
Authors: Elizabeth P. Lanata, MS-IV and Matthew S. Siket, MD, MSc, FACEP (@SiketMD) // Reviewed by: Alexander Y. Sheng, MD, MHPE (@TheShenger); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case
The patient is a 72-year-old male with a past medical history significant for hypertension, diet-controlled type 2 diabetes mellitus, hyperlipidemia, coronary artery disease, and appendectomy who presented to the emergency department (ED) with aphasia and right upper extremity weakness. His symptoms started while he was watching TV earlier that morning and resolved after 15 minutes. The patient experienced similar symptoms of right upper extremity weakness 5 months ago but was not evaluated at that time as his symptoms resolved after 1-2 minutes. Prior to 5 months ago, he had not experienced similar symptoms. The patient is a prior cigarette smoker, 1 PPD for 20 years, quit 15 years ago, and does not use alcohol. He is retired but previously worked as a carpenter. His family history is significant for a father with STEMI at age 67 and stroke at age 78 and a mother with insulin dependent type 2 diabetes mellitus. The patient’s daily medications include lisinopril, atorvastatin, and a baby aspirin.
Follow up questions
- What are the diagnostic imperatives in the ED?
- What is the appropriate disposition? Specifically, when and where does the workup need to be completed, and does this patient require hospitalization?
Introduction
Transient ischemic attack (TIA) is a medical emergency that serves as a warning sign for an impending stroke, with the highest risk of stroke occurring in the first seven days following a TIA.1 In 2009, the American Heart Association/American Stroke Association (AHA/ASA) revised the definition of TIA from a classic time-based definition that existed before the advent of neuroimaging and arbitrarily chose a 24-hour time period, to a tissue-based definition. TIA is currently defined as “a transient loss of neurologic function caused by focal brain, spinal cord or retinal ischemia, without acute infarction.”2 Implied in this modernized definition is the acquisition of neuroimaging to discern focal ischemia from infarct and non-stroke mimics. There remains a lack of consensus as to the optimal disposition from the ED for a patient with suspected TIA. The right answer is often patient and institution-specific and depends upon a combination of short-term stroke risk and access to outpatient care to help determine the underlying cause.
Epidemiology and Pathogenesis
The incidence of TIA in the United States is estimated to be 200,000-500,000 per year, with a prevalence of 5 million individuals, but is likely underreported.2 Stroke is preceded by TIA in 12-30% of patients and is the 5th leading cause of death in the US, contributing significantly to long term disability.2,3 Strokes occur more commonly in men than women, but women experience more severe morbidity.2,3 Stroke prevalence increases with age and occurs more frequently in black and Hispanic populations.3 It should also be noted that 90% of strokes worldwide occur in the setting of potentially modifiable risk factors which presents an incredible opportunity for early intervention, especially following TIA.2
TIA and stroke most commonly result from thrombotic or embolic complications of atherothrombotic disease.2 Stroke symptoms occur due to a focal area of neuronal hypoperfusion leading to oligemia, impaired oxygen and glucose metabolism and eventual ischemia and infarction.2,3 When an etiology is discovered, stroke is most commonly caused by three distinct categories – large vessel disease, small vessel disease or cardioembolic, though cryptogenic (defined as stroke of undetermined etiology) causes account for 25-50% of ischemic events.3 The most common etiology for large vessel disease is longstanding hypertension, whereas cardioembolic events can be due to atrial dysrhythmias (atrial fibrillation is most common and carries a 0.2%-23.6 % risk of stroke annually), valvular disease, left ventricle thrombi and right-to-left shunts.2
Diagnostic Approach
History is a key component in evaluation of suspected TIA and essential in ruling out common non-ischemic mimics. TIA mimics include, but are not limited to hypoglycemia, complicated migraine, seizure with or without Todd’s paralysis, intracranial mass lesion, neuropathy, acute vestibular syndrome, demyelinating disease, metabolic disarray, and psychogenic causes.3 Initial serologic work up should be aimed at differentiating true TIA from mimics and generally include blood glucose, CBC, electrolytes and coagulation studies (PT/INR, PTT). Although recommended by the AHA/ASA as a part of the routine TIA workup, coagulation studies are usually low yield unless the patient is young and without apparent vascular etiology3. None the less, they should be ordered to complete the workup and identify potential underlying coagulopathies.
