
Author: Jason Brown, MD (EM Resident Physician, University of Maryland) // Edited by: Alex Koyfman, MD (EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital, @EMHighAK) and Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF)
DISTAL RADIUS FRACTURES
Colles’ Fracture
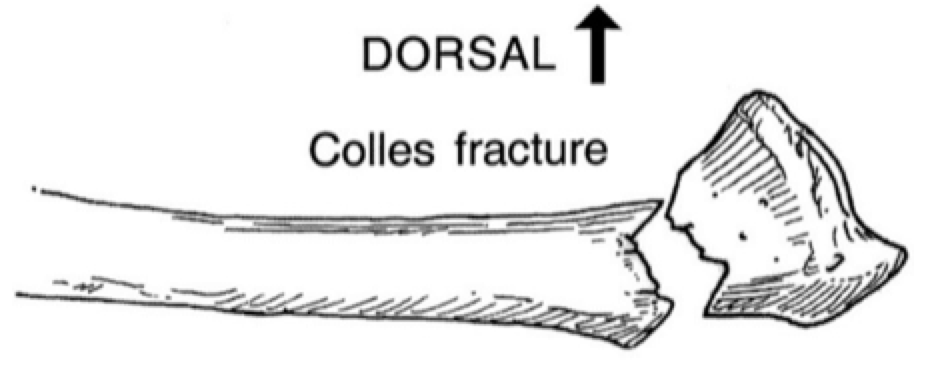 Originally described by Abraham Colles in 1814 after noticing a distinct fracture pattern in low energy injuries in elderly people, this fracture is typically dorsally displaced and angulated.1
Originally described by Abraham Colles in 1814 after noticing a distinct fracture pattern in low energy injuries in elderly people, this fracture is typically dorsally displaced and angulated.1
It occurs as a result of forced extension of the wrist, generally from a fall on an outstretched hand (FOOSH). There is significant tension on the volar aspect of the radius and compression on the dorsal aspect.
It is commonly associated with ulnar styloid process fractures, scapholunate dissociations, and injuries to the triangular fibrocartilage complex (TFCC).2
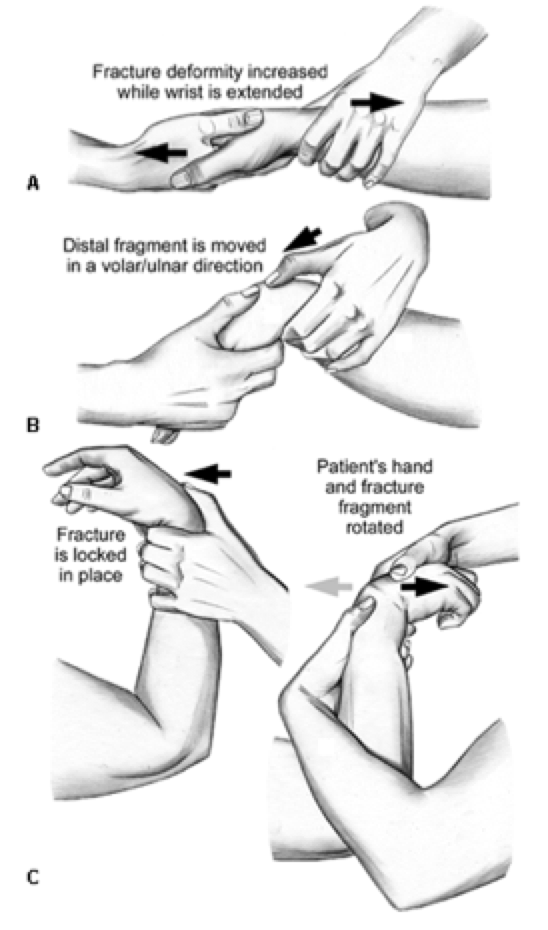
Reduction is achieved with longitudinal traction, over-exaggeration of the deformity (dorsiflexion), and replacement of the dorsally and proximally displaced fracture fragment into normal anatomic position. 2
A sugar-tong or double sugar-tong splint should be applied. The position of immobilization is under debate; however, the wrist should be kept in a position of function and slightly dorsiflexed and neutral.3
Non-displaced fractures can be seen in orthopedic follow-up within 10 days. Displaced fractures without satisfactory reduction should be seen urgently. 3
Smith’s Fracture
Named after Robert William Smith after he described the fracture in A Treatise on Fractures in the Vicinity of Joints.1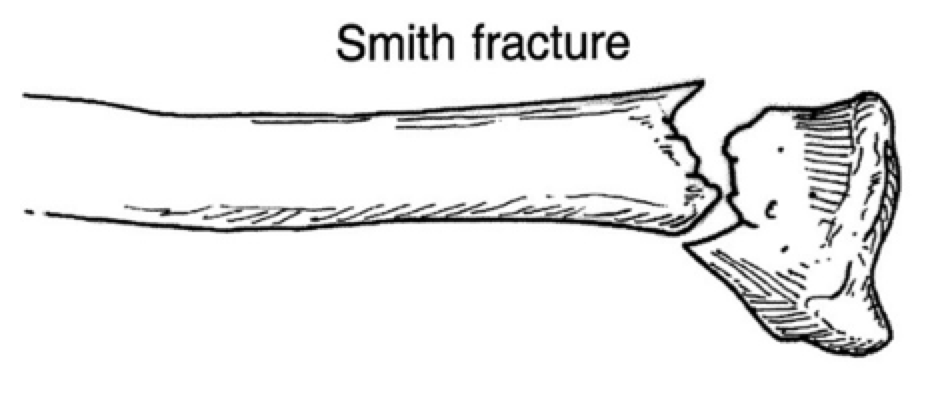
This fracture is often referred to as a reverse Colles’ fracture. The fracture is typically volarly displaced and angulated.
It occurs as the result of forced flexion and pronation of the wrist during a FOOSH or, less commonly, after a direct blow to the dorsal surface of the wrist.
Commonly associated with acute carpal tunnel syndrome (characterized by paresthesia in the median nerve distribution) as well as carpal injuries.4
Reduction is achieved with longitudinal traction with hyperflexion and return of the fracture fragment to anatomical position. Care should be taken when hyperflexing the wrist, as it can result in new and/or worsening median nerve damage.
A long arm/double sugar-tong cast should be applied with the wrist in neutral position and the forearm in supination.
Barton Fracture
Named after John Rhea Barton (1794-1871), who first described the injury pattern in 1838.1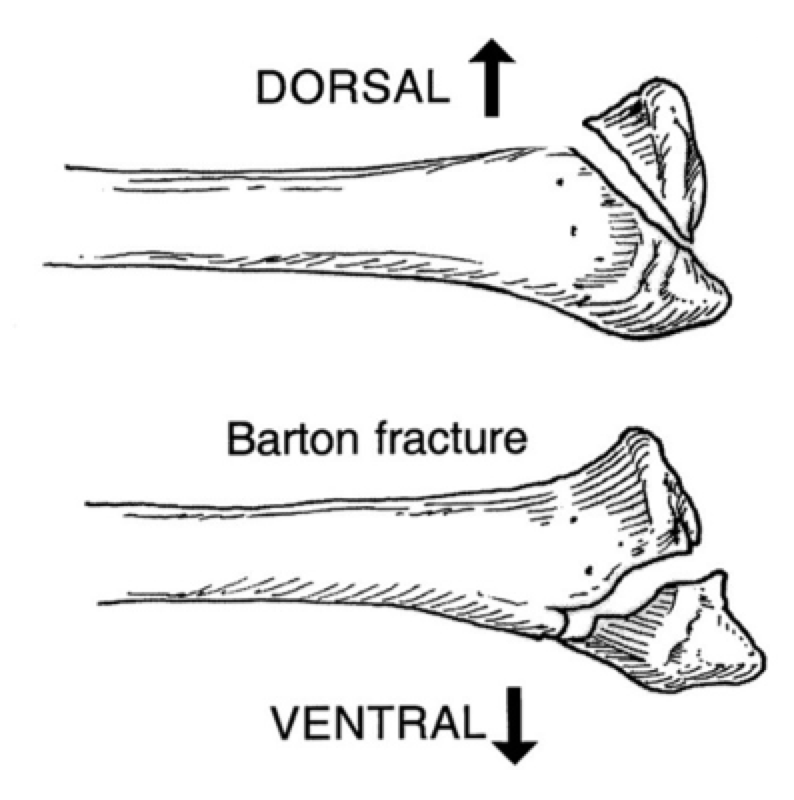
Barton fractures can either be displaced volarly or dorsally. The commonality in the two is that they are both fractures of the distal radius, through the joint space, and include dislocation of the overlying carpal bones with the fracture fragment. The volar type is more common than dorsal type.
