
Welcome back to the “52 in 52” series. This collection of posts features recently published must-know articles. This week we cover the EXTEND-IA TNK study, which evaluates TNK versus tPA before thrombectomy.

Author: Brannon Inman (Chief Resident, Emergency Medicine Physician, San Antonio, TX) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Tenecteplase versus Alteplase before Thrombectomy for Ischemic Stroke
AKA: EXTEND-IA TNK
Clinical question:
Is Tenecteplase (TNK) non-inferior to alteplase (TPA) in patients with anterior circulation strokes undergoing endovascular thrombectomy.
Study design:
- Investigator-initiated, multicenter, prospective, randomized, open-label, blinded- outcome trial
- Non-inferiority boundary of 4.6% (the maximum difference in effect between the new and established treatments that can be considered clinically acceptable was predetermined to be 4.6%)
- Assessment for the superiority of TNK would be performed if non-inferiority threshold was met
- Using logistic regression analysis, with adjustment for the site of vessel occlusion
PICO:
Population:
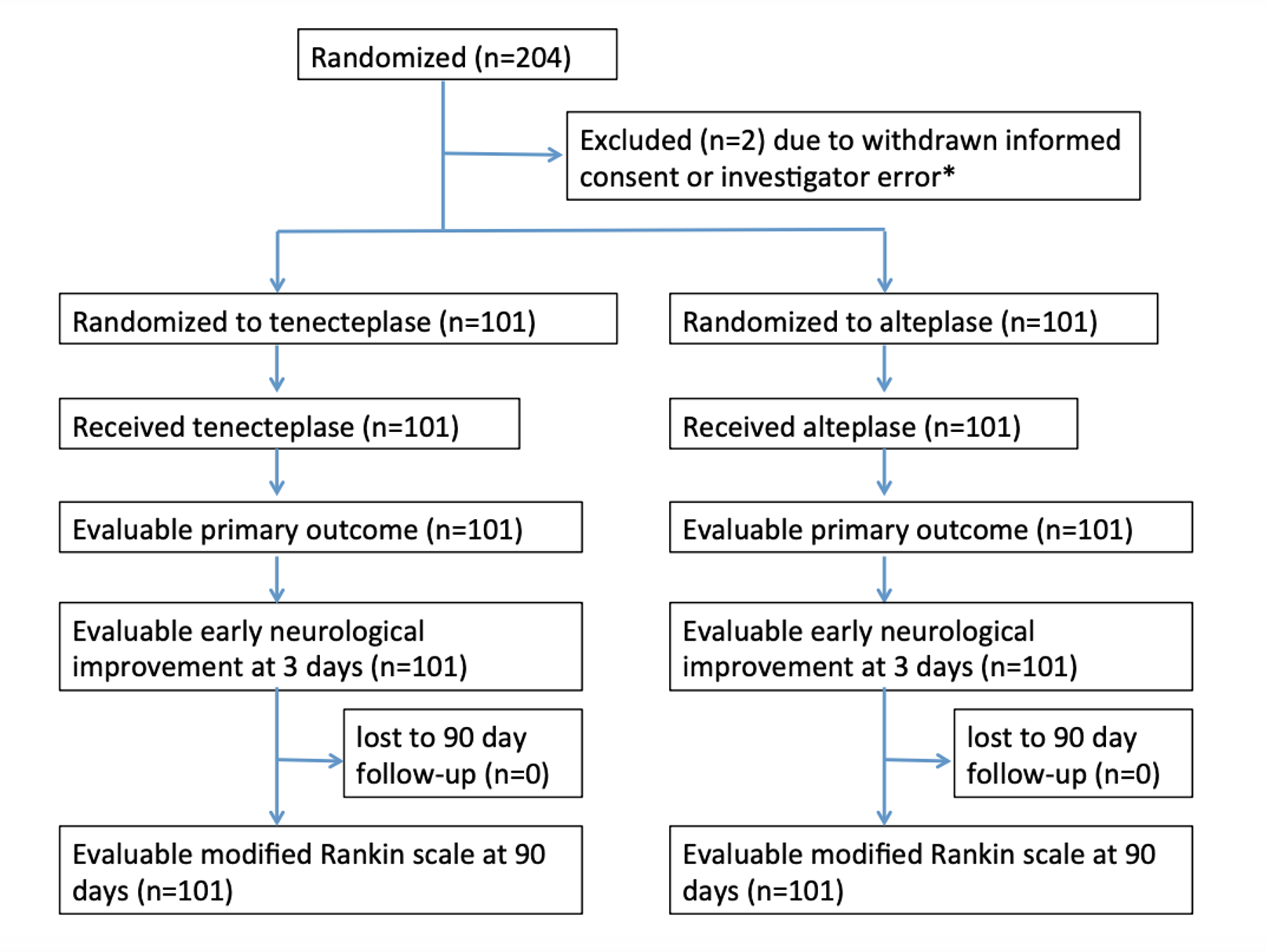
- Enrolled patients in at 13 centers in Australia and New Zealand
- Inclusion:
- Ischemic stroke within 4.5 hours
- Eligible to undergo IV thrombolysis and endovascular thrombectomy
- Evidence large vessel occlusion on CT angiography of the:
- Internal carotid artery
- M1 branch of the middle cerebral artery
- M2 branch of the middle cerebral artery
- Basilar artery
- Patient must have endovascular thrombectomy initiated (arterial access obtained) with in 6 hours of stroke symptom onset
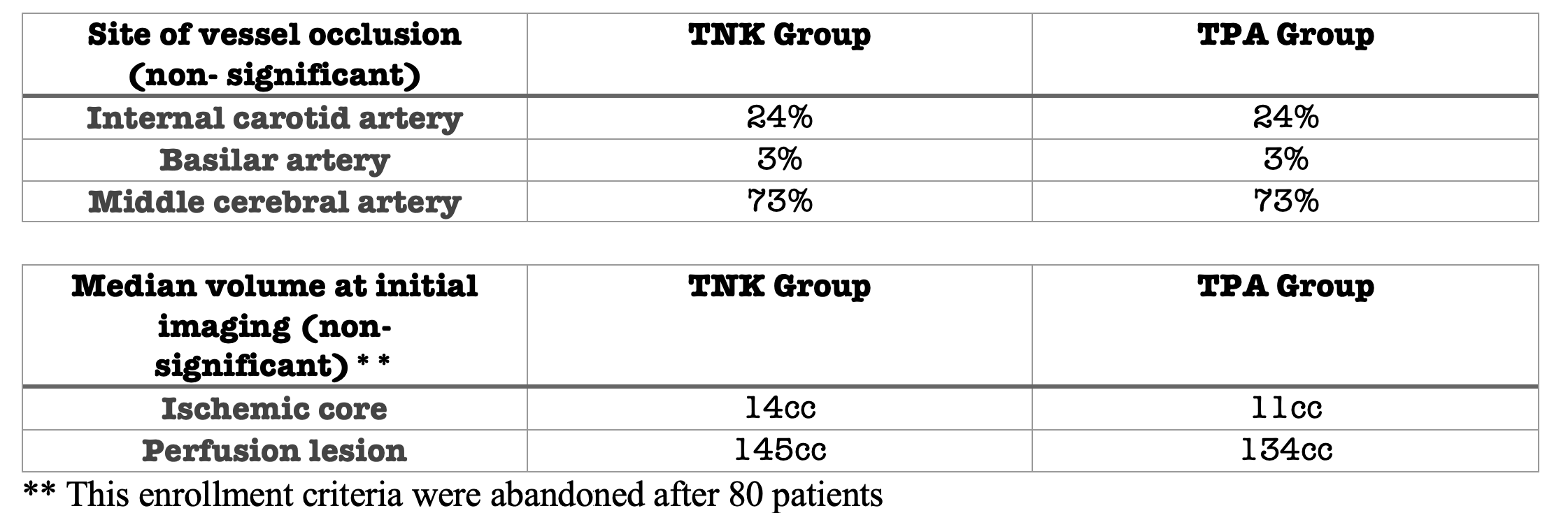
- Original inclusion criteria required CT-perfusion mismatch for anterior circulation strokes: Ratio of >1.2 between volume of hypoperfusion and the volume of the ischemic core, absolute difference in volume >10ml, ischemic core volume <70ml, which was removed after about 80 patients had been enrolled.
