Originally published on Ultrasound G.E.L. on 3/26/18 – Visit HERE to listen to accompanying PODCAST! Reposted with permission.
Follow Dr. Michael Prats, MD (@PratsEM) from Ultrasound G.E.L. team!

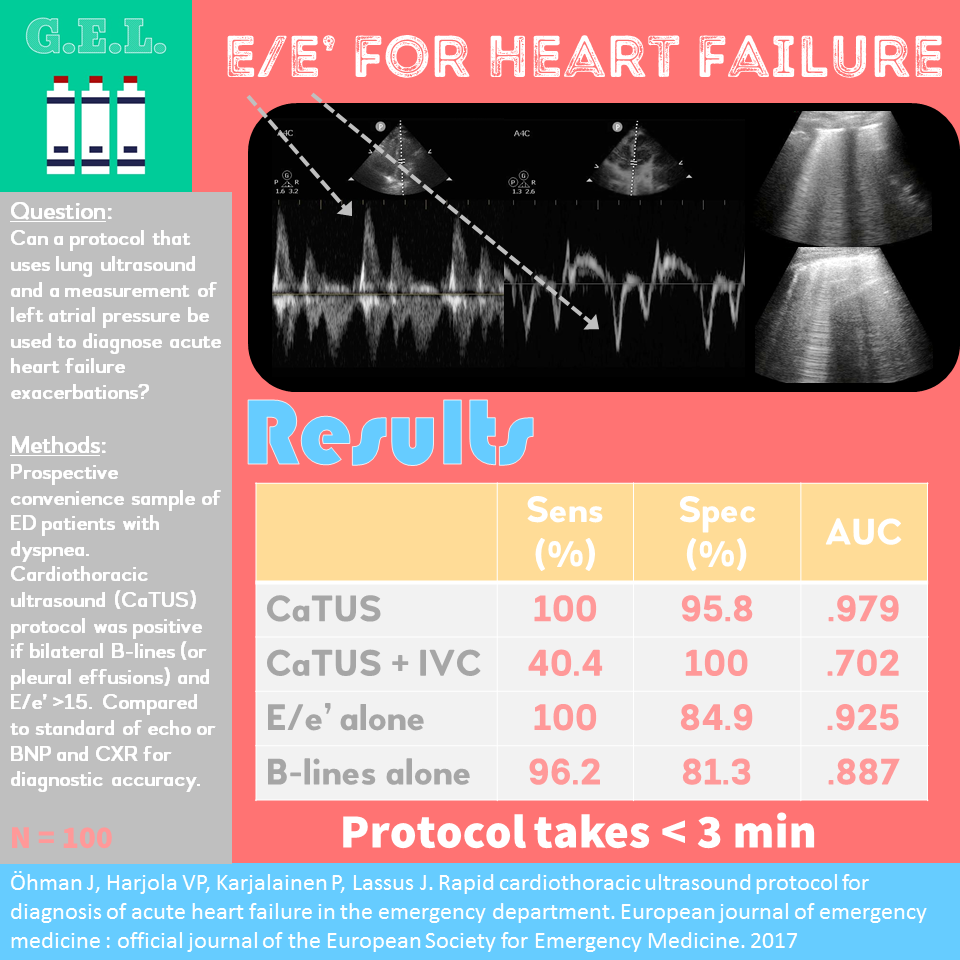
Rapid cardiothoracic ultrasound protocol for diagnosis of acute heart failure in the emergency department
European Journal of Emergency Medicine Oct 2017 – Pubmed Link
Take Home Points
1. Measuring the left atrial pressure with E/e’ ratio may improve accuracy of ultrasound diagnosis of acute heart failure.
2. The combined lung and echo protocol in this small study had 100% sensitivity and 98.5% specificity for diagnosing acute heart failure, but limitations include a poor gold standard and lack of blinding.