Dorsal Barton fractures represent the most common fracture/dislocation of the wrist.2 It results from a FOOSH with the wrist in extension and pronation.
Volar Barton fractures result from a FOOSH onto a flexed wrist in pronation. It is sometimes referred to as a type III Smith’s fracture.
The majority of Barton fractures will require ORIF, especially those that involve >50% of the articular surface.
Chauffeur Fracture (aka Hutchinson’s fracture)
Named after Jonathan Hutchinson (1821-1913), a British surgeon. More colloquially known by chauffeur fracture, as it was commonly seen in patients of this profession.
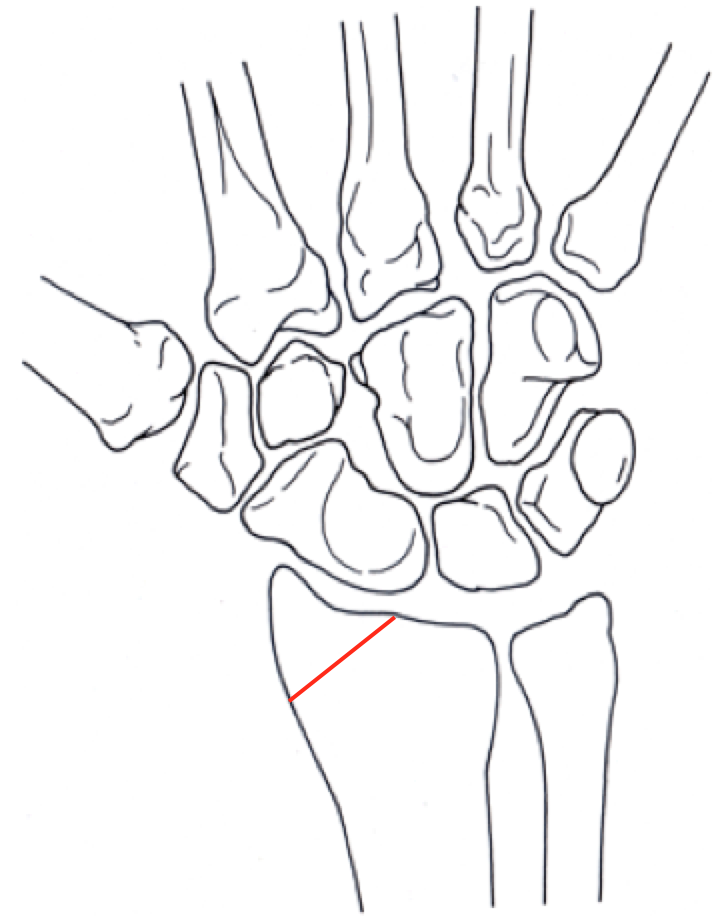 The fracture is typified by oblique fractures through the radial styloid process. These fractures are rarely displaced, but are high risk as they are always intraarticular.
The fracture is typified by oblique fractures through the radial styloid process. These fractures are rarely displaced, but are high risk as they are always intraarticular.
There are three mechanisms of injury. The first is from a direct blow on the dorsal surface of the wrist. The second is from a FOOSH with ulnar seviation and supination, leading to avulsion of the radial styloid secondary to the strength of the radioscapholunate ligament. The fracture is also seen in FOOSH injuries with extension and abduction of the wrist. This causes the scaphoid to impact the radial stylus, resulting in compression.
