Author: Adrianna Long, MD (Emergency Medicine Staff at Winn Army Community Hospital, Fort Belvoir, GA) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit)
It is important that providers make the correct choice for imaging when dealing with emergent conditions. MRI is a costly choice, but sometimes the most appropriate to evaluate for specific pathology. It is imperative to weigh the risk and benefits of MRI as compared to other imaging modalities. Also, in many facilities, MRI is only available during business hours, which makes obtaining emergent MRIs very difficult. So, when is ordering an MRI in the Emergency Department indicated?
MRI of the Brain
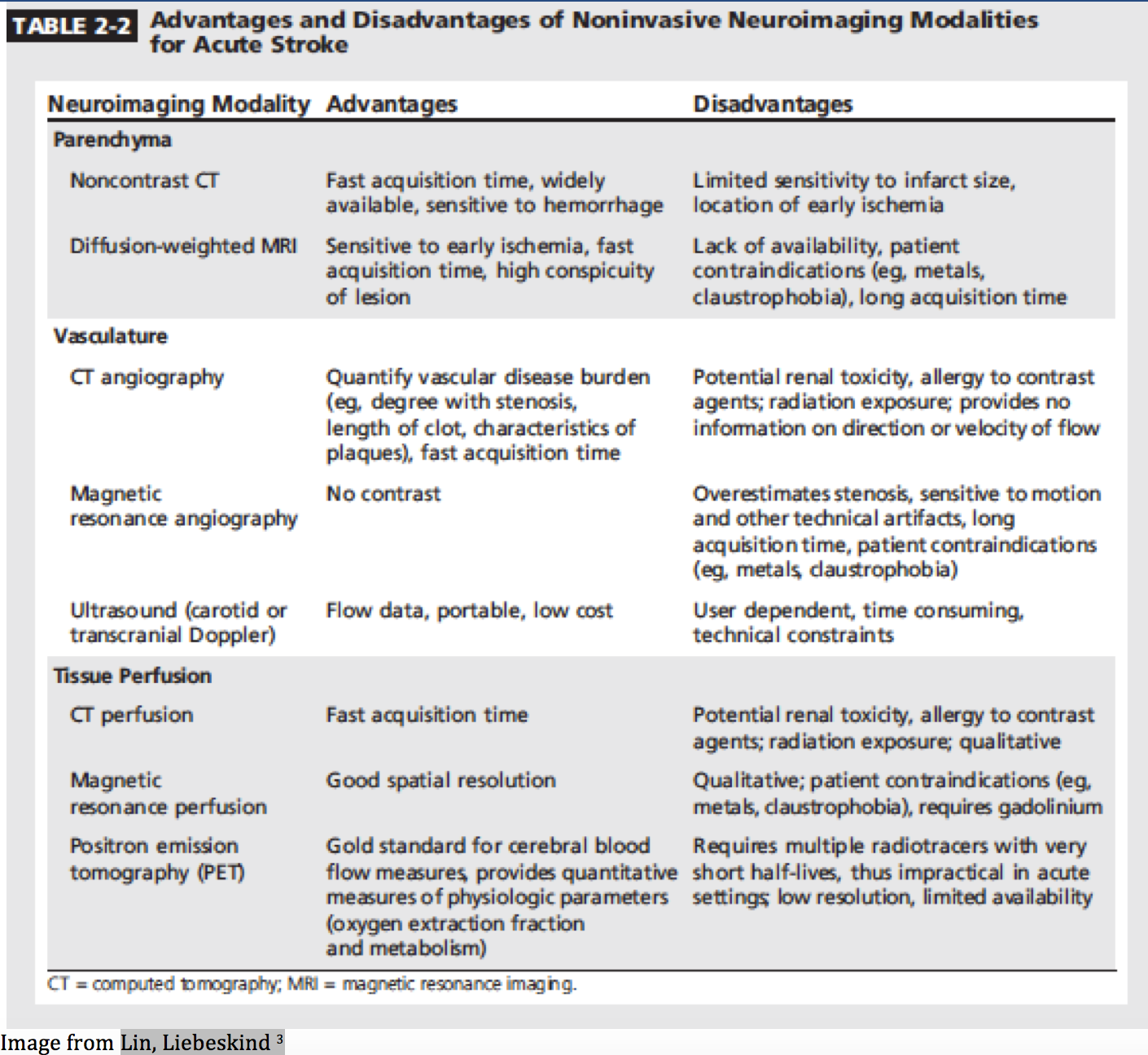
MRI has a significantly greater detection rate for acute ischemic infarction than CT, particularly in an early setting. CT has been reported to have a sensitivity ranging from 73-88% for acute stroke within the first 12 hours. In comparison, MRI has a sensitivity of 93-100% and may be able to detect acute ischemic injury within a few minutes of onset.1,2 However, not all patients that have acute strokes are candidates for interventions including tPA or endovascular therapy, so it is important to choose the appropriate imaging modality as an MRI may not be indicated emergently.