Background
We’ve covered ultrasound for dyspnea and also for acute heart failure before. We know that ultrasound is good for this. It can help make the diagnosis in less time and seems to be more accurate than many traditional diagnostics (chest xray, serum BNP). What this article brings to the table is the addition of diastolic measurements in the assessment of suspected acute heart failure exacerbation. The idea is that not all heart failure has systolic dysfunction, which is the finding usually included in focused heart failure protocols. What we care about in the acute setting is any type of heart failure (systolic or diastolic) that leads to the development of pulmonary edema. Pulmonary edema in heart failure usually develops when the left atrial pressure gets too high. The ratio of the E wave to the e’ wave can estimate the left atrial pressure and is fairly accurate even in irregular rhythms. These authors surmised that by adding the E/e’ estimation of the left atrial pressure to the evaluation of the acutely dyspneic patient, it might improve the accuracy of the exam. I guess we’ll find out.
Question
How accurately does a cardiac and lung ultrasound protocol including measurement of left atrial pressure diagnose an acute heart failure exacerbation?
Population
Single, tertiary care center in Turku, Finland
Inclusion:
- Adults with undifferentiated dyspnea in the ED
Exclusion:
- Unsatisfactory visibility on ultrasound
- Known pulmonary fibrosis
- Age <18
- Mitral stenosis on echo
- Prosthetic mitral valve
Design
Prospective convenience sample
All patient enrolled received intervention
The gold standard for the diagnosis of Acute Heart Failure (AHF) was defined as meeting one of two criteria:
- Structural heart disease on echo OR
- BNP > 400 ng/l OR BNP > 100 ng/l with pulmonary congestion on CXR
Intervention
CaTUS (cardiothoracic ultrasound) protocol was initiated immediately after arrival to the ED (before further investigations). See “Scan” below for details.
All patients had serum BNP
Most also had chest xray (96%) – unclear who determined if CXR was performed. Presumably treating physician.
Who did the ultrasounds?
Single experienced sonographer with >1000 examinations of echo and lung ultrasound (possibly a cardiologist?).
The Scan
Phased array probe

The CaTUS protocol:
- Patient supine with upper body elevated slightly
- Leftward rotation allowed only if necessary (avoiding postural alteration of cardiac filling pressures)
- Cardiac Component: Apical four chamber view obtained. E wave recorded a tip of mitral valves, averaged 3 consecutive cycles. If irregular, averaged 5 cycles. e’ measured with tissue doppler at medial mitral annulus.
- Lung Ultrasound component (LUS): Two pulmonary fields per side (apical and mammillary regions) in mid clavicular line → looking for B-lines
- Additional pulmonary view in axillary line looking for pleural effusions
- Also evaluated IVC, calculated IVC index.
IVC index was graded 1-3.
- Grade 1 was <21 mm + >50% respiratory variation
- Grade 2 was >20 mm OR respiratory variation <50%
- Grade 3 was >20 mm AND respiratory variation <50%
CaTUS exam was positive if +LUS and E/e’ >15
Lung ultrasound was positive if at least 3 B-lines in one intercostal space bilaterally OR bilateral pleural fluid (>5 mm of dependent fluid)
Thorough Introduction to Diastology
Slightly shorter but still long video on Diastolic function
Learn about B-lines on 5 Minute Sono!
Results
The Patients
N = 100 patients
Patients:
- 52 had acute heart failure
- Acute heart failure patients were older (~10 years on average), had more comorbidities (renal failure – could affect the BNP used in gold standard), less pulmonary disease (COPD, parenchymal disease).
- Acute heart failures patients also had higher respiratory rate (25 vs 21), less wheezing, less sinus rhythm, more QRS widening.
Primary Outcomes
CaTUS:
Sensitivity 100% (91.4-100)
Specificity 95.8% (84.6-99.3)
Best Area Under the Curve (AUC): 0.979
Bilateral B lines alone:
Sensitivity 96.2% (86.8-99.5)
Specificity 81.3% (67.4-91.1)
AUC 0.887
E/e’ > 15 alone:
Sensitivity 100% (91.4-100)
Specificity 84.9% (71.9-92.8)
AUC 0.925
CaTUS + IVC ≥ grade 2:
Sensitivity 86.5% (73.6-94.0)
Specificity 97.1% (88.8-99.5)sensitive, 97.1% specific
AUC 0.918
CaTUS + IVC ≥ grade 3:
Sensitivity 40.4% (27.3-54.9)
Specificity 100% (93.3-100)
AUC 0.702
Other Findings
In comparing Acute heart failure (AHF) and Non-Acute Heart failure (Non-AHF) patients, there were several differences between populations. A BNP > 400, bilateral B-lines, bilateral pleural fluid, E/e’, IVC index, and congestion on CXR all were significantly different between the groups. BUT that is because echo, CXR, and BNP were used as gold standard! However note:
- 22.9% of non-AHF had BNP >400 (~50% elevated above 100)
- 18.8% of non-AHF had bilateral Blines (whereas only 6.3% had bilateral effusions)
- 8.3% of non-AHF had congestion on CXR
Interestingly – there was no statistically significant different in LV EF in AHF vs non-AHF (42.4 vs 51.8%). This seems to be in contrast to the accuracy of other protocols that utilize systolic dysfunction to diagnosis acute heart failure. This paper we reviewed found systolic dysfunction and bilateral anterior B-lines to be 100% specific.
All exams lasted < 3 min
100% interobserver agreement for +LUS. For E/e’ there was a mean inter-observer coefficient of variation of 9.99%.
30 patients were referred for a review by cardiologist (blinded to clinical information) – 95.8% sens, 97.8% spec
E/e’ and LUS correlated well (kappa 0.796)
AUC for E/e’ identifying B-lines on lung ultrasound was 0.95
CaTUS found focal B-lines in 4/5 patients diagnosed with pneumonia. Also found right heart strain in 4/5 patients with PE. Also caught one dissection causing tamponade, and one chordae tendinae rupture causing cardiogenic shock. All in a days work.
A group of hypertensive AHF patients had IVC index of 0 which brought down the accuracy of adding the IVC.
Limitations
Gold standard is not ideal – just having disease on echo does not imply causality for symptoms. Secondly, BNP is known to be a pretty bad test for acute heart failure (see First 10 EM post and EMNerd post). CXR is probably less good than ultrasound for picking up pulmonary edema so that is also a poor standard.
Skilled operator. Lots of scans. Not everyone would be comfortable calculating E/e’, although other emergency protocols have used this and shown it to be feasible.
Single center outside the US. Small study.
Excluded patients without good window and those with interstitial lung disease.
Sonologists in this study were not blinded to clinical presentation or vital signs → may have introduced some bias.
Discussion
There are two main issues here. The first, is this even feasible to implement in the emergency department? I think the answer to this is – sometimes. In the acute crashing patient – probably not. You need to have a decent apical four chamber window to get these measurements. It does take some additional training, because these doppler measurements are angle dependent. It will clearly be intimidating to many people, but it is not as complex as it sounds. This article does not do much to prove general feasibility since it was a single skilled operator in Finland (who may or may not be a cardiologist). The other aforementioned study seem to indicate that this is feasible to accomplish in the emergency department within a reasonable amount of time. I think it will take some training and convincing, but I don’t think that this alone would be prohibitive.
The second problem is that the flaws in this study call into question the impressive accuracies these authors found. As mentioned above, the main two problems are the gold standard used and the lack of blinding. Although this study is thought provoking, I think that these limitations might prevent me from trusting the accuracy of measuring the E/e’ in the diagnosis of acute heart failure. What’s your take?
Take Home Points
1. Measuring the left atrial pressure with E/e’ ratio may improve accuracy of ultrasound diagnosis of acute heart failure.
2. The combined lung and echo protocol in this small study had 100% sensitivity and 98.5% specificity for diagnosing acute heart failure, but limitations include a poor gold standard and lack of blinding.
Our score

Cite this post as
Michael Prats, MD. E/e’ for Acute Heart Failure. Ultrasound G.E.L. Podcast Blog. Published on March 26, 2018. Accessed on July 30, 2021. Available at https://www.ultrasoundgel.org/43.