FOREARM FRACTURES
Galeazzi Fracture-Dislocation
First described by Riccardo Galeazzi (1866-1952), an orthopedist from Italy in 1934.1
The fracture is described as a distal 1/3rd radial shaft fracture with dislocation of the distal radioulnar joint with an intact ulna. A direct blow to the radius is a less common cause. The radius can displace either dorsally (type I) or volarly (type 2), with dorsal displacement being much more common.
These fracture-dislocations are more common in children with a peak incidence from 9-12. They generally occur as a FOOSH with a flexed elbow.
These fractures uniformly result in disruption of the distal radioulnar joint (DRUJ) and damage to the triangular fibrocartilage complex (TFCC). As such, they require emergent orthopedic evaluation for reduction and immobilization. The majority undergo ORIF for the radial fracture and K-wire fixation of the DRUJ.
Monteggia Fracture-Dislocation
Named for Giovanni Battista Monteggia (1762-1815), an Italian surgeon who first described the fracture in 1814. 1
Typified of a proximal ulnar shaft fracture with an associated proximal radial head dislocation. They generally occur as a result of a FOOSH. Radial head dislocation can be subtle and failure to identify this injury can have significant medicolegal implications.
These fractures generally require prompt orthopedic evaluation. All Monteggia-type fractures warrant ORIF with specialized reduction and immobilization techniques.
CARPAL FRACTURES
Scaphoid
Accounting for 70-80%, the scaphoid is the most commonly fractured carpal bone.5 The mechanism is a FOOSH in extension; less commonly, a direct compressive force.
Anatomically, the scaphoid is divided into the proximal pole (closest to the radius and lunate), waist (underlying the anatomical snuffbox), and distal pole (closest to the trapezium). The majority (80%) of fractures occur through the waist; the proximal and distal poles acount for the remaining 20% and 10%, respectively.6,7
Occult fracture of the scaphoid is common, with 20% of initial radiographs being read as negative.8 Physical examination is a poor tool to rule-in a scaphoid fracture but may be helpful in lowering the clinical suspicion of one.9 Tenderness of the anatomical snuffbox, thumb-compression induced pain, and pain illicited by resisted supination were all associated with high sensitivity but poor specificity. 9 Current estimates suggest that any patient with a suspected scaphoid fracture ought to be placed in a thumb spica splint. Pretest probability for occult scaphoid fracture in a patient with a concerning mechanism, negative radiographs, and positive physical exam findings is 25%; meaning we will splint three patients without a fracture for every patient with an occult scaphoid fracture.9
Triquetrum
Anatomically, the triquetrum is the most ulnar and dorsal of the first row of carpal bones. It lies just distal to the ulnar styloid process and is located just dorsal to the pisiform.
The triquetrum is the second most commonly fractured carpal bone, accounting for 4% to 20% of carpal fractures.10
Fractures generally occurs as a FOOSH with hyperextension and ulnar deviation. The majority of fractures are dorsal in nature and result from contact with either the hamate or the ulnar styloid process. 10 These are seen in a lateral view as a small fracture fragment lying dorsal to the carpal bones. A less common mechanism is by direct blow to the bone, resulting in a fracture through the body, which are difficult to detect on conventional radiography.
Dorsally displaced fractures should be placed in a short-arm splint with routine orthopedic follow-up. Body fractures require more urgent consultation.