There is no standard imaging protocol for the evaluation of acute stroke or TIA beyond head CT noncontrast. The goal of neuroimaging is to provide rapid information and increase providers’ decision-making with regards to reperfusion therapy without causing harm from delays.3
A study recently published reviewed the imaging of 8,247 patients who were evaluated with TIA or minor stroke in 2011, revealing that approximately 50% of patients underwent MRI imaging within 2 days of presentation. The use of MRI to evaluate TIA or stroke is limited in many facilities with lack of availability, and MRIs are often ordered by inpatient services rather than emergently.4
The American College of Neuroradiology, the American College of Radiology, and Society of NeuroInterventional Surgery have made a joint statement with regards to the imaging of acute stroke and TIA. When determining whether endovascular therapy should be considered, they have found that noncontrast CT with digital subtraction angiography, noncontrast CT with CTA, and MRI with MRA are equivalent options for clinicians.5 Of those imaging modalities, noncontrast CT with CTA is the preferred strategy currently when selecting intraarterial thrombectomy candidates, as CT is widely available and faster.6
While a cavernous venous thrombosis (CVT) is a rare diagnosis, the use of MRV offers an alternative diagnostic modality. The MRV is more sensitive at diagnosis of a CVT than an unenhanced CT.7 Therefore, when considering CVT as a diagnosis, MRV may be considered for imaging, but CT venography is rapid, readily available, and an accurate technique to detect CVT.7
MRI of the Spine
The early diagnosis of an epidural abscess is essential to minimize patient morbidity and mortality. A study of 63 patients with spinal epidural abscess indicated that a delay in diagnosis greater than 24 hours occurred in 75% of cases, and persistent motor weakness resulted in 45% with diagnostic delays.8 The ACR ranks MRI of the spine with and without contrast as the most appropriate study to evaluate for infectious processes of the spine. When there is clinical suspicion for an epidural abscess, the emergency physician should insist on early MRI to prevent poor neurologic outcomes.9
The sudden onset of neurologic deficit due to neoplasm is another emergency that requires immediate imaging, neurosurgical consult, and treatment with high dose steroids.10
Epidural hematoma is a rare cause of back pain that may be associated with myelopathy and usually the result of recent spinal procedures or trauma. The symptoms may present similarly to an acute disc herniation. Patients who may be of particular risk are those on anticoagulant therapy.10
Cauda equina syndrome (CES) is suspected when there is severe lower back pain and radicular symptoms, especially at L5/S1, with saddle anesthesia and bowel/bladder/sexual dysfunction. The diagnosis of CES requires an emergent MRI followed by rapid surgical decompression.11
Basically, if serious underlying pathology is plausible or there is evidence of neurologic involvement in patients with back pain, MRI is the study of choice.9
MRI to evaluate for appendicitis
Pediatric patients:
Efforts are being made to decrease ionizing radiation exposure in pediatric patients, and MRI has been shown to be useful for the diagnosis of acute appendicitis.12 MRI protocols have been created with combined use of ultrasound to diagnose appendicitis in many hospitals for adult and pediatric patients. In one institution over 30 months, MRI has been shown to have a sensitivity of 96.8%, specificity of 97.4%, negative predictive value of 98.9%, and positive predictive value of 92.4%.13
A retrospective study at another institution with utilization of MRI for 49 pediatric patients with suspected appendicitis after having indeterminate ultrasound found a sensitivity of 94% and a specificity of 100% for diagnosis of acute appendicitis. There were a total of 16 patients diagnosed with appendicitis. The use of MRI aided clinicians in obtaining final diagnoses as well, including other diagnoses such as pyelonephritis, constipation, pelvic inflammatory disease, ruptured ovarian cyst, hemorrhagic cyst, and epiploic appendagitis.14
A study of 662 pediatric patients imaged with CT versus MRI found no significant difference in time to antibiotic administration, time to appendectomy, perforation rate, or hospital length of stay for patients imaged with either modality.15
Pregnant patients:
In 2011, the American College of Radiology (ACR) designated ultrasound as the initial imaging study choice to evaluate for acute appendicitis in pregnant patients.16 However, there have been multiple studies published indicating that ultrasound may not be the most appropriate imaging study to evaluate for appendicitis in pregnant patients since nonvisualization of the appendix has been reported to range as high as 68-97%.17-19 The efficiency of ultrasound may be limited due to bowel gas, body habitus, and anatomic displacement of the appendix, as well as patient tolerance in the setting of an acute abdomen.18
A meta-analysis of 6 articles analyzing the diagnostic strength of MRI in 359 pregnant women with suspected appendicitis found a specificity of 98% and 99% negative predictive value when a normal appendix is visualized.20
The ACR endorses the use of MRI when ultrasound cannot provide diagnostic information in pregnant patients. MRI has been shown to be useful for multiple diagnoses in pregnant patients with acute abdominal/pelvic pain.21 A retrospective study including 171 patients undergoing MRI with a pregnant appendicitis protocol had an appendix visualization rate of 69%. Furthermore, the overall diagnostic rate was 43.3% finding ovarian masses, ovarian torsion, uterine fibroid tumors, ectopic pregnancies, hernias, renal abscess, as well as appendicitis.22
MRI of the Hip
The use of MRI in the Emergency Department to evaluate for suspected hip fracture can be useful when the clinician has a high suspicion and there is a negative Xray or CT. Despite the use of CT to evaluate for hip fractures, there are still 2-4% with missed hip fractures.23,24 While there is a general consensus that a delay to surgery >48 hours is associated with a higher mortality, and a retrospective study of 6,638 patients with hip fractures indicated that surgery before 12 hours improved survival.25 The results of this study suggest that rapid diagnosis of a hip fracture is essential so patients can receive the appropriate treatment as soon as possible to avoid complications.
There is 100% sensitivity and 99% specificity in detecting hip fractures with abbreviated MRI. This hip protocol MRI may also be used to detect avascular necrosis (AVN) with a sensitivity of 97% and 100% specificity.26
Hazards in MRI scanning
Patients should be adequately screened prior to obtaining MRI, and alternative imaging should be considered in patients with:
- Renal disease (especially a GFR lower than 30mL/min)
- Allergy to gadolinium
- History of injury involving projectiles
- History of surgery with retained metallic items, e.g. surgical clips, pacemaker, stents
- Claustrophobia27
Nephrogenic systemic fibrosis (NSF) is a potentially fatal condition that has been associated with the use of gadolinium.28 A study of 8997 patients who received gadolinium showed a total of 15 patients (0.17%) who subsequently developed NSF, with a GFR of less than 30mL/min in all of the affected patients.29
Of note, there is inherent risk in sending patients who may become unstable during transport and time to obtain the MRI. Most MRIs require time away from the ED, utilizing emergency staff and equipment outside of the ED, for a prolonged period, or there may be a need to transport to a facility where MRIs are available.
Bottom line:
An MRI should only be ordered in the ED when the patient’s treatment and/or management will be affected.
The misuse of MRIs in the ED generates unnecessary costs to patients and increased time in the department. It is essential to weigh the risk(s) of ordering an MRI for your patient in the ED.
The indications for emergency MRI Brain include clinical concern for acute ischemic stroke, particularly wherein the management may differ with possible intervention versus less aggressive treatment plans.
If there is clinical concern for new spinal cord compression from disease or injury, an emergency MRI evaluation is necessary.
The indications for emergency spinal MRI include suspicion for:
- Spinal cord compression (herniated disc, burst fracture, tumors, etc)
- Spinal infection (i.e. abscess)
- Spinal trauma (epidural hemorrhage, etc)
- Demyelination with acute neurologic changes
Additionally, emergency MRIs may be considered if there is concern for:
- Appendicitis in the pregnant or pediatric patient
- Hip fracture not detected on plain film or CT
References/Further Reading:
- Krieger DA, Dehkharghani S. Magnetic Resonance Imaging in Ischemic Stroke and Cerebral Venous Thrombosis. Top Magn Reson Imaging. 2015;24(6):331-352.
- Lev MH. CT versus MR for acute stroke imaging: is the “obvious” choice necessarily the correct one? AJNR Am J Neuroradiol. 2003;24(10):1930-1931.
- Lin MP, Liebeskind DS. Imaging of Ischemic Stroke. Continuum (Minneap Minn). 2016;22(5, Neuroimaging):1399-1423.
- Chaturvedi S, Ofner S, Baye F, et al. Have clinicians adopted the use of brain MRI for patients with TIA and minor stroke? Neurology. 2017;88(3):237-244.
- Wintermark M, Sanelli PC, Albers GW, et al. Imaging recommendations for acute stroke and transient ischemic attack patients: a joint statement by the American Society of Neuroradiology, the American College of Radiology and the Society of NeuroInterventional Surgery. J Am Coll Radiol. 2013;10(11):828-832.
- Goyal M, Hill MD, Saver JL, Fisher M. Challenges and Opportunities of Endovascular Stroke Therapy. Ann Neurol. 2016;79(1):11-17.
