
Authors: Sophia Gorgens, MD (EM Resident Physician, Zucker-Northwell NS/LIJ) and Jessica Army, MD (EM Attending Physician, Zucker-Northwell NS/LIJ) // Reviewed by: Marina Boushra, MD; Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
The Case
A 52-year-old woman with known cervical cancer, hypertension, diabetes type II, and atrial fibrillation on apixaban presents to the emergency department (ED) with heavy vaginal bleeding. She was diagnosed with cervical cancer one year ago and has not responded to treatment, with her most recent CT scan showing metastasis to the liver and lungs. The vaginal bleeding started as light spotting two days ago but has gotten steadily heavier. She now endorses using two pads an hour for the past three hours. Additionally, she has experienced dyspnea on exertion and light-headedness. Her triage vitals are temperature 97.9 °F, heart rate 102 bpm, blood pressure 95/50 mm Hg, respiratory rate 18 breaths per minute, oxygen saturation 98% on room air. On physical exam, she is diffusely tender across her lower abdomen. On pelvic exam, the patient’s cervix is not visualized due to blood pooling in the vaginal vault. Bleeding volume obscures view even when forceps with gauze are utilized. No bleeding source can be visualized. What is the most appropriate step in this patient’s care?
Introduction
Cervical cancer is the fourth most common cancer in women, responsible for 6.9% of cancer cases. Despite improvements in diagnostic testing, 604,000 new cases of cervical cancer were diagnosed worldwide in 2020 alone, with over 340,000 deaths per year.1,2 It is a malignancy instigated by human papillomavirus (HPV) 16 and 18 infection.3 Due to increased vaccination rates and improved cervical cancer screening, women from high-income countries often present with early-stage cervical cancer, but for those who present with late-stage disease, the five-year survival rate can be as low as 5-15%.2 For many women who lack access to screening, post-coital bleeding may be the first indication of cervical cancer.4, 5 When post-coital bleeding without hemodynamic compromise is the presenting complaint, the patient requires urgent outpatient gynecological follow-up for diagnostic colposcopy. It is unusual for early stages of cervical cancer to progress to life-threatening bleeding, whereas more advanced disease stages can portend greater volume losses.4, 5 Women who present to the ED with symptomatic cervical cancer with no prior cervical cancer diagnosis are at higher risk for late-stage disease and therefore at higher risk for further complications and death.6
In late-stage cervical cancer, vaginal bleeding is extremely common but difficult to manage and can result in life-threatening hemorrhage.2 In fact, up to 6% of all patients with cervical cancer die from hemorrhagic vaginal bleeding.2 Therefore, vaginal bleeding in these patients should be considered a gynecologic emergency.
Anatomy
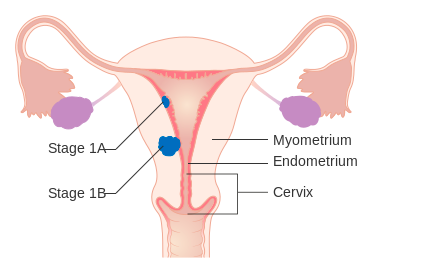
Cervical cancer is staged according to extent of invasion, which will also be informative of the source and potential extent of the bleeding (Table 1). While Stage I cervical cancer is limited to the cervix, Stage II spreads to the vagina and the parametria, Stage III to the lower third of the vagina and the pelvic wall, and Stage IV to the bladder, rectum, or distant organs.6 Early-stage cancer may have cervical cancerous tissue that becomes ulcerated, necrotic, and friable, bleeding spontaneously or on contact and leading to light post-coital bleeding. Conversely, late-stage cancer is likely to have a deeper source of bleeding due to tumor spread past the cervix.6 This means that although vaginal packing may be a temporizing measure, it is unlikely to result in definitive hemostasis in bleeding associated with late-stage cervical cancer. Ligating or embolizing the uterine artery or hypogastric artery, on the other hand, may prove successful. However, as cancer promotes neovascularization, even the neutralization of the uterine or hypogastric artery may not suffice, so radiation oncology, which can target a larger area, may be helpful.

Stabilize the Patient
As with any patient presenting to the ED, the first steps are to assess the patient, focusing on airway, breathing, and circulation. In patients with hemorrhage from cervical cancer, airway and breathing are less likely to be compromised, but patients who are hemodynamically unstable need immediate intervention. Place the patient on the monitor and establish two or more large-bore IV access sites immediately. As with any hemorrhagic condition, transfusion should be targeted to patient need. With advanced-stage cervical cancer as a possible bleeding source, the need for large volume or massive transfusion protocols can arise and should be considered early. This includes a 1:1:1 transfusion of packed red blood cells, platelets, fresh frozen plasma. If the patient is on an anticoagulant, consider the risks and benefits of reversing the medication. While disruption of anticoagulation for patients with atrial fibrillation may be tolerable, for those with high-risk conditions like a mechanical valve it may be more dangerous.7 However, in cases of a hemodynamically unstable patient with a life-threatening bleed, reversing the anticoagulant is critical (table 2).7 Lastly, assess for any other sources of bleeding or alternative sources of hypotension, such as sepsis. As resuscitation is ongoing, the next step is to control the bleed at the source.