Hamate
The hamate is the most ulnar of the second row of carpal bones. It is the third most commonly fractured carpal bone, accounting for 2% to 4%. 6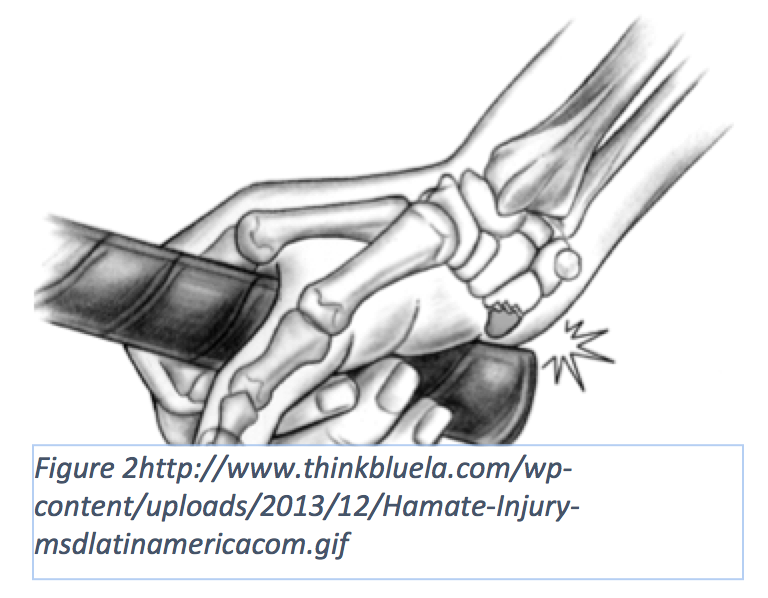
Fractures result most commonly from a direct blow to the hamate by a solid object, such as a bat or golf club, against the hook. Physical exam most often reveals tenderness to palpation of the volar aspect of the hypothenar eminence, pain with flexion of the 4th and 5th fingers, and weak/painful grip. 10,11
Hamate fractures are often difficult to diagnose on conventional carpal views. Addition of a carpal tunnel view may be helpful in diagnosis. If clinical suspicion is high then a CT should be ordered. 11
Treatment in the emergency room is the application of an ulnar gutter splint and orthopedic follow-up.
Perilunate Instability
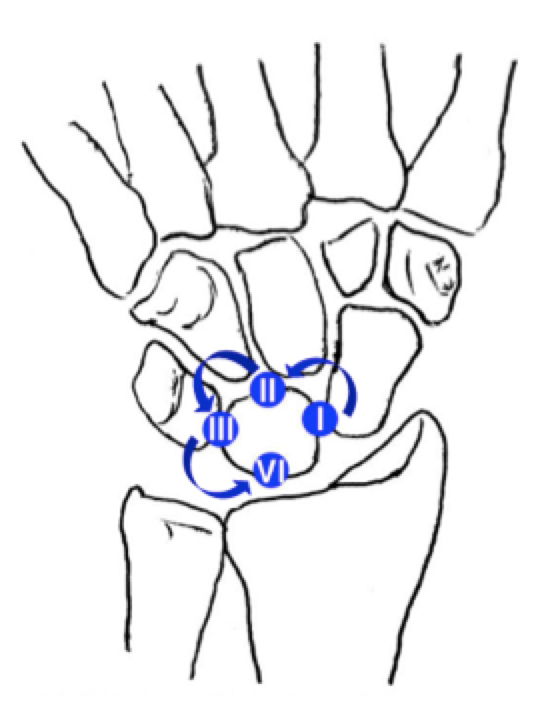
Perilunate instability occurs in distinct stages (termed the Mayfield classification) as the ligamentous support structure of the lunate is disrupted. These injuries are highly associated with distal radius fractures and generally occur as a result of a FOOSH injury. The stages correspond to scapholunate dissociation, perilunate dislocation, perilunate and triquetrum dislocation, and lunate dislocation. These injuries occur on a continuum from least severe to most severe. 12
 Complications related to these injuries are severe, including; avascular necrosis, acute or subacute carpal tunnel syndrome, median nerve injury, scapholunate advanced collapse (SLAC), and chronic arthritides. 12
Complications related to these injuries are severe, including; avascular necrosis, acute or subacute carpal tunnel syndrome, median nerve injury, scapholunate advanced collapse (SLAC), and chronic arthritides. 12
These ligamentous injuries can be seen with or without other injuries and their presentation can be subtle. A recent study 13 reports up to 25% of these injuries are missed on initial presentation.
