Originally published on Ultrasound G.E.L. on 5/10/21 – Visit HERE to listen to accompanying PODCAST! Reposted with permission.
Follow Dr. Michael Prats, MD (@PratsEM) from Ultrasound G.E.L. team!

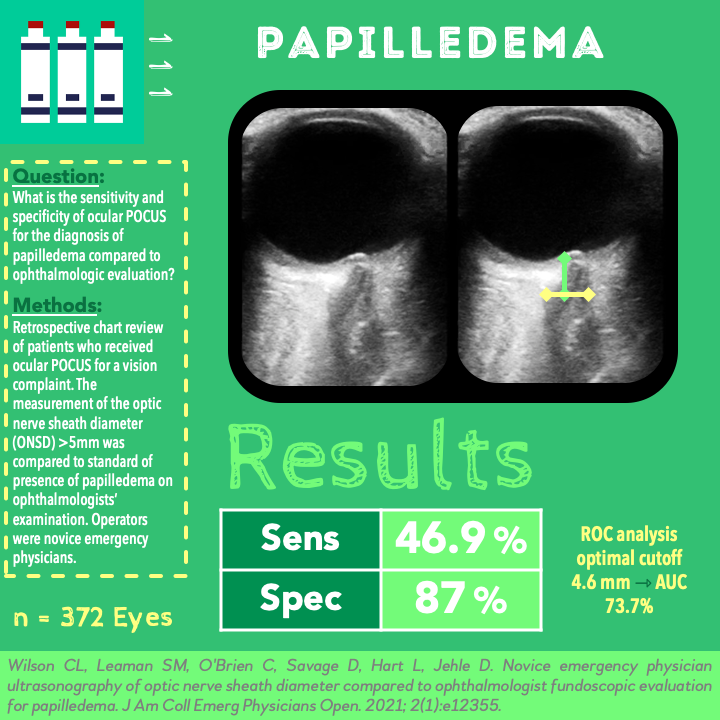
Novice emergency physician ultrasonography of optic nerve sheath diameter compared to ophthalmologist fundoscopic evaluation for papilledema
Unrelated Cases Mentioned in Podcast
Use of point-of-care ultrasound to diagnose an alternate cause of flank pain in a patient with presumed renal colic
Take Home Points
1. The results of this article would suggest that ONSD is not sufficiently accurate enough to rule in or out elevated intracranial pressure however, given the limitations of the study it should not change current practice.
2. Prospective research is needed to evaluate whether or not patients with primary visual complaints may be distinct from prior populations in which ONSD was studied.
Background
Using ocular ultrasound looking at the optic nerve sheath diameter (ONSD) can be helpful in evaluating for increased intracranial pressure. However, there have not been many studies evaluating whether or not ultrasound is good at visualizing papilledema (swelling of the optic disc due to elevated intracranial pressure). This would be really helpful because let’s face it – many of us do not do a dilated fundoscopic exam in the acute setting and therefore it can be a challenge to directly see when this pathology is present. This comes up all the time, especially in patients with suspected Idiopathic Intracranial Hypertension (IIH). If ultrasound could accurately discern the presence of papilledema, it might provide a fast and noninvasive way to identify these patients and expedite management.
Question
What is the sensitivity and specificity of emergency physician-performed ocular ultrasound for the diagnosis of papilledema compared to the reference standard of ophthalmology evaluation?
Population
Emergency department patients, data from 2014-2017
Inclusion:
- ≥17 years old
- Primary vision complaint + ophthalmology consultation + bedside ocular ultrasound
Exclusion:
- Did not receive BOTH formal ophthalmology evaluation and bedside ultrasound by an emergency physician
Design
Retrospective chart review
Identified patients who received a point-of-care ocular ultrasound for a vision complaint
Compared the measurement of the ONSD to the grading of the papilledema on an ophthalmologists examination
Calculated the sensitivity, specificity, PPV, NPV. Also looked at the ROC and sought to determine an optimal ONSD cutoff value for optimal accuracy.
Who did the ultrasounds?
Novice resident emergency physicians (most on their intern emergency ultrasound elective)
55 different residents ranging from PG1-PGY4
Most operators had between 2 and 20 ocular ultrasounds during this study period.
The Scan
Linear Transducer

Optic nerve sheath diameter (ONSD) measured 3 mm posterior to the papilla
Measured diameter in 2 planes, used the average
Standard cut off of >5 mm considered abnormal (papilledema).
Learn how to do Optic Nerve Sheath Diameter from 5 Minute Sono!

Check out Ocular Pathology on the POCUS Atlas!