- Leach JL, Fortuna RB, Jones BV, Gaskill-Shipley MF. Imaging of cerebral venous thrombosis: current techniques, spectrum of findings, and diagnostic pitfalls. Radiographics. 2006;26 Suppl 1:S19-41; discussion S42-13.
- Davis DP, Wold RM, Patel RJ, et al. The clinical presentation and impact of diagnostic delays on emergency department patients with spinal epidural abscess. J Emerg Med. 2004;26(3):285-291.
- Seidenwurm DJ, Wippold FJ, 2nd, Cornelius RS, et al. ACR Appropriateness Criteria((R)) myelopathy. J Am Coll Radiol. 2012;9(5):315-324.
- Arce D, Sass P, Abul-Khoudoud H. Recognizing spinal cord emergencies. Am Fam Physician. 2001;64(4):631-638.
- Mukherjee S, Thakur B, Crocker M. Cauda equina syndrome: a clinical review for the frontline clinician. Br J Hosp Med (Lond). 2013;74(8):460-464.
- Moore MM, Brian JM, Methratta ST, et al. MRI for clinically suspected pediatric appendicitis: case interpretation. Pediatr Radiol. 2014;44(5):605-612.
- Kulaylat AN, Moore MM, Engbrecht BW, et al. An implemented MRI program to eliminate radiation from the evaluation of pediatric appendicitis. J Pediatr Surg. 2015;50(8):1359-1363.
- Rosines LA, Chow DS, Lampl BS, et al. Value of gadolinium-enhanced MRI in detection of acute appendicitis in children and adolescents. AJR Am J Roentgenol. 2014;203(5):W543-548.
- Aspelund G, Fingeret A, Gross E, et al. Ultrasonography/MRI versus CT for diagnosing appendicitis. Pediatrics. 2014;133(4):586-593.
- Rosen MP, Ding A, Blake MA, et al. ACR Appropriateness Criteria(R) right lower quadrant pain–suspected appendicitis. J Am Coll Radiol. 2011;8(11):749-755.
- Israel GM, Malguria N, McCarthy S, Copel J, Weinreb J. MRI vs. ultrasound for suspected appendicitis during pregnancy. J Magn Reson Imaging. 2008;28(2):428-433.
- Lehnert BE, Gross JA, Linnau KF, Moshiri M. Utility of ultrasound for evaluating the appendix during the second and third trimester of pregnancy. Emerg Radiol. 2012;19(4):293-299.
- Vu L, Ambrose D, Vos P, Tiwari P, Rosengarten M, Wiseman S. Evaluation of MRI for the diagnosis of appendicitis during pregnancy when ultrasound is inconclusive. J Surg Res. 2009;156(1):145-149.
- Long SS, Long C, Lai H, Macura KJ. Imaging strategies for right lower quadrant pain in pregnancy. AJR Am J Roentgenol. 2011;196(1):4-12.
- Furey EA, Bailey AA, Pedrosa I. Magnetic resonance imaging of acute abdominal and pelvic pain in pregnancy. Top Magn Reson Imaging. 2014;23(4):225-242.
- Theilen LH, Mellnick VM, Longman RE, et al. Utility of magnetic resonance imaging for suspected appendicitis in pregnant women. Am J Obstet Gynecol. 2015;212(3):345 e341-346.
- Hakkarinen DK, Banh KV, Hendey GW. Magnetic resonance imaging identifies occult hip fractures missed by 64-slice computed tomography. J Emerg Med. 2012;43(2):303-307.
- Iwata T, Nozawa S, Dohjima T, et al. The value of T1-weighted coronal MRI scans in diagnosing occult fracture of the hip. J Bone Joint Surg Br. 2012;94(7):969-973.
- Bretherton CP, Parker MJ. Early surgery for patients with a fracture of the hip decreases 30-day mortality. Bone Joint J. 2015;97-B(1):104-108.
- Khurana B, Okanobo H, Ossiani M, Ledbetter S, Al Dulaimy K, Sodickson A. Abbreviated MRI for patients presenting to the emergency department with hip pain. AJR Am J Roentgenol. 2012;198(6):W581-588.
- Institute for Magnetic Resonance Safety E, and Research (IMRSER). Magnetic Resonance (MR) Procedure Screening Form For Patients and Magnetic Resonance (MR) Environment Screening Form for Individuals. 2017.
- Grobner T. Gadolinium–a specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrol Dial Transplant. 2006;21(4):1104-1108.
- Prince MR, Zhang H, Morris M, et al. Incidence of nephrogenic systemic fibrosis at two large medical centers. Radiology. 2008;248(3):807-816.