Scapholunate Dissociation
Scapholunate dissociation occurs commonly from trauma involving a FOOSH onto an extended hand with ulnar deviation. This stresses and tears the scapholunate ligament, a U-shaped ligament between the two representative bones. The scaphoid undergoes rotary subluxation into a more volar alignment, creating a widening of the scapholunate joint space.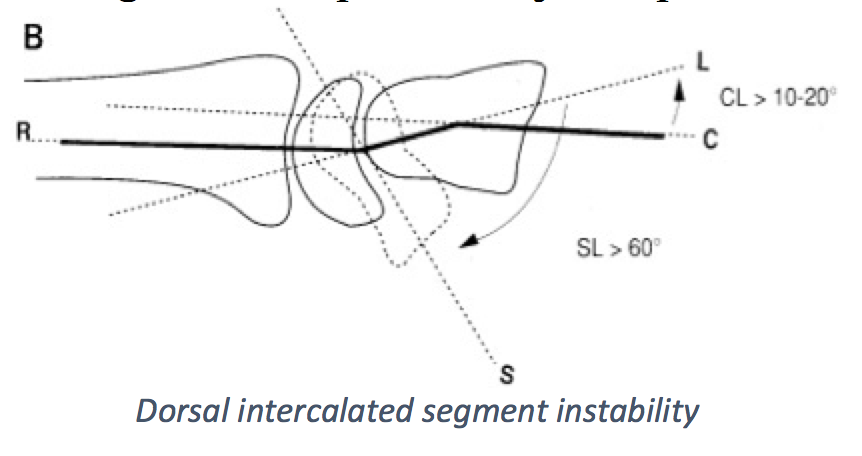
This widening is most easily noticeable on the PA view of the hand and is accentuated with ulnar deviation and/or a clenched fist view. Normal joint space should be <2mm. Widening of >4mm in the PA and >8mm in the ulnar deviation/clenched fist view are diagnostic. 14 This is often referred to as the “Terry Thomas” sign, after the British comedian of the same name who was known to have a wide gap in his central incisors.
In the lateral view, the lunate is dorsally rotated while the scaphoid enters a more volar orientation. This creates an increase in the normal scapholunate angle to >80° along with an increase in the capitolunate angle to >30°. 6 The injury pattern is often termed dorsal intercalated segment instability, due to the disruption of the dorsal intercarpal ligament and is always a pathologic finding.
Patients often present with other injuries and care should be taken to fully examine the carpal bone alignment on radiography.
Emergency room treatment includes prompt orthopedic referral for ORIF as closed reduction often fails.
Perilunate and Lunate Dislocation
Perilunate dislocation is the second stage of the Mayfield classification and results from capitolunate ligament failure. This allows the capitate to move dorsally and proximally.
Radiographs in the PA view show loss of the usual carpal joint arcs, resulting in a crowded appearance. The lateral view is confirmatory and is typified by dorsal dislocation and proximal shortening of the capitate, while the lunate remains in articulation with the radius.14 If there is enough force, the capitate will displace the lunate, disrupting the dorsal radiocarpal ligaments, and forcing the lunate into a volar position.
Due to the rotational and compressive forces involved between the first and second rows of carpal bones, there are often associated carpal fractures with perilunate dislocations; most common is a trans-scaphoid fracture. 13
These injuries should receive immediate orthopedic consultation for ORIF. Closed reduction can be achieved by palcing these patients in finger traps and then placing one thumb on the palmar surface of the lunate and one on the dorsal surface of the capitate. The goal is to volar-tilt the lunate and distally displace the capitate back into normal anatomic position. 15 Closed reduction often fails in these patients as the injuries cause intrinsic instability to the wrist; as such, all cases should be referred for immediate internal fixation.
Perilunate instability complications include: median nerve neuropathy (25%), avascular necrosis of the carpal bones (20%), scaphoid non-union, persistent wrist instability, and arthitis.15
References / Further Reading
- Hunter TB, Peltier LF, Lund PJ. Radiologic history exhibit. Musculoskeletal eponyms: who are those guys? Radiographics. 2000;20(3):819-836. doi:10.1148/radiographics.20.3.g00ma20819.
- Padegimas EM, Ilyas AM. Distal radius fractures: emergency department evaluation and management. Orthop Clin North Am. 2015;46(2):259-270. http://www.ncbi.nlm.nih.gov/pubmed/25771320. Accessed June 2, 2015.
- Abraham MK, Scott S. The emergent evaluation and treatment of hand and wrist injuries. Emerg Med Clin North Am. 2010;28(4):789-809. http://www.ncbi.nlm.nih.gov/pubmed/20971392. Accessed August 7, 2015.
- Turner RG, Faber KJ, Athwal GS. Complications of distal radius fractures. Orthop Clin North Am. 2007;38(2):217-228, vi. http://www.ncbi.nlm.nih.gov/pubmed/17560404. Accessed August 7, 2015.
- Fowler JR, Hughes TB. Scaphoid fractures. Clin Sports Med. 2015;34(1):37-50. http://www.ncbi.nlm.nih.gov/pubmed/25455395. Accessed August 8, 2015.
- Loredo R a., Sorge DG, Garcia G. Radiographic evaluation of the wrist: A vanishing art. Semin Roentgenol. 2005;40(3):248-289. doi:10.1053/j.ro.2005.01.014.
- Goldfarb CA, Yin Y, Gilula LA, Fisher AJ, Boyer MI. Wrist fractures: what the clinician wants to know. Radiology. 2001;219(1):11-28. http://www.ncbi.nlm.nih.gov/pubmed/11274530. Accessed August 8, 2015.
- Waeckerle JF. A prospective study identifying the sensitivity of radiographic findings and the efficacy of clinical findings in carpal navicular fractures. Ann Emerg Med. 1987;16(7):733-737. http://www.ncbi.nlm.nih.gov/pubmed/3592326. Accessed August 8, 2015.
- Carpenter CR, Pines JM, Schuur JD, Muir M, Calfee RP, Raja AS. Adult scaphoid fracture. Acad Emerg Med. 2014;21(2):102-121. doi:10.1111/acem.12317.
- Vigler M, Aviles A, Lee SK. Carpal fractures excluding the scaphoid. Hand Clin. 2006;22(4):501-516; abstract vii. http://www.ncbi.nlm.nih.gov/pubmed/17097470. Accessed August 8, 2015.
- O’Shea K, Weiland AJ. Fractures of the hamate and pisiform bones. Hand Clin. 2012;28(3):287-300, viii. doi:10.1016/j.hcl.2012.05.010.
- Grabow RJ, Catalano L. Carpal dislocations. Hand Clin. 2006;22(4):485-500; abstract vi – vii. http://www.ncbi.nlm.nih.gov/pubmed/17097469. Accessed August 8, 2015.
- Budoff JE. Treatment of acute lunate and perilunate dislocations. J Hand Surg Am. 2008;33(8):1424-1432. http://www.ncbi.nlm.nih.gov/pubmed/18929215. Accessed August 8, 2015.
- Lohan D, Cronin C, Meehan C, Walsh S, Sheppard D, O'Keeffe D. Injuries to the Carpal Bones Revisited. Curr Probl Diagn Radiol. 2007;36(4):164-175. doi:10.1067/j.cpradiol.2007.03.002.
- Apergis E. Fracture-Dislocations of the Wrist.; 2013. doi:10.1007/978-88-470-5328-1.
- http://www.ncbi.nlm.nih.gov/pubmed/26113244
- http://www.ncbi.nlm.nih.gov/pubmed/25892722
- http://www.ncbi.nlm.nih.gov/pubmed/25738245
- http://www.ncbi.nlm.nih.gov/pubmed/25892729
- http://www.ncbi.nlm.nih.gov/pubmed/25441249





1 thought on “Wrist and Distal Forearm Injuries: Pearls & Pitfalls”
Pingback: emDOCs.net – Emergency Medicine EducationEM Boards Survival Guide: Orthopedics 1 - emDOCs.net - Emergency Medicine Education