Authors: Theresa Dao, MD, Anthony Scoccimarro, MD and Muhammad Waseem, MD, MS (Lincoln Medical & Mental Health Center, Bronx, New York) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Stephen Alerhand, MD (@SAlerhand)
Trauma is the leading cause of death in pregnant women from causes unrelated to the pregnancy2. Trauma affects 7% of all pregnancies3,4 and greater than 50% of trauma occurs during the third trimester. The most common causes of these traumas are related to motor vehicle collision, penetrating trauma, domestic violence, and suicide2. Emergency department management of such women requires special considerations due to the changes in their anatomy and physiology. Here we will discuss the changes expected in pregnancy, how to interpret them, and what changes are recommended for successful trauma resuscitation.
Anatomical and Physiological Variations
As with all trauma patients, the ABCs remain critical during the initial evaluation and assessment
AIRWAY
There are several physiological changes secondary to hormonal and mechanical effects:
–Increased laryngeal edema secondary to water retention2
–Lingual mucosa thickening secondary to capillary engorgement2
-Larynx becomes more anteriorly displaced due to the elevation of the diaphragm2
–Increased rates of hypoxia and decompensation => consider early high O2 flow
-Hypoxia to the mother => increased fetal hypoxia7
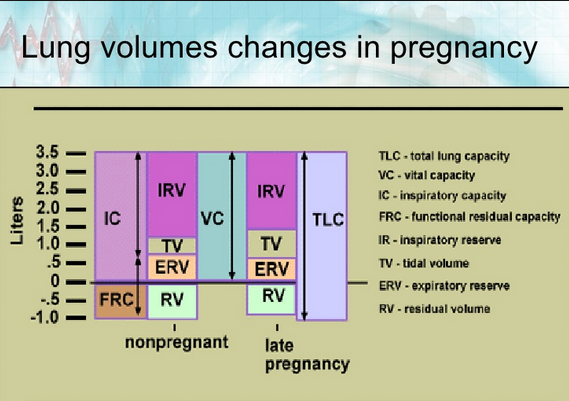
BREATHING
-Gravid uterus => Increased intra-abdominal pressure => Elevated hemidiaphragm => Decreased functional residual capacity by 20%7
-Gravid uterus => Increased intra-abdominal pressure => Decreased Chest wall compliance
-Increased progesterone levels => Decreased lower esophageal sphincter tone => Increased aspiration risk
-Consider antiemetic and early intubation to reduce complications
 Chukwuma, I. Onyeije MD, Morehouse School of Medicine
Chukwuma, I. Onyeije MD, Morehouse School of Medicine
CIRCULATION
Two important factors to keep in mind during management are positioning and compensation:
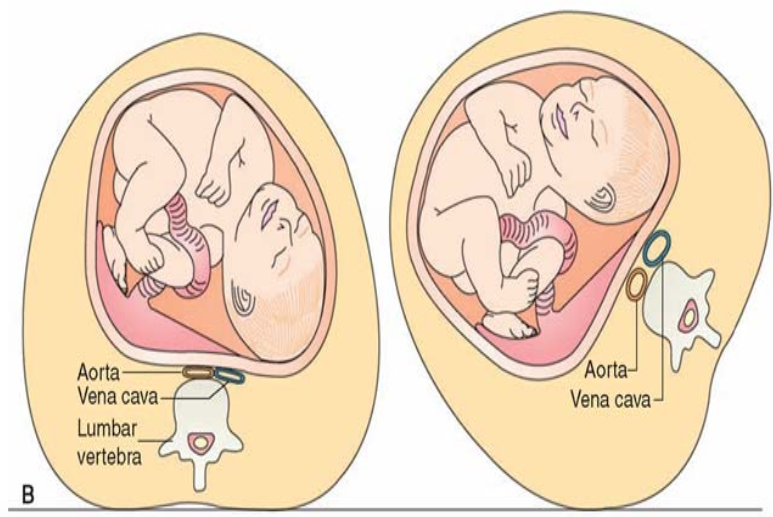
-The gravid uterus compresses the inferior vena cava, which can reduce venous return and reduce cardiac output by up to 30%2,7
-Consider tilting the patient to the left side on the backboard or manually displacing the uterus to improve maternal circulation
– Recognition of maternal cardiovascular collapse may be delayed due to maternal compensation, i.e. 25-30% of volume may be lost prior to signs of instability6
–Avoid vasopressors => decreased fetal circulation
-If central access is needed, avoid femoral lines => compression of femoral veins secondary to gravid uterus8
–Optimization of maternal resuscitation will optimize fetal viability and improve fetal outcome.4
 George Koenig DO, FACS; Thomas Jefferson University Hospital
George Koenig DO, FACS; Thomas Jefferson University Hospital
Imaging
-Consider performing bedside ultrasound for initial evaluation
–Do not delay or withhold any necessary diagnostic or therapeutic tests due to fear of harming the fetus => exposure to < 5 rads has minimal risk1,2,8
-Shield whenever possible to minimize radiation exposure
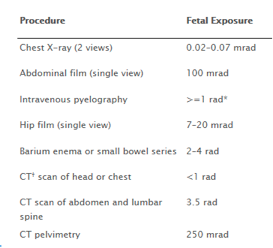
Figure 1: Fetal Exposure from Diagnostic Imaging (Adapted from http://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Obstetric-Practice/Guidelines-for-Diagnostic-Imaging-During-Pregnancy) Accessed on December 22, 2015
When to Administer Rhogam?
