Author: Maryam Abdrabbo, PharmD Candidate 2018 (Rutgers Ernest Mario School of Pharmacy, New Brunswick NJ), Cynthia Santos, MD (Assistant Professor Emergency Medicine, Medical Toxicology, Rutgers NJMS) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital), and Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX)
Case:
A 19-year-old woman is brought into the ED by family members after she reported ingesting 35 Tylenol tablets (Extra-Strength) 2 hours ago. She complains of nausea and vomiting and admits this was an attempt to harm herself. Her weight is 54 kg.
Clinical Pearls:
Acetaminophen (APAP) comes in different strengths and formulations.
- There are immediate- and extended-release formulations.
- IR – majority is absorbed within 2 hours.1
- ER – majority is absorbed within 4 hours.1
- Therefore, one can assume for all ingested formulations (whether IR or ER), most APAP is absorbed at 4 hours.1
- The time to peak may be extended by coingestion of opiods or anticholinergics.
- Regular-Strength (IR) = 325mg
- Extra-Strength (IR) = 500mg
- Arthritis Pain 8HR (ER) = 650mg
Many OTC combination products contain acetaminophen!
- This can be one of the causes for chronic APAP toxicities.
- Examples include cough and cold products, migraine medications (which also could contain aspirin like Excedrin® Migraine), etc.
Acute vs. Chronic APAP Ingestion1
- Acute overdose is arbitrarily defined as an entire ingestion within a single 8-hour period.
- Chronic overdose occurs with repeated supratherapeutic ingestions (greater than an 8-hour period).
Toxic Dose1
- Acute ingestion (< 8 hours)
- Adults: 7.5 g
- (Note: more likely to see doses >12 g cause toxicity)
- Children: 150 mg/kg
- (Note: more likely to see doses >200 mg/kg cause toxicity)
- Adults: 7.5 g
- Chronic ingestion (> 8 hours)
- Adults
- 24-hour period
- 200 mg/kg or 10 g (whichever is less)
- 48-hour period
- 150 mg/kg/day or 6 g/day (whichever is less)
- Children
- 100 mg/kg/day over 72 hour period or greater
- Adults
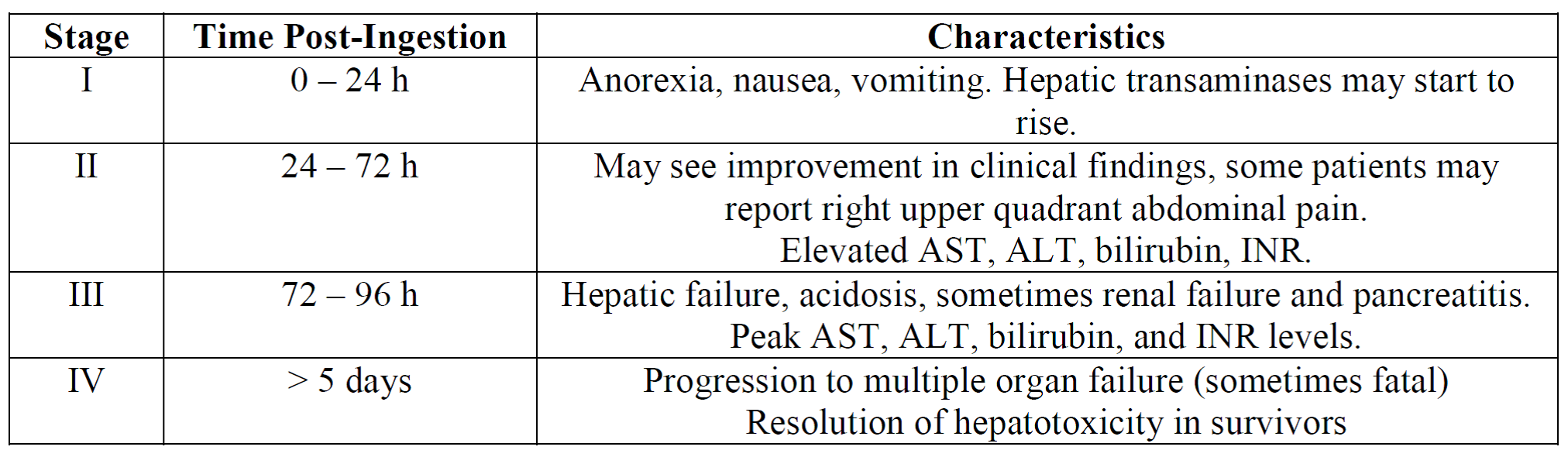
Stages of Acute Acetaminophen Poisoning1,3
Getting APAP Levels1
- Pre-4 hour vs 4-hour level
- Getting an APAP level 1 to 4 hours after ingestion may be helpful only to exclude ingestion of APAP (that is, if the level is zero).
