH. Atlas of Human Anatomy. Philadelphia: Saunders/Elsevier; 2014.
- Gorsi U. Expect the unexpected: Rectus sheath hematoma comes without a notice. R I Med J (2013). 2017 Nov 1;100(11):39-40.
- Majumder A. Clinical Anatomy and Physiology of the Abdominal Wall. Hernia Surgery. 2016:1-13.
- Ko S-B, Choi HA, Malhotra R, Lee K. Giant Rectus Sheath Hematoma After Therapeutic Paracentesis Resulting in Hemodynamic Instability in the Intensive Care Unit. Hospital Practice. 2010;38(3):52-55.
- Cullen TS. Hemorrhage into or beneath the rectus muscle simulating an acute abdominal condition. Bull Johns Hopkins Hosp. 1937;61:317-348.
- Fothergill WE. Haematoma in the Abdominal Wall Simulating Pelvic New Growth. BMJ. 1926;1(3413):941-942.
- Carnett JB. Intercostal neuralgia as a cause of abdominal pain and tenderness. Surg Gynecol Obstet. 1926;42:625-632.
- Jafferbhoy SF, Rustum Q, Shiwani MH. Abdominal compartment syndrome – a fatal complication from a rectus sheath haematoma. Case Reports. 2012;2012(apr02 1).
- Yamada Y, Ogawa K, Shiomi E, Hayashi T. Bilateral Rectus Sheath Hematoma Developing During Anticoagulant Therapy. Circulation. 2010;121(15):1778-1779.
- Klingler PJ, Wetscher G, Glaser K, Tschmelitsch J, Schmid T, Hinder RA. The use of ultrasound to differentiate rectus sheath hematoma from other acute abdominal disorders. Surgical Endoscopy. 1999;13(11):1129-1134.
- Gallego AM, Aguayo JL, Flores B, et al. Ultrasonography and computed tomography reduce unnecessary surgery in abdominal rectus sheath haematoma. British Journal of Surgery. 1997;84(9):1295-1297.
- Rimola J, Perendreu J, Falcó J, Fortuño JR, Massuet A, Branera J. Percutaneous Arterial Embolization in the Management of Rectus Sheath Hematoma. American Journal of Roentgenology. 2007;188(6).
- Salemis NS, Gourgiotis S, Karalis G. Diagnostic evaluation and management of patients with rectus sheath hematoma. A retrospective study. International Journal of Surgery. 2010;8(4):290-293.
- Berná JD, Garcia-Medina V, Guirao J, Garcia-Medina J. Rectus sheath hematoma: diagnostic classification by CT. Abdominal Imaging. 1996;21(1):62-64.
- Toyonaga J, Tsuruya K, Masutani K, et al. Hemorrhagic Shock and Obstructive Uropathy Due to a Large Rectus Sheath Hematoma in a Patient on Anticoagulant Therapy. Internal Medicine. 2009;48(24):2119-2122.