-Feto-maternal hemorrhage (FMH) is evaluated by the Kleihauer-Betke (KB) acid elution technique of maternal blood, which has a sensitivity of 5 mL of FMH
-Unfortunately, as little as 1 mL of FMH can sensitize 70% of Rh-negative woman
-Severity of trauma is not a good indicator of the degree of FMH
-Recommendation: all Rh-negative women with a history of abdominal trauma should receive one 300-ug prophylactic dose of Rhogam within 72 hours of the traumatic event7
-Generally, the fetal blood volume is less than 30 mL until 16 weeks gestation
-Don’t under-dose: Give 300-ug of Rhogam per each 30 mL of FMH, as determined by KB testing
Post-Resuscitative Monitoring
After ventilatory and hemodynamic stabilization is achieved, simultaneous evaluation of injuries to the mother can occur while initiating monitoring of the fetus.
-Consult your OB/GYN service for fetal heart rate monitoring and tocometry.
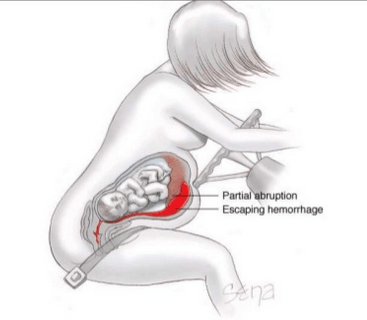
-Monitoring fetal heart tones can be a useful early indicator of maternal cardiovascular collapse and to assess for placental abruption, premature rupture of membranes, and FMH2
-Avoid tocolytics => uterine contractions are useful in monitoring fetal viability and maternal hemodynamic status7
Resuscitative Efforts
In the event that stabilization fails and the mother develops cardiac arrest, ACLS guidelines can be followed.
-Tilting may be difficult during CPR => have assistant manually displace uterus
-Avoid amiodarone => risk of iodine toxicity to the fetus
-Guidelines recommend the completion of a peri-morteum C-section within 5 minutes of a cardiac arrest, which may increase maternal cardiac output by up to 80%5.
–Indications for peri-mortem C-section after 4 minutes of CPR without ROSC1,5:
–Gestational age >24 weeks, i.e. fundal height four finger-breadths above umbilicus
–Fetal viability => bedside sonography with positive fetal heart tones
–Continue CPR during peri-mortem C-section and have a separate team at the bedside to care for the fetus
Summary
- Any resuscitative efforts geared toward optimizing the medical management of the pregnant mother will optimize the fetal well-being.
- Provide high oxygen flow to compensate for the pregnancy-based predisposition toward hypoxia.
- Aggressive IV fluids administration, since blood pressure and pulse are not a reliable indicator of impending cardiovascular collapse during pregnancy.
- Avoid having the gravid uterus compressing the inferior vena cava with left-sided upward tilt, wedge displacement, or manual displacement.
- Avoid femoral lines that could be impeded by a gravid uterus.
- Administer prophylactic dose of Rhogam to all Rh-negative mothers with abdominal trauma.
- Peri-mortem C-section should be considered within 5 minutes of witnessed cardiac arrest.
References / Further Reading
- Barraco, Robert D. MD, MPH; Chiu, William C. MD; Clancy, Thomas V. MD; Como, John J. MD; Ebert, James B. MD; Hess, L. Wayne MD; Hoff, William S. MD; Holevar, Michele R. MD; Quirk, J. Gerald MD, PhD; Simon, Bruce J. MD; Weiss, Patrice M. MD, Pregnant Patient, Diagnosis and Management of Injury, J Trauma. 69 (1): 211-4, July 2010. https://www.east.org/education/practice-management-guidelines/pregnant-patient%2c-diagnosis-and-management-of-injury
- Bouchard, Scott. ACEP Now , Trauma in the Obstetric Patient: A Bedside Tool, July 1, 2010
- Chames, Mark C. MD and Mark D. Pearlman, Trauma During Pregnancy: Outcomes and Clinical Management, Clinical Obstetrics and Gynecology, Volume 51, Number 2, 398–408,v http://www.emergpa.net/wp/wp- content/uploads/2012/02/Trauma-during-Pregnancy-Outcomes-and-Clinical-Management.pdf
- Chang, Andrew K MD., Pregnancy Trauma. http://emedicine.medscape.com/article/796979-clinical
- Datner, Elizabeth M. Promes, Susan B. Resuscitation issues in pregnancy. Tintinalli’s Emergency Medicine: A comprehensive study guide. 2011. Pages 91-96
- Delorio, Nicole M. Trauma in Pregnancy. Tintinalli’s Emergency Medicine: A comprehensive study guide. 2011. Pages 1687-1691.
- Desjardins, Georges. MD FRCPC, Management of the Injured Pregnant Patient. http://www.trauma.org/archive/resus/pregnancytrauma.html
- http://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Obstetric-Practice/Guidelines-for-Diagnostic-Imaging-During-Pregnancy (Accessed on December 22, 2015)





1 thought on “Trauma Management of the 3rd-Trimester Pregnant Patient: Pearls & Pitfalls”
[…] EMDocs: Trauma Management of the 3rd-Trimester Pregnant Patient: Pearls & Pitfalls […]