- Obtain a 4-hour level (or later, up to 24 hours) to get estimated peak absorption (that is, if time of ingestion is certain).
When to Initiate Treatment:
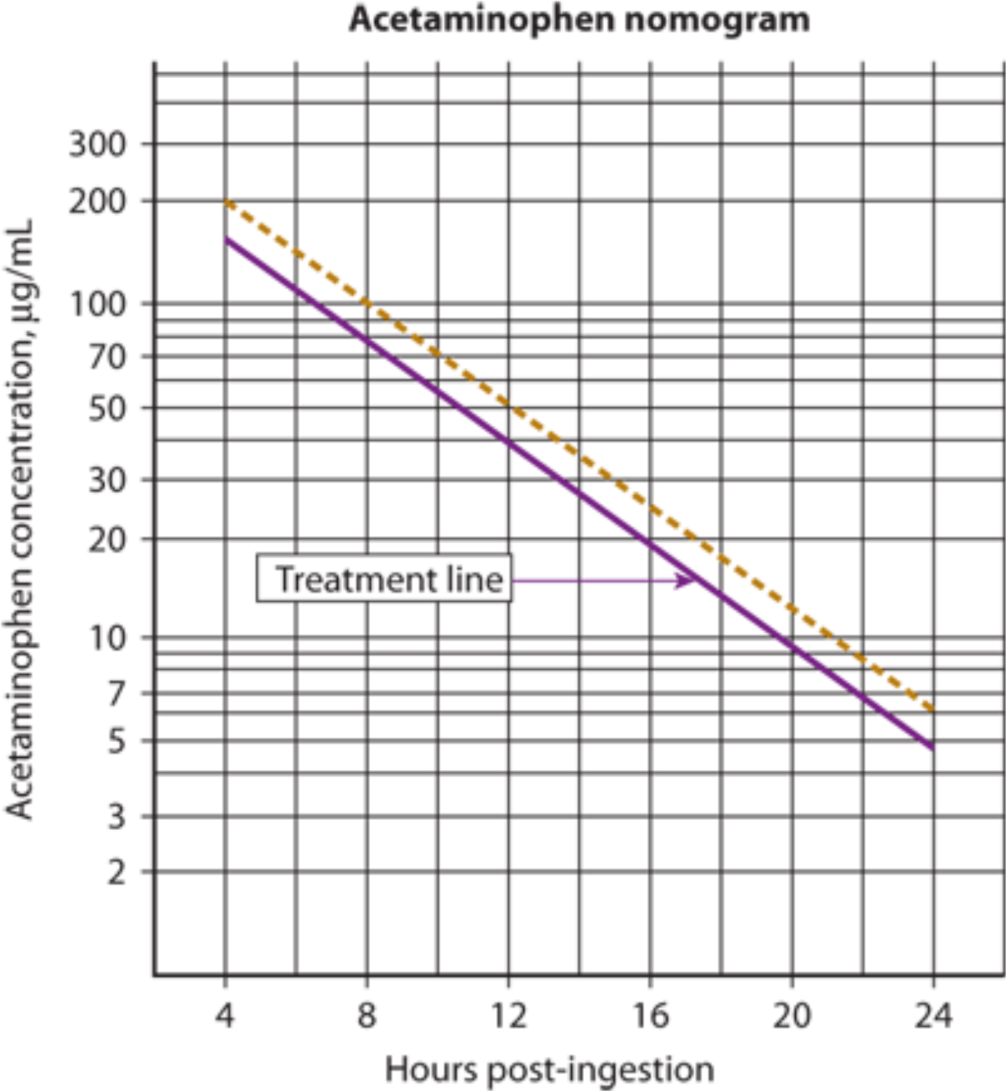
Figure 1. Rumack-Matthew Nomogram for Acetaminophen1
Using APAP Rumack-Matthew Nomogram
- The Rumack-Matthew nomogram is used to determine the risk of APAP-induced hepatoxicity after a single acute ingestion only (not for chronic or repeated ingestions).
- Serum concentrations above the treatment line indicate the need for N-acetylcysteine (NAC) therapy.
- The treatment line starts at 150 mcg/mL at 4 hours post-ingestion.
- Remember, majority of APAP absorption occurs by 4 hours (this may not be true with overdose).
Determining Hepatotoxicity Risk if Nomogram Isn’t Applicable
- If time of ingestion is unknown or if ingestion spans more than 24 hours: Screen with labs (APAP concentration, hepatic function tests, renal function tests, coagulation studies, blood gas), assess patient risk factors and clinical features.1,3
- If ASTs are elevated = treat with NAC
- If [APAP] is detectable = treat with NAC
- If [APAP] is undetectable and ASTs are normal = NAC is unnecessary
- If lab testing shows progressive hepatic failure or continued detection of [APAP] = continue NAC (this implies repeat testing).
Laboratory Assessment:
- APAP Levels
- Assess Labs for Hepatic Injury
- Get initial and daily LFTs
- If progressive hepatic failure, obtain LFTs every 12 hours
- PT, INR
- pH (Metabolic acidosis)
- SCr (Toxic APAP metabolites can also affect CYP enzymes in the kidney)
- Get initial and daily LFTs
- Continue Lab Monitoring
This patient plots above the “150-line” at 4 hours on the nomogram for her single ingestion acute overdose. She should be started on NAC. Continue monitoring the patient’s labs.
Treatment:
- GI decontamination
- Generally not useful due to rapid APAP absorption
- Activated charcoal may be useful if administered early on or if suspected co-ingestants
- Supportive care
- Nausea, vomiting, acidosis, hepatic or renal failure
- Antidotal therapy with N-Acetyl Cysteine (NAC)
- Best and most effective option!
N-Acetyl Cysteine (NAC) Therapy1,2
Mechanism of Action:
- The non-toxic route of APAP metabolism gets saturated in overdoses, which leads to the formation of the toxic metabolite NAPQI.
- NAC helps replenish glutathione stores to conjugate the toxic metabolite, and assists with other routes of liver metabolism as well. See Figure 2 below.
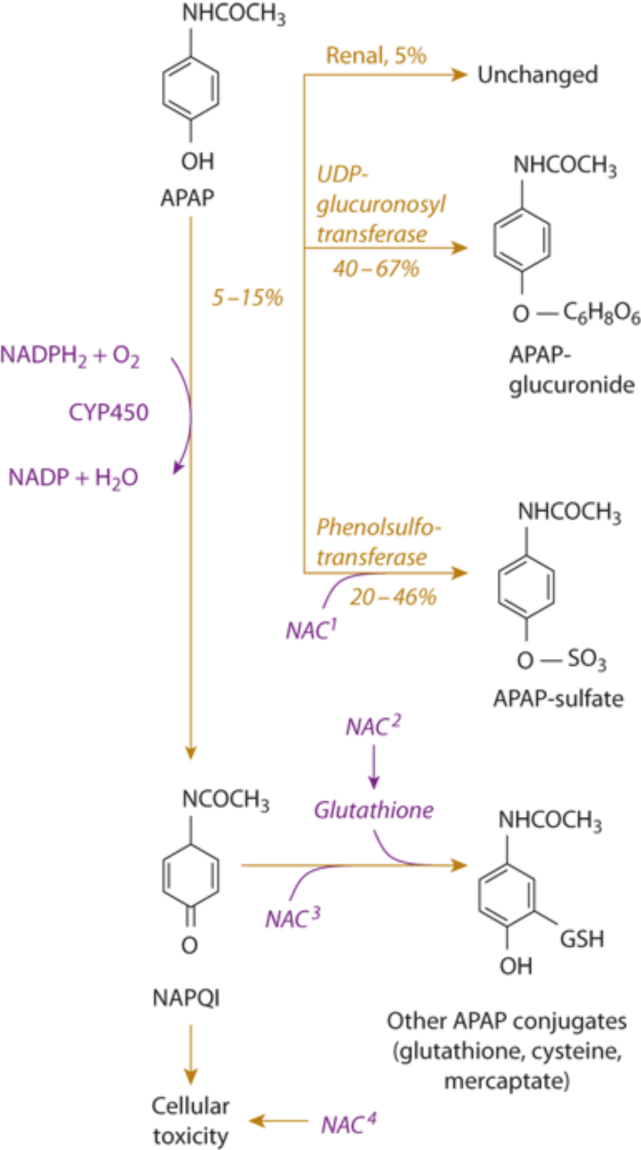
Figure 2.1 NAC has a hepatoprotective effect. NAC augments sulfation, NAC2 is a glutathione (GSH) precursor, NAC3 is a GSH substitute, and NAC4 improves multiorgan function during hepatic failure and possibly limits the extent of hepatocyte injury.