Results
N = 372 eyes
- 212 encounters, 206 patients (some with repeat visits)
- Based on the total, not every eye was looked at by both ultrasound and ophthalmologist for each of these patients
- 51% female
- 13.2% (28) had papilledema
- 78.6% of patient with papilledema were female
- Median age 37 (with papilledema) and 48 (without papilledema)
Primary Outcome – Using 5mm Cutoff
Sensitivity 46.9% (CI 32.5-61.7%)Specificity 87% (CI 82.8-90.5%)
Likelihood Ratios (not reported but I calculated)
+LR 3.61-LR 0.61
Secondary Outcomes
ROC analysis identified optimal cutoff of 4.6 mm yielding sensitivity of 67.3% and specificity 67.5%, AUC 73.7%.
Strengths
Practical reference standard
Large sample size compared to prior studies
Novice operators assesses for feasibility in settings with less POCUS expertise
Limitations
Retrospective, no uniform criteria for ophthalmology consultation or POCUS indication which would bias the population. Lack of blinding could have influenced the interpretations of both the POCUS and the fundoscopic exam (although it is pretty normal to integrate that into both). What if the patients just had a headache? Might be a skewed population of idiopathic intracranial hypertension (IIH).
Limited operator experience with no evaluation of image quality makes it unclear whether or not it was the operators experience responsible for the low specificity seen.
No comparison to actual measurement of intracranial pressure. Reference standard of the ophthalmology exam is reasonable, but could have inaccuracies. Furthermore, true papilledema may not be present in all cases of elevated intracranial pressure. Speaking of true papilledema, it should technically be bilateral in almost every case – does analyzing individual eyes actually double the n of this study without studying more people? I suppose each eye is an opportunity to test the strength of the test so it is probably fine the way they did it.
Discussion
It is surprising that these results showed low sensitivity and higher specificity. This is in contrast to the many metaanalyses (1, 2, 3, 4, 5) that have been performed comparing ONSD on ultrasound to CT or direct intracranial pressure measurements. Those have shown sensitivities in 90-99%, specificities 73-86%. Could this be because of the select patient population with only vision complaints or because of the relatively novice operators? Hard to say. I hesitate to agree with the authors that we should lower the cut off based on their study. There are so many reasons why an ONSD could be elevated, and I think this would lead to an unacceptable amount of false positives (especially given the lack of specificity seen in all prior studies).
What about optic nerve elevation (ONE)? A few studies have demonstrated that this could be a more accurate way to diagnose papilledema. Definitely an area to explore with more research. We talk about this more on our two part special edition podcast with Denver Health. Here are more articles on that idea 1, 2.
Summary
This is a retrospective study of 372 eyes of emergency department patients with visual complaints. They found that compared to an ophthalmologists exam, the POCUS ONSD was 87% specific and <50% sensitive.
Take Home Points
1. The results of this article would suggest that ONSD is not sufficiently accurate enough to rule in or out elevated intracranial pressure however, given the limitations of the study it should not change current practice.
2. Prospective research is needed to evaluate whether or not patients with primary visual complaints may be distinct from prior populations in which ONSD was studied.
More Great FOAMed on This Topic
Our score

Expert Reviewer for this Post

Jeremy S. Boyd, MD, FACEP @geek_md
Living and working in Nashville, TN as Ultrasound Fellowship Director at Vanderbilt University Medical Center and another hospital that starts with a V.
Reviewer’s Comments
The reviewer accurately points out the limitations of this study when it comes to the utility and test characteristics of Optic Nerve Sheath Diameter (ONSD) for Papilledema. They rightly point out the limitations of the methodology, especially the problem of a reference or criterion standard that is uniformly utilized. It’s important to emphasize the notable differences in the test characteristics of ONSD in this study as compared to others, however, to a certain extent this is likely the result of comparing sonographic apples to oranges—ONSD and papilledema are both used as indicators of elevated intracranial pressure, and neither is uniformly present in everyone with elevated intracranial pressure (ICP). As such it’s not surprising that the test performed poorly in this context when trying to identify another secondary physical exam finding associated with elevated ICP. Ocular ultrasound is incredibly useful, but ONSD has had some limitations due to interoperator differences in technique as well as varying cutoff points for the test. I agree with the author that lowering the threshold measurement would likely create far too many false positives. I’m glad they mention Optic Nerve Elevation—anecdotally this is something I’ve found to be more accurate for diagnosing papilledema and elevated ICP, and is an area of POCUS that deserves to be explored further for its test characteristics across large groups of patients and populations. In short, I think the probe scale is spot on for this one. Cool idea, but there are some flaws here that limit this study’s generalizability.
Cite this post as
Michael Prats. POCUS versus Ophthalmologic Exam for Papilledema. Ultrasound G.E.L. Podcast Blog. Published on May 10, 2021. Accessed on August 20, 2021. Available at https://www.ultrasoundgel.org/111.





