
Welcome back to the “52 in 52” series. This collection of posts features recently published must-know articles. This week the series covers sensitivity of multi-slice CT for aneurysmal SAH at different timepoints.

Author: Brannon Inman (Chief Resident, Emergency Medicine Physician, San Antonio, TX) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Sensitivity of modern multi-slice CT for subarachnoid hemorrhage at incremental timepoints after headache onset: a 10-year analysis
Clinical question:
In patients with subarachnoid hemorrhage, what is the sensitivity of modern multi-slice CT scanners at incremental time points from time of symptom onset?
Study design:
- Single center retrospective analysis
PICO:
Population:
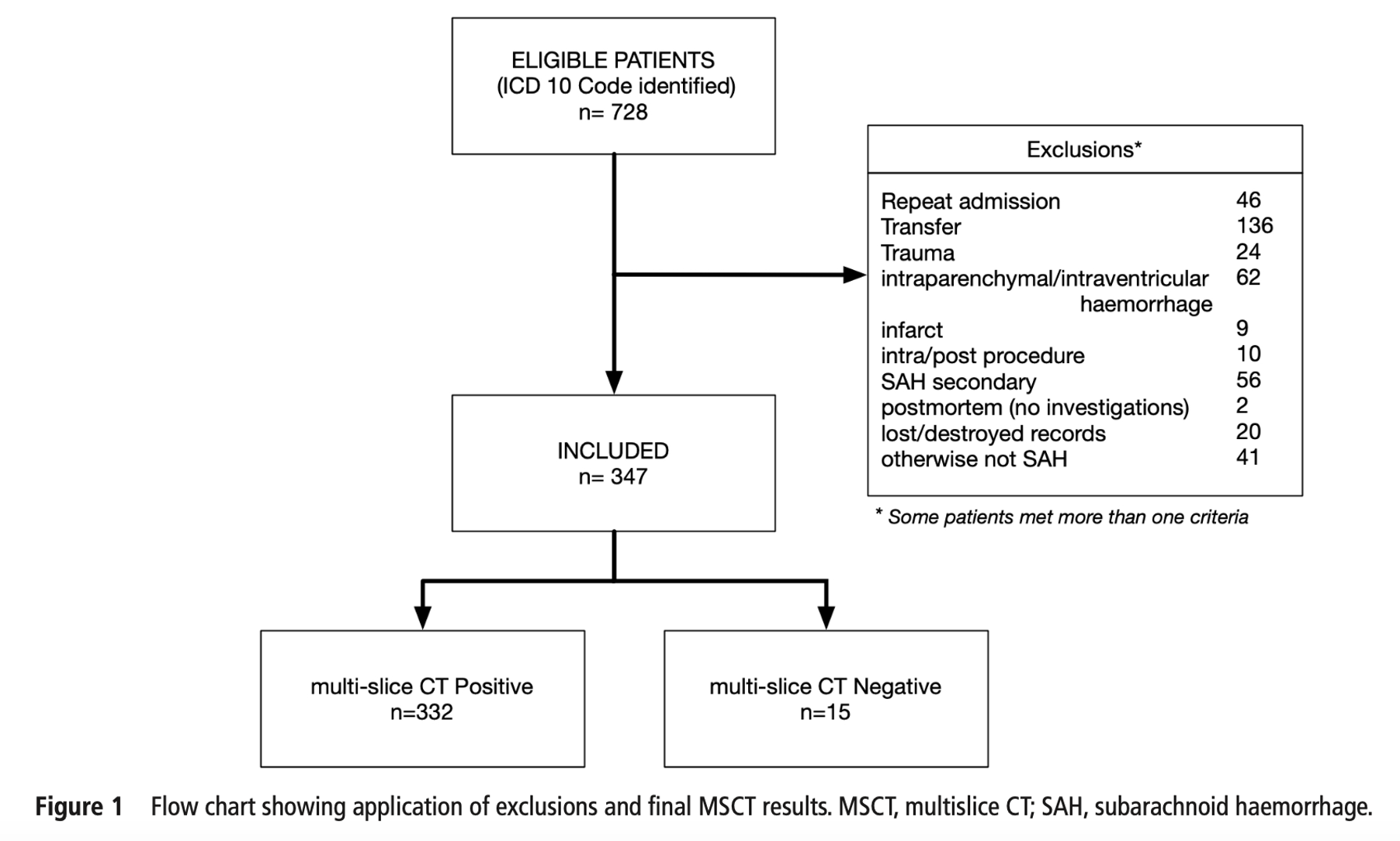
- Inclusion:
- Patients presenting to a single regional metropolitan ED in New Zealand, diagnosed with sub arachnoid hemorrhage (SAH) between 1 January 2008 and 31 December 2017
- Exclusion:
- Cases were miscoded as SAH (i.e., patient actually had a subdural, etc)
- Traumatic SAH
- Repeat admission/bounce back admission for SAH
- SAH was diagnosed on autopsy, but no CT scan was obtained
- Unknown time and date of onset
- Patient was transferred to the study site from another hospital
- Lost/destroyed records
- SAH was classified as being present if