Stop the Bleed
There are several temporizing and definitive interventions to consider when attempting to achieve hemostasis in a patient with bleeding from cervical cancer. In the ED, options include vaginal packing, formalin-soaked vaginal packs, kaolin-based hemostatic gauze, and off-label tranexamic acid (TXA).2 As massive hemorrhage is often caused by necrotic tumors which are a nidus for infection, strongly consider the addition of broad-spectrum antibiotics, such as piperacillin-tazobactam, ertapenem, or ciprofloxacin + metronidazole. The addition of vancomycin will cover MRSA, if necessary.8,9
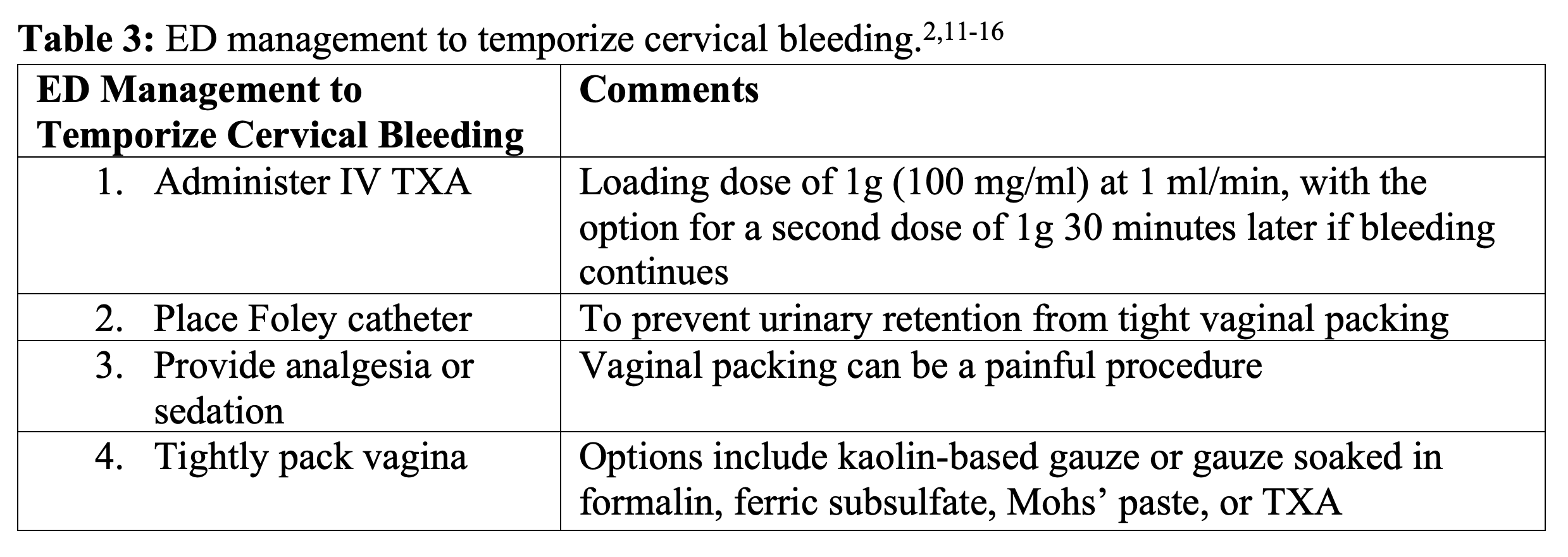
Tight vaginal packing should be done with help of a speculum and with adequate analgesia, including procedural sedation if necessary (Table 3).2 Packing with kaolin-based gauze is preferred as it promotes coagulation.11 If kaolin-based gauze is not available, other options include soaking gauze in formalin (also known as formaldehyde, which causes chemical cauterization and warrants additional pain control), ferric subsulfate (which enhances thrombus formation), and Mohs’ paste (which contains zinc ions to promote hemostasis) (Image 1).2 There is little data on the efficacy of TXA-soaked gauze for vaginal bleeding, though it has been effective in epistaxis and early studies in post-partum hemorrhage are promising.12, 13 One suggested dose for this is soaking gauze in 20 ml of tranexamic acid (1g10ml).12 No matter the choice of material, vaginal packing compresses the urethra, so the patient will require foley placement prior to packing.2

TXA acts by inhibiting the activation of plasminogen and by directly inhibiting plasmin.2 Building off the CRASH-2 trial, which showed a reduced risk of death in bleeding trauma patients who received TXA, the WOMAN trial demonstrated that 1g of intravenous (IV) TXA given to women with postpartum hemorrhage reduced death due to bleeding.14, 15 Therefore, by extrapolation, TXA has been adopted as an adjunct in the treatment of hemorrhage in patients with cervical cancer. For IV use, TXA should be given as a loading dose of 1 g (100 mg/ml) at 1 ml/min.16 A second dose of 1g can be given after 30 minutes if bleeding continues.16 While IV TXA would be preferred in an active hemorrhage, if hemostasis is achieved with packing, oral TXA can be considered for ongoing prophylaxis as this may prolong time to re-bleeding.16 The oral dosing of TXA is up to 1300 mg three times a day.16
Anyone with a bleeding cervical mass requires urgent gynecology/oncology evaluation in the ED. This becomes all the more emergent if attempted interventions fail to control the bleeding as there are several more advanced hemostasis options consultants can offer. Gynecology/oncology may attempt cautery, endoscopic hemostatic forceps, or uterine artery ligation; interventional radiology (IR) may be called for uterine artery embolization; radiation oncology may suggest radiation therapy.2, 17 It is usually best to first call the gynecology team and see which route they recommend.
Goals of Care
Patients with cervical cancer presenting with significant vaginal bleeding often have advanced disease and a poor cancer survival rate. If a goals-of-care discussion has not previously been broached with the patient and their family, it would be appropriate and beneficial to begin that conversation in the ED. This can sometimes be a time-consuming effort but may save the patient unnecessary admission and invasive procedures with limited ability to prolong life. Importantly, when possible, these conversations should be started as early as possible as pain control or anesthesia necessitated by resuscitative procedures can alter the patient’s ability to participate.
Every person has a different view on what type of life is acceptable to them and what level of intervention they wish to pursue. After gathering relevant family members, assess the patient’s understanding of their disease and their options for treatment, palliative care, and hospice (if indicated).18-21 Bring consultants in on the conversation as needed – for example, to discuss certain interventions that they can offer and if that would be in line with the patient’s wishes.16-19 Discuss code status and fill out the necessary paperwork with them. Reassess their understanding and ask what questions they have.18-21
Case Resolution
While waiting for the patient’s type and cross to come back, the patient emergently receives a transfusion of one unit of unmatched pRBCs, and her blood pressure improves to 110/65 mm Hg. Packing the patient’s vagina with gauze achieves temporary hemostasis, and the patient receives 1g IV tranexamic acid. As this is a life-threatening bleed, apixaban is reversed with 4-factor prothrombin complex concentrates (PCC) (Andexanet alfa would be another option if the level of the factor Xa inhibitor is known). While waiting for the gynecology/oncology consultants to arrive in the ED, goals of care are discussed with the patient and her husband. As she has failed multiple rounds of outpatient treatment, the patient asks for a palliative care referral and will additionally consider hospice though she remains full code at this time. The gynecology/oncology team arrives and admits the patient to their service for further hemodynamic monitoring and palliative radiotherapy for hemostasis.
Key Points
-Vaginal bleeding in cervical cancer patients is a common but potentially dangerous presentation and should be treated as a gynecologic emergency, particularly in the advanced stages of disease.
-After stabilizing the patient, attempt to achieve hemostasis via vaginal packing with formalin-soaked vaginal packs or kaolin-based gauze. TXA-soaked gauze can also be considered. This procedure is painful and requires analgesia or procedural sedation as well as placement of a foley catheter.
–Consider giving IV tranexamic acid and broad-spectrum antibiotics, such as piperacillin-tazobactam, ertapenem, or ciprofloxacin + metronidazole. The addition of vancomycin can be utilized to cover MRSA, if necessary.
-Consult the gynecology/oncology team to assess the need for further intervention, which can include surgical uterine artery ligation, uterine artery embolization with IR, or radiotherapy with radiation oncology.
-Patients with cervical cancer presenting with significant vaginal bleeding are often late-stage and discussing goals of care with these patients and their families is critical.
References and Further Reading
- Cervical cancer statistics I world cancer research fund international. WCRF International. https://www.wcrf.org/cancer-trends/cervical-cancer-statistics/. Published April 14, 2022. Accessed August 18, 2022.
- Eleje GU, Eke AC, Igberase GO, Igwegbe AO, Eleje LI. Palliative interventions for controlling vaginal bleeding in advanced cervical cancer. Cochrane Database Syst Rev. 2019;3(3):CD011000. Published 2019 Mar 19. doi:10.1002/14651858.CD011000.pub3
- Zhang S, Xu H, Zhang L, Qiao Y. Cervical cancer: Epidemiology, risk factors and screening. Chin J Cancer Res. 2020;32(6):720-728. doi:10.21147/j.issn.1000-9604.2020.06.05
- Shapley M, Jordan J, Croft PR. A systematic review of postcoital bleeding and risk of cervical cancer. Br J Gen Pract. 2006;56(527):453-460.
- Cohen O, Schejter E, Agizim R, et al. Postcoital bleeding is a predictor for cervical dysplasia. PLoS One. 2019;14(5):e0217396. Published 2019 May 23. doi:10.1371/journal.pone.0217396
- Šarenac T, Mikov M. Cervical Cancer, Different Treatments and Importance of Bile Acids as Therapeutic Agents in This Disease. Front Pharmacol. 2019;10:484. Published 2019 Jun 4. doi:10.3389/fphar.2019.00484
- Farkas, Josh. Anticoagulant reversal. Internet Book of Critical Care. 2021 Sept 25. https://emcrit.org/ibcc/reverse/. Accessed 2022 Aug 24.
- Farkas, Josh. Antibiotics. Internet Book of Critical Care. 2021 June 24. https://emcrit.org/ibcc/antibiotics/. Accessed 2022 Aug 24.
- Nickson, Chris. Antimicrobial Quick Reference. Life in the Fastlane. 2020 Nov 3. https://litfl.com/antimicrobials-quick-reference/. Accessed 2022 Aug 24.
- Maguire FB, Cooley JJP, Morris CR, Parikh-Patel A, Kennedy VA, Keegan THM. Symptomatic presentation of cervical cancer in emergency departments in California. Cancer Causes Control. 2021;32(12):1411-1421. doi:10.1007/s10552-021-01489-z
- Vilardo N, Feinberg J, Black J, Ratner E. The use of QuikClot combat gauze in cervical and vaginal hemorrhage. Gynecol Oncol Rep. 2017;21:114-116. Published 2017 Jul 25. doi:10.1016/j.gore.2017.07.012
- Abdulridha M, Alharoon D, Hassan J. The effectiveness of uterine packing combined with topical tranexamic acid for the management of primary postpartum hemorrhage. The Medical Journal of Basrah University. 2020; 38(2): 104-108.
- Zahed R, Mousavi Jazayeri MH, Naderi A, Naderpour Z, Saeedi M. Topical Tranexamic Acid Compared With Anterior Nasal Packing for Treatment of Epistaxis in Patients Taking Antiplatelet Drugs: Randomized Controlled Trial. Acad Emerg Med. 2018;25(3):261-266. doi:10.1111/acem.13345
- CRASH-2 trial collaborators, Shakur H, Roberts I, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet. 2010;376(9734):23-32. doi:10.1016/S0140-6736(10)60835-5
- WOMAN Trial Collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial [published correction appears in Lancet. 2017 May 27;389(10084):2104]. Lancet. 2017;389(10084):2105-2116. doi:10.1016/S0140-6736(17)30638-4
- Cai J, Ribkoff J, Olson S, et al. The many roles of tranexamic acid: An overview of the clinical indications for TXA in medical and surgical patients. Eur J Haematol. 2020;104(2):79-87. doi:10.1111/ejh.13348
- Alméciga A, Rodriguez J, Beltrán J, et al. Emergency Embolization of Pelvic Vessels in Patients With Locally Advanced Cervical Cancer and Massive Vaginal Bleeding: A Case Series in a Latin American Oncological Center. JCO Glob Oncol. 2020;6:1376-1383. doi:10.1200/GO.20.00239
- Elsayem AF, Elzubeir HE, Brock PA, Todd KH. Integrating palliative care in oncologic emergency departments: Challenges and opportunities. World J Clin Oncol. 2016;7(2):227-233. doi:10.5306/wjco.v7.i2.227
- Saiki C, Ferrell B, Longo-Schoeberlein D, Chung V, Smith TJ. Goals-of-care discussions. J Community Support Oncol. 2017;15(4):e190-e194. doi:10.12788/jcso.0355
- Ouchi K, George N, Schuur JD, et al. Goals-of-Care Conversations for Older Adults With Serious Illness in the Emergency Department: Challenges and Opportunities. Ann Emerg Med. 2019;74(2):276-284. doi:10.1016/j.annemergmed.2019.01.003
- Walker LE, Bellolio MF, Dobler CC, et al. Paths of Emergency Department Care: Development of a Decision Aid to Facilitate Shared Decision Making in Goals of Care Discussions in the Acute Setting. MDM Policy Pract. 2021;6(2):23814683211058082. Published 2021 Nov 13. doi:10.1177/23814683211058082