NAC Dosing:1,2
Treatment should begin within 8 hours of ingestion or as soon as possible after ingestion.
- Oral (Mucomyst®):
- 72-hour regimen: Consists of 18 doses
- Loading dose: 140 mg/kg
- Maintenance dose: 70 mg/kg every 4 hours for 17 additional doses
- Repeat dose if emesis occurs within 1 hour of administration
- 72-hour regimen: Consists of 18 doses
- IV (Acetadote ®):
- 21-hour regimen: Consists of 3 components
- Loading dose: 150 mg/kg infused over 1 hour
- Second dose: 50 mg/kg infused over 4 hours
- Third dose: 100 mg/kg infused over 16 hours
- 21-hour regimen: Consists of 3 components
Note: It is highly recommended to consult with a poison control center or medical toxicologist when considering the discontinuation of acetylcysteine prior to the conclusion of a full course of therapy.
Liver Transplant1
King’s College Criteria for predicting the need for hepatic transplant:
- Serum pH < 7.3 or lactate > 3 mmol/L after fluid resuscitation
OR
- All of the following:
- SCr > 3.3 mg/dL
- PT > 100 sec (or INR > 6.5)
- Grade III or IV encephalopathy
Main Point:
- For patients with acute APAP overdoses, use the Rumack-Matthew Nomogram.
- Plot a single [APAP] onto the nomogram.
- If the [APAP] plots above the treatment line, or “150-line”, treat with NAC.
- For patients with chronic APAP overdoses (repeated supratherapeutic ingestions), treat with NAC if:
- ASTs are elevated OR [APAP] is detectable.
- Use the King’s College Criteria for evaluating the need for hepatic transplantation.
- NAC shouldn’t be given as a set length protocol. An informed decision should be made when stopping NAC, which requires assessing that the risk of developing toxicity is low ([APAP] is undetectable, ASTs are normal), and any toxicity that occurred has been resolved.
References:
- Hendrickson RG. Acetaminophen. In: Goldfrank’s Toxicologic Emergencies 9th edition. Nelson LS, et al (Eds). New York, NY, McGraw-Hill 2011.
- Acetylcysteine [monograph]. In: Lexicomp Online [online database]. Hudson, OH: Lexi-Comp (Accessed 2017 Aug 22).
- O’Malley GF., Kimmel S, O’Malley R. “Acetaminophen Poisoning.” Merck Manuals Professional Edition. https://www.merckmanuals.com/professional/injuries-poisoning/poisoning/acetaminophen-poisoning. (Access 22 Aug 2017).
- EXTRIP. “Acetaminophen (APAP) Poisoning.” The Extracorporeal Treatments In Poisoning Workgroup. http://www.extrip-workgroup.org/acetaminophen. (Accessed 22 Aug 2017).





1 thought on “TOXCard: Acetaminophen Toxicity and Management”
Pingback: Paracetamolintox – Mind palace of an ER doc