- There was a coded ICD-10 diagnosis of SAH and
- if SAH was confirmed in the radiology report and medical records
Methods:
- Primary outcome was the proportion of patients with spontaneous aneurysmal SAH that had a positive CT.
- Secondary outcome was the proportion of patients with any cause for spontaneous SAH that had a positive CT.
- All patients during the study period were examined using either:
- A 128-slice MSCT (SOMATOM Definition Flash)
- A 64-slice MSCT (GE VCT Lightspeed)
- CT interpretation
- Head CT was considered as positive if there were high density material within the basal cisterns or subarachnoid space consistent with blood
- CT was considered indeterminate if there was degraded imaging, beam hardening, or motion
- CT was considered negative if there was an absence of high density material within the basal cisterns
- Patient Work up:
- During the study period patients initially had CT performed. If CT of the head was negative, a lumbar puncture (LP) was performed.
- If the CT or LP was positive for SAH, a CT angiogram was performed.
- In a non-standardized fashion, MRI/MRA would be performed if there was doubt about aneurysm or in attending physician preference.
- Authors handled missing time of headache onset using two approaches: one that maximized false negatives, and one minimized false negatives.
Outcome:
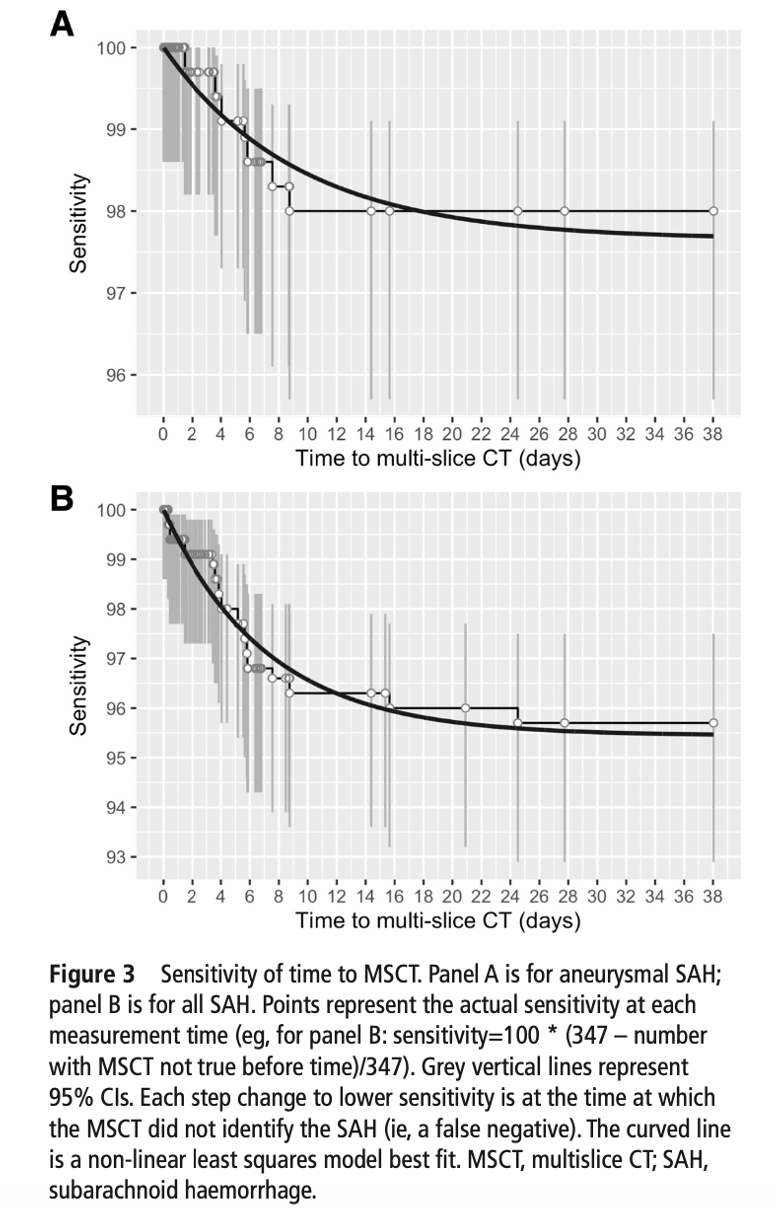
In the primary analysis (maximizing false negative rates) sensitivity was as follows:
- Sensitivity for aneurysmal SAH by time:
- At 6 hours sensitivity was 100% (98.0 to 100)
- At 12 hours sensitivity was 100% (98.2 to 100)
- At 24 hours sensitivity was 100% (98.3 to 100)
- At 48 hours sensitivity was 99.6% (97.6 to 100)
- At 72 hours sensitivity was 99.6% (97.6 to 100)
- At 96 hours sensitivity was 98.7% (96.4 to 99.7)
- Sensitivity for all cause SAH by time:
- At 6 hours sensitivity was 100% (98.3 to 100)
- At 12 hours sensitivity was 99.2% (97.2 to 99.9)
- At 24 hours sensitivity was 99.3% (97.5 to 99.9)
- At 48 hours sensitivity was 99.0% (97.1 to 99.8)
- At 72 hours sensitivity was 99.0% (97.2 to 99.8)
- At 96 hours sensitivity was 97.8% (95.5 to 99.1)

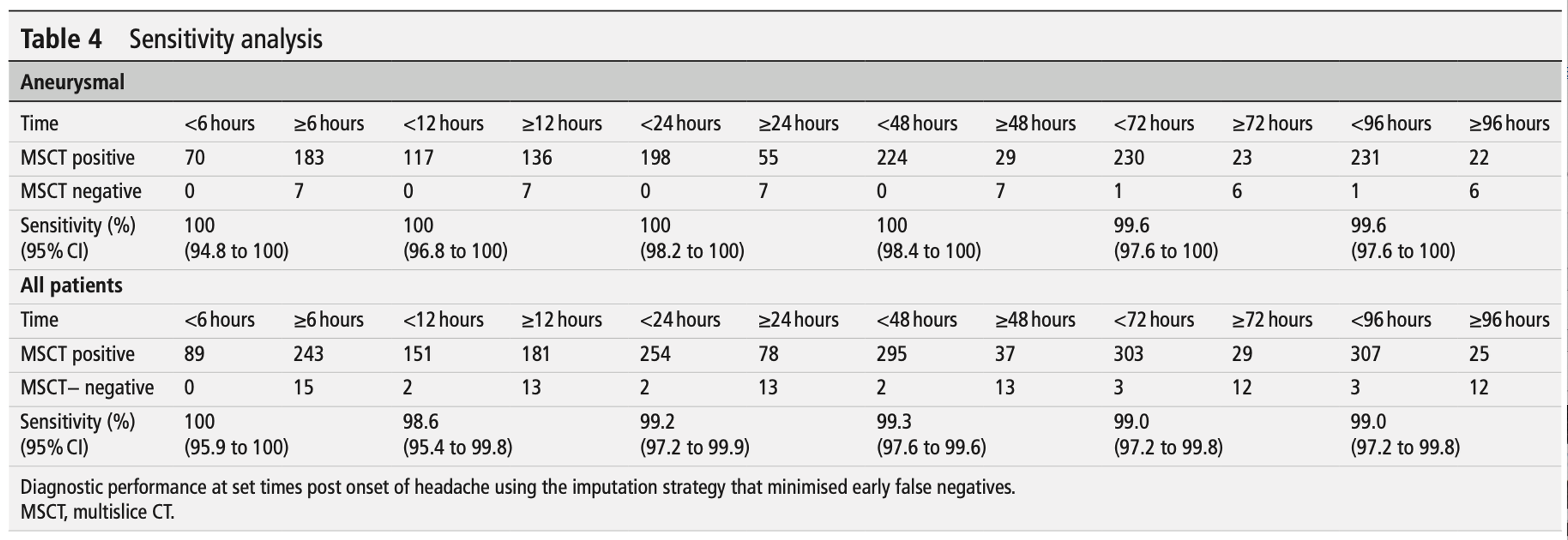
In the secondary analysis (minimizing false negative rates) sensitivity was as follows:
- Sensitivity for aneurysmal SAH by time:
- At 6 hours sensitivity was 100% (94.8 to 100)
- At 12 hours sensitivity was 100% (96.8 to 100)
- At 24 hours sensitivity was 100% (98.2 to 100)
- At 48 hours sensitivity was 100% (98.4 to 100)
- At 72 hours sensitivity was 99.6% (97.6 to 100)
- At 96 hours sensitivity was 99.6% (97.6 to 100)
- Sensitivity for all cause SAH by time:
- At 6 hours sensitivity was 100% (95.9 to 100)
- At 12 hours sensitivity was 98.6% (95.4 to 99.8)
- At 24 hours sensitivity was 99.2% (97.2 to 99.9)
- At 48 hours sensitivity was 99.3% (97.6 to 99.6)
- At 72 hours sensitivity was 99.0% (97.2 to 99.8)
- At 96 hours sensitivity was 99.0% (97.2 to 99.8)
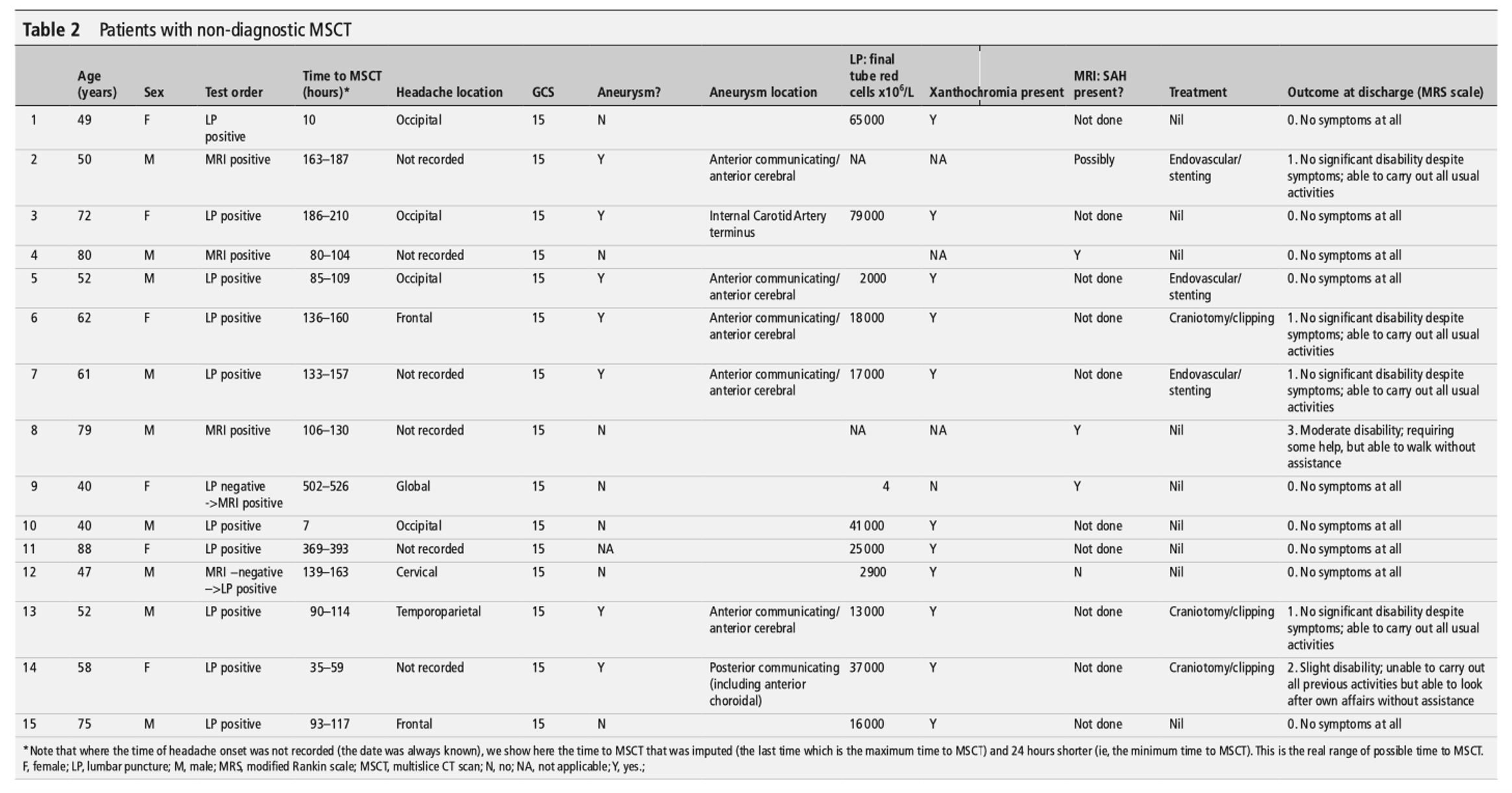
- 15 patients ultimately diagnosed with SAH had an initial negative head CT.
- All of these patients had a GCS of 15.
- For 11 of these patients, SAH was ultimately diagnosed on LP.
- Three of the patients had no LP performed.
- 14 of the patients were discharged from the hospital with no disability, and 1 was discharged with slight disability.
Take aways:
- This single center retrospective analysis showed a 100% detection rate for aneurysmal SAH on head CT performed within 24 hours of onset. Given that we generally do not know from the start of the encounter whether our patient has aneurysmal or non-aneurysmal SAH, the sensitivity for all cause SAH is probably more helpful (99.3% in the conservative analysis) than the reported 100% sensitivity reported for aneurysmal SAH .
- 15 patients in this 10-year period had a negative head CT and ultimately had SAH. 12/15 patients had LP performed after CT was negative.
- Chart review methods in the manuscript were limited; aside from ICD codes the chart review methods are not well described.
- The manuscript does not detail how they may have captured individuals who were discharged from the ED without a diagnosis of SAH. For example, in an individual discharged from the ED with a negative head CT snd a diagnosis of “headache” or “cephalgia” who may have ultimately died due to a SAH, it is not well outlined how this data would be captured. The text mentions that it excludes patients diagnosed on autopsy but did not have a head CT performed. However, it does not outline the patients who had a diagnosis of SAH on autopsy with a negative head CT and how it was incorporated into analytical calculations.
My take:
- This is a single center retrospective analysis offering promising data that noncontrast head CTs may have adequate sensitivity up to 24 hours of headache onset. However, I will not be incorporating this into my practice just yet.
- ACEP does support using a negative head CT within 6 hours of symptom onset to preclude the need for other diagnostic workup for SAH (Level B). I’m looking forward to more data on time windows past 6 hours.
References:
- Vincent A, Pearson S, Pickering JW, et al. Sensitivity of modern multislice CT for subarachnoid haemorrhage at incremental timepoints after headache onset: a 10-year analysis. Emerg Med J. 2022;39(11):810-817. doi:10.1136/emermed-2020-211068