History
The history of present illness should describe a transient episode of abrupt focal neurological dysfunction. When delineating details of the event it may be helpful to have the patient discern “negative symptoms” from “positive symptoms.” Negative symptoms are those associated with a loss of normal neurological function and are more indicative of ablative phenomena such as ischemia. Alternatively, positive symptoms describe irritative phenomena, which are less likely to be ischemic in origin, and are characterized by the addition of a new symptom (such as tingling instead of numbness, or visual flashes/floaters instead of vision loss).3 One notable exception is dizziness, which can be both a positive and negative symptom (loss of normal vestibular function and onset of new vertiginous feeling). Dizziness is a symptom of posterior circulation ischemia but has only been associated with TIA or stroke in 3.2% of patients reporting the symptom, and only 0.7% of patients without other signs and symptoms.3 Majority of TIAs are brief, with 60% lasting less than 1 hour.3 History should also investigate co-morbidities which put patients at an increased risk of developing TIA or stroke, including hypertension, hyperlipidemia, carotid stenosis, advanced age, prior TIA or stroke.3
Physical Exam
Patients suspected of having a TIA should receive a full neurological exam, which includes cranial nerves, strength and sensation, visual fields, language, gait, and coordination.2,3 Focal neurological deficit on exam should raise suspicion for TIA and stroke. In additional to a complete neurological exam, it is important to auscultate the carotids to assess for bruit that could be indicative of carotid stenosis as well as perform a thorough cardiac exam, listening closely for murmurs and irregular rhythms.3
Neuroimaging
Neuroimaging should be considered a high priority in patients with suspected TIA and stroke, and as a general rule should always be obtained at the point of first contact with a patient following a suspected event.4 Patients experiencing ongoing symptoms should be considered as having a stroke until proven otherwise. Emergent non-contrast head computed tomography (NCHCT) should be performed to assess for early ischemic signs and to rule out intracerebral hemorrhage (ICH).2 NCHCT has a low sensitivity in TIA and is usually normal.2 If negative for intracranial hemorrhage and mass lesion, CT angiography should be added to visualize the intra- and extra-cranial cervicocephalic vessels searching for large vessel occlusion.2 Magnetic resonance angiography (MRA) is a reasonable alternative to CTA for vessel visualization but requires additional time and lacks widespread availability.2 If CTA is negative for large vessel occlusion and TIA is suspected, MRI should be obtained to evaluate for signs of ischemia/infarct.2 The diffusion weighted imaging (DWI) sequence on a noncontrast MRI is the gold standard for the diagnosis of acute ischemic stroke and reliably distinguishes stroke from TIA.2 DWI identifies areas of focal cytotoxic edema formation by appearing as bright white spots.2 These areas are generally confirmed as acute stroke if they also appear dark on the corresponding Apparent Diffusion Coefficient (ADC) sequence.2
Risk Stratification and Proposed Management
Timely diagnosis of TIA can reduce subsequent stroke risk through early etiologic determination and initiation of secondary prevention strategies.5 A 2017 study published in by the American Academy of Neurology demonstrated that 20% of ischemic strokes are preceded by TIA in the hours to days prior to stroke onset, and that up to 80% of strokes following TIA are preventable.6 Some have suggested that all patients presenting with TIA should be admitted for further risk stratification, but admission alone has not been shown to reduce the risk of subsequent stroke.1 An expedited diagnostic evaluation can often be performed in the outpatient setting with much of it initiated from the ED.7 The question then becomes: which patients are appropriate for an expedited outpatient evaluation and in whom is hospitalization favored? This is when risk stratification tools can be (somewhat) helpful.
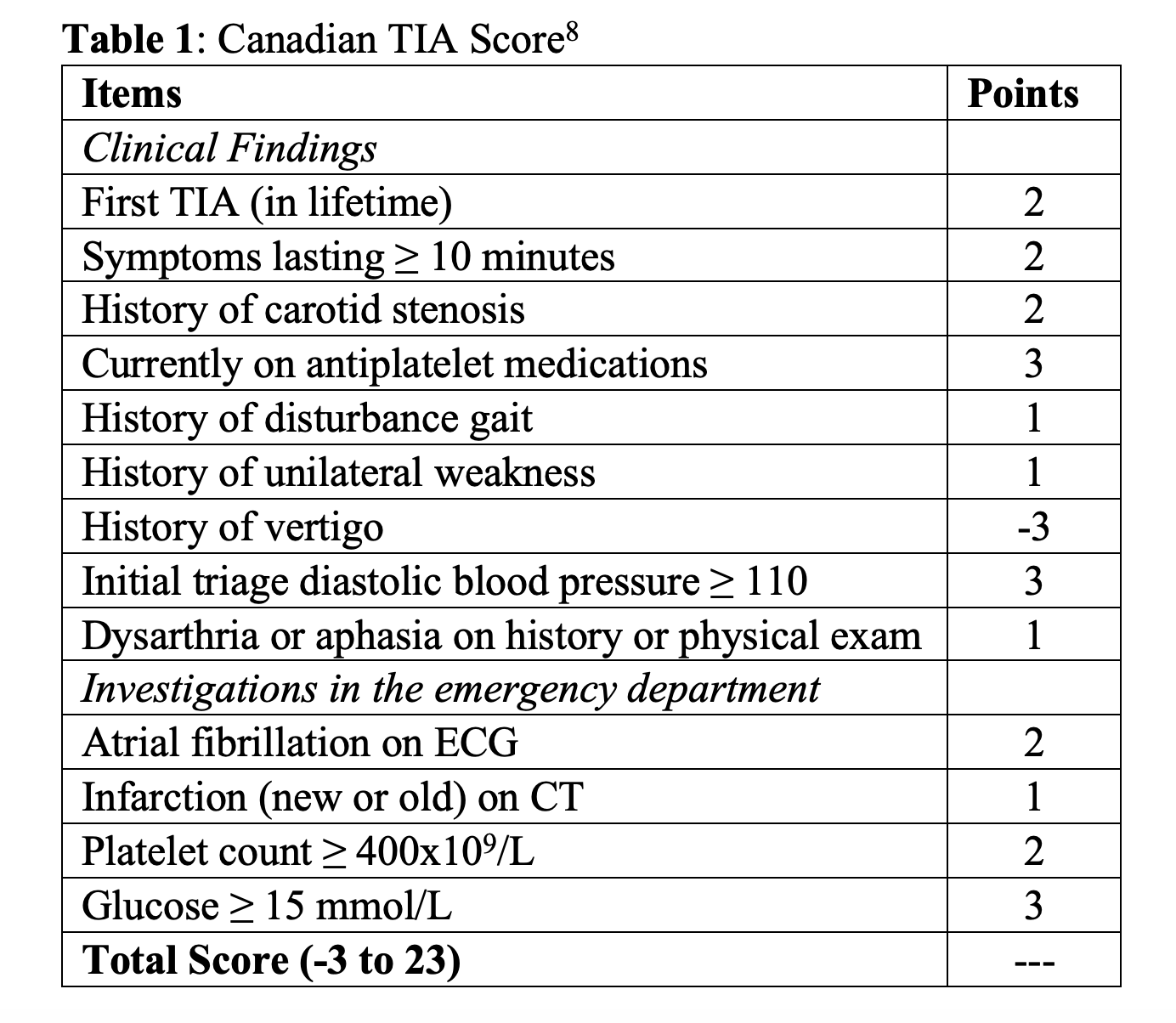
Risk stratification tools, most notably the ABCD2 score, are commonly used to identify patients’ risk of subsequent stroke following a TIA. The ABCD2 score allots points for risk factors including age, blood pressure, and diabetes, as well as certain clinical features (speech disturbance and unilateral weakness) and duration of symptoms.8 Its predictive ability is modest and is outperformed by other tools that incorporate additional high-risk clinical and imaging criteria such as the ABCD2-I and ABCD3-I scores.9,10 Imaging-enhanced scores such as these are of limited practical utility in resource-limited settings, as they require advanced brain and vascular imaging in order to complete. Alternatively, the Canadian TIA score stratifies patients into minimal, low, high, or critical risk categories that correlate with the probability of developing a stroke in the week following a TIA using only variables that are routinely obtained in the ED setting (Table 1).1 Suggested work up is based on that risk. Utilization of the Canadian TIA Score strikes a balance that allows for risk stratification based on history, clinical data points, and neuroimaging and defines clear follow up based on the patient’s predictive score. When compared to the ABCD2 score, the Canadian TIA Score showed better predictability with c-statistics of 0.64 and 0.77 respectively.1
The Canadian TIA score risk stratifies patients using a total of 13 components, 9 relating to the clinical history and exam and 4 derived from clinical investigations, including neuroimaging obtained in the emergency setting. The score ranges from -3 to 23 with a probability of subsequent stroke within 7 days of TIA ranging from 0.01% to >27.6%.1 The probability of subsequent stroke within 7 days of TIA diagnosis is shown in Table 2.1 A recent study, surveying 131 emergency physicians in Canada, found that greater than 75% of those surveyed classified patients as minimal risk if the probably of 7 day stoke was less than 1%, low risk probability 1%-4.9%, high risk 5-10% and critical risk as those with a probability greater than 10%.8

The proposed work up was based on clinical risk and was as follows:8
- Minimal Risk: Obtain an ECG today, obtain CT brain imaging as outpatient, image carotid arteries as outpatient, obtain echocardiogram as outpatient, outpatient holter cardiac monitoring
- Low Risk: Obtain ECG today, image carotid arteries as outpatient, obtain echocardiogram as outpatient, outpatient holter cardiac monitoring
- High Risk: Obtain ECG today, obtain CT brain imaging today, cardiac monitoring for at least 2 hours today
- Critical Risk: Obtain ECG today, obtain brain CT imaging today, image carotid arteries today, obtain echocardiogram today, cardiac monitoring for at least 2 hours today
Greater than 75% of surveyed physicians also proposed the following risk modification guidelines based on risk category. In addition to antiplatelet therapy, either maintaining current antiplatelet or starting acetylsalicylic acid (ASA), the following risk modifications were suggested by greater than 75% of surveyed physicians:8
- Minimal and Low Risk: Refer patient to rapid outpatient assessment with neurologist
- High Risk: Start or switch antiplatelet to clopidogrel or dipyridamole + ASA, start or optimize control of hypertension, refer patient to neurology today
- Critical Risk: Start or switch antiplatelet agent to clopidogrel or dipyridamole + ASA, start oral anticoagulation if in atrial fibrillation, start statin class medication, start or optimize control of hypertension, admit patient to the hospital with referral to neurology today
It should be noted that risk prediction scores should be utilized in conjunction with the larger clinical picture and should not alone dictate which patients with TIA can be safely discharged from the ED. Regardless of risk stratification, almost all patients with TIA warrant a front-loaded work up to reduce the risk of subsequent stroke.
As an alternative to the binary decision of admission vs discharge, some hospital systems offer the option of specialized TIA clinics or ED observation units, which serve as safe and efficient alternatives to hospital admission for many patients with TIA.3 Observation units allow for a full TIA work up directly after presentation to the ED, which avoids the need for admission to further complete the workup as well as decreases ED congestion.3 Recent studies have shown that the utilization of observation units for patients presenting with a suspected TIA can decrease the hospital admission rate in this group by more than 80% without compromising patient safety.7 TIA clinics, which provide 24/7 TIA evaluation by neurologists, offer an additional safe and cost-efficient alternative to admission. According to a 2013 study by Martinez-Martinez et all, TIA clinics can provide efficient evaluation and care at one fifth of the cost of hospitalization.7 These alternatives to the traditional admit vs discharge allow for prompt evaluation of potential etiologies and risk factors, expedited work up and decreased overall hospital expenses associated with admission.
Limitations of Canadian TIA Score
Although the Canadian TIA Score was shown to have superior risk predictability when compared to the ABCD2 score, the Canadian TIA Score has not yet been validated.11 Risk stratification score alone should not be used to determine disposition. Rather, the decision regarding admission vs. discharge should be made within the greater clinical context.
Case Conclusion
Additional Information
Upon presentation to the ED, vital signs included T37, HR82, BP134/78, RR16, SPO2 97% on RA. He is currently asymptomatic in the ED. ECG demonstrated sinus rhythm, rate of 84, no ST segment elevations, depressions, or T wave abnormalities. There was no hemorrhage or infarct noted on NCHCT, and CTA revealed no areas of significant vessel stenosis. CBC and electrolytes were within normal limits and blood glucose was 134.
Utilizing the Canadian TIA Score, this patient has a score of 9 (symptoms > 10 minutes, history of carotid stenosis, already taking antiplatelet therapy, history of unilateral weakness, aphasia), which puts his probability of having a stroke within the next 7 days at 3.2% and in the “low risk” category on risk stratification.
Given this risk stratification, outpatient risk reduction methods should include referral to rapid outpatient assessment with a neurologist, as well as outpatient echocardiogram and cardiac event monitoring.
American College of Emergency Physicians TIA Clinical Policy
In a 2016 systemic review of the TIA literature, the American College of Emergency Physicians (ACEP) developed a clinical TIA policy in which it aimed to provide clinical recommendations developed from an evidence-based review. In concordance with our recommendations, the policy suggests a level B recommendation stating that physicians not rely entirely on risk stratification tools to determine disposition.11 It states that the ABCD2 scores lack sufficient diagnostic accuracy in predicting short-term risk of stroke following TIA and although the Canadian TIA score demonstrates superior predictability, it has not yet been validated.11 Thus, risk stratification scores cannot be used in isolation when determining a safe disposition.
The policy also attempts to answer the question of what imaging needs to be completed in the ED setting and what imaging can be safely delayed. It makes a class C recommendation stating that an initial NCHCT can identify some of the common TIA mimics, but cannot reliably predict early stroke in those presenting with suspected TIA.11 While it is accurate that a NCHCT does not reliably predict the short-term risk of subsequent stroke in those presenting with TIA symptoms, emergent brain imaging must be obtained to rule out the possibility of ongoing stroke. This level C recommendation also states that DWI and cervical vascular imaging do predict short-term risk for stroke in patients presenting with TIA and that obtaining a carotid ultrasound can be used to exclude severe carotid stenosis with similar accuracy to MRA or CTA.11
The policy concludes with a level B recommendation suggesting the utilization of a rapid ED-based diagnostic protocol to evaluate short-term risk of stroke in patients without high-risk conditions presenting with suspected TIA.11 In this group of patients, a rapid diagnostic protocol is equivalent to admission in terms of patient safety and is associated with decreased hospital costs and length of stay.11
In alignment with these recommendations, we propose the utilization of a front-loaded work up, much of which can be initiated in the ED, and risk stratification tools, namely the Canadian TIA Score utilized within the greater clinical picture, to assist disposition.
Summary Points
- Timely workup and treatment can minimize the risk of developing a subsequent stroke following TIA and much of this work up can be initiated from the ED
- The Canadian TIA Score combines clinical history and exam finding with neuroimaging to risk stratify patients and better predict the probability of stroke occurring within 7 days of TIA; this risk stratification can help to guide the where and when of the TIA work up
- Risk Stratification scores alone cannot be used to determine disposition and must be utilized within the larger clinical context
- Regardless of risk stratification score, all patients with TIA should have a front-loaded work up to decrease potential stroke in the subsequent weeks to months following a TIA (know the pros and limitations of the clinical system you work in)
References
- Perry JJ, Sharma M, Sivilotti ML, et al. A Prospective Cohort Study of Patients With Transient Ischemic Attack to Identify High-Risk Clinical Characteristics. Stroke. 2013;45(1):92-100 doi:10.1161/strokeaha.113.003085.
- Siket MS, Edlow J. Transient ischemic attack: an evidence-based update. Emerg Med Pract. (2013) 15:1–26.
- Siket M, Marcolini E. Transient Ischemic Attack and Acute Ischemic Stroke. CorePendium. https://www.emrap.org/corependium/chapter/recEAr4nPXQE4eOBH/Transient-Ischemic-attack-and-Acute-Ischemic-Stroke.
- Easton JD, Saver JL, Albers GW, et al. Definition and Evaluation of Transient Ischemic Attack. Stroke. 2009;40(6):2276-2293. doi:10.1161/strokeaha.108.192218.
- Jarhult SJ, Howell ML, Barnaure-Nachbar I, Chang Y, White BA, Amatangelo M, Brown DF, Singhal AB, Schwamm LH, Silverman SB, Goldstein JN. Implementation of a Rapid, Protocol-based TIA Management Pathway. West J Emerg Med. 2018 Mar;19(2):216-223. doi: 10.5811/westjem.2017.9.35341. Epub 2018 Feb 8. PMID: 29560046; PMCID: PMC5851491.
- Coutts SB. Diagnosis and Management of Transient Ischemic Attack. Continuum (Minneap Minn). 2017;23(1, Cerebrovascular Disease):82-92. doi:10.1212/CON.0000000000000424
- Mijalski C, Silver B. TIA Management: Should TIA Patients be Admitted? Should TIA Patients Get Combination Antiplatelet Therapy? Neurohospitalist. 2015 Jul;5(3):151-60. doi: 10.1177/1941874415580598. PMID: 26288673; PMCID: PMC4530421.
- Perry JJ, Losier JH, Stiell IG, Sharma M, Abdulaziz K. National survey of emergency physicians for transient ischemic attack (TIA) risk stratification consensus and appropriate treatment for a given level of risk. CJEM. 2016 Jan;18(1):10-8. doi: 10.1017/cem.2015.57. Epub 2015 Jul 31. PMID: 26226855.
- Merwick A, Albers GW, Amarenco P, Arsava EM, Ay H, Calvet D, Coutts SB, Cucchiara BL, Demchuk AM, Furie KL, Giles MF, Labreuche J, Lavallée PC, Mas JL, Olivot JM, Purroy F, Rothwell PM, Saver JL, Sheehan OC, Stack JP, Walsh C, Kelly PJ. Addition of brain and carotid imaging to the ABCD² score to identify patients at early risk of stroke after transient ischaemic attack: a multicentre observational study. Lancet Neurol. 2010 Nov;9(11):1060-9. doi: 10.1016/S1474-4422(10)70240-4. Epub 2010 Oct 11. PMID: 20934388.
- Giles MF, Albers GW, Amarenco P, Arsava MM, Asimos A, Ay H, Calvet D, Coutts S, Cucchiara BL, Demchuk AM, Johnston SC, Kelly PJ, Kim AS, Labreuche J, Lavallee PC, Mas JL, Merwick A, Olivot JM, Purroy F, Rosamond WD, Sciolla R, Rothwell PM. Addition of brain infarction to the ABCD2 Score (ABCD2I): a collaborative analysis of unpublished data on 4574 patients. Stroke. 2010 Sep;41(9):1907-13. doi: 10.1161/STROKEAHA.110.578971. Epub 2010 Jul 15. PMID: 20634480.
- Lo BM, Carpenter CR, Hatten BW, et al. Clinical Policy: Critical Issues in the Evaluation of Adult Patients With Suspected Transient Ischemic Attack in the Emergency Department. Annals of Emergency Medicine. 2016;68(3). doi:10.1016/j.annemergmed.2016.06.048.