- Exclusion:
- Intracranial hemorrhage (ICH) identified by CT or MRI
- Rapidly improving symptoms at the discretion of the investigator
- Pre-stroke mRS score of ≥ 4 (indicating major previous disability)
- Hypodensity in >1/3 MCA territory or equivalent proportion of basilar artery territory on non-contrast CT
- Contraindication to imaging with contrast agents
- Any terminal illness such that patient would not be expected to survive more than 1 year
- Any condition that, in the judgment of the investigator could impose hazards to the patient if study therapy is initiated or affect the participation of the patient in the study.
- Pregnant women
Randomization:
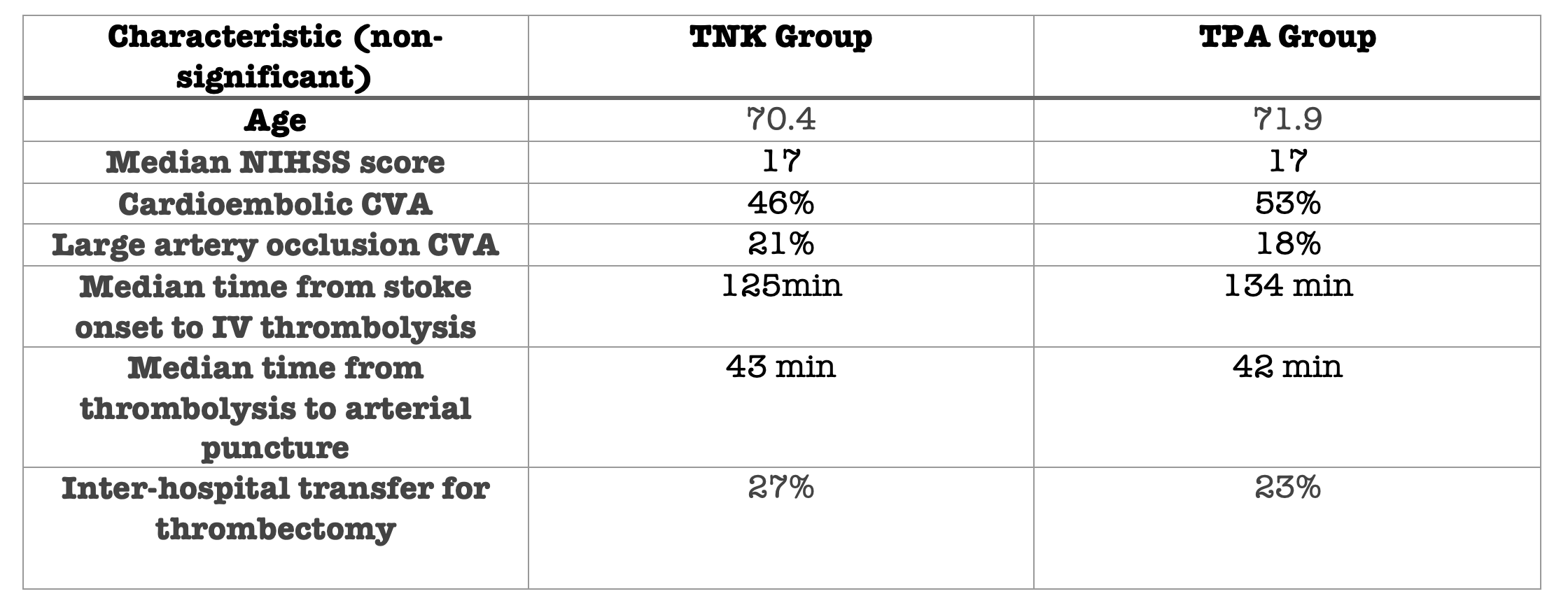
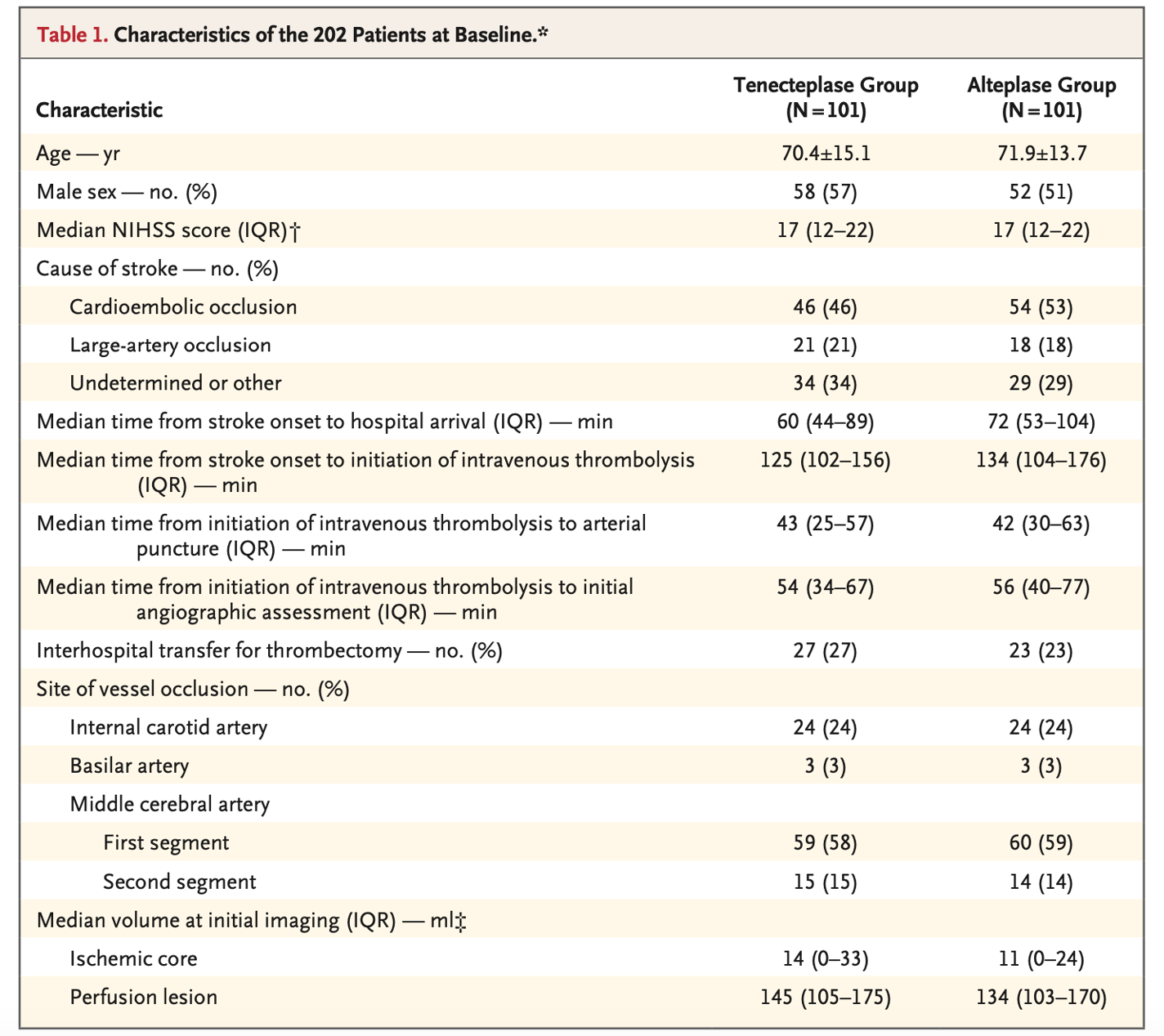
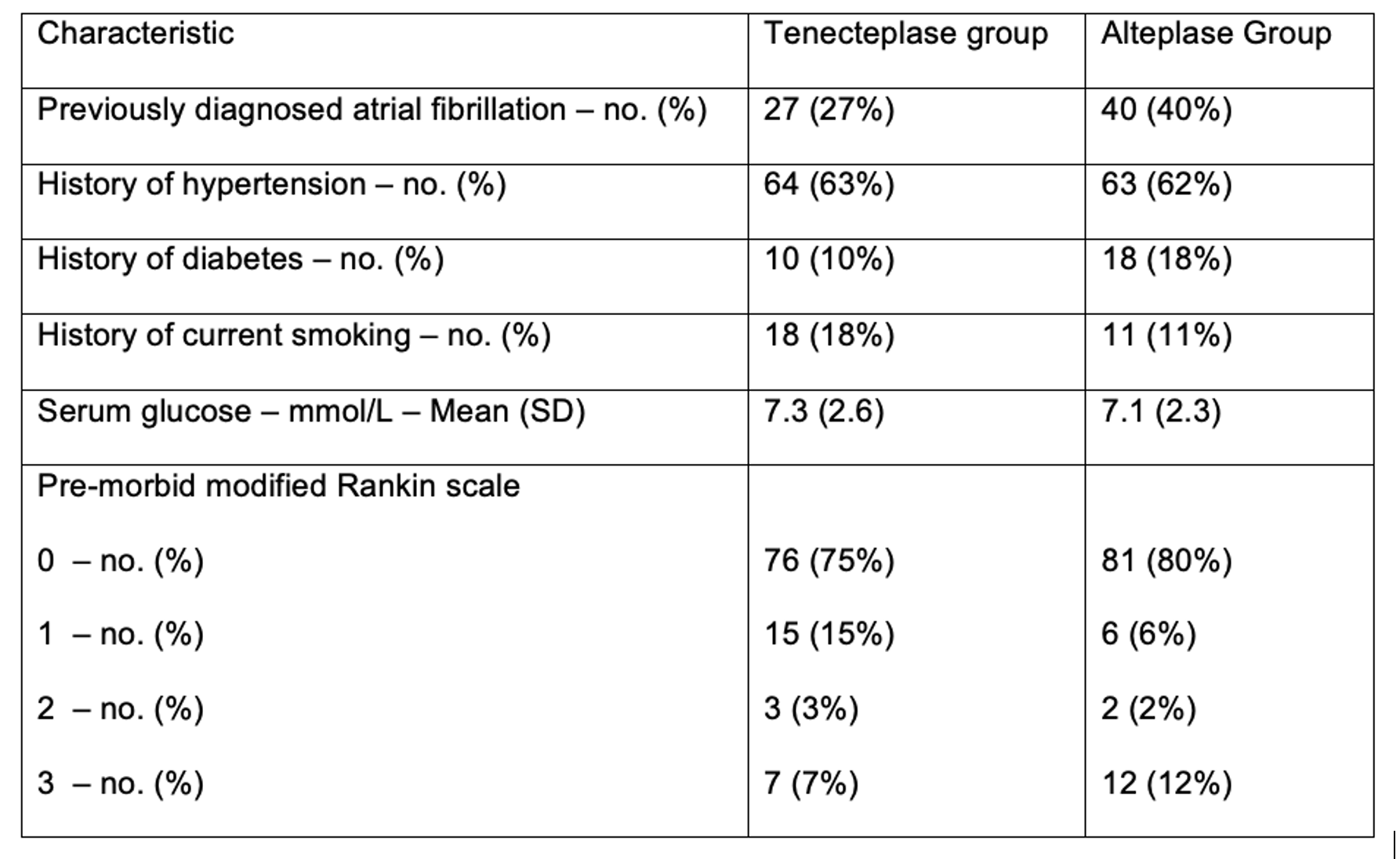
- There was a higher burden of preexisting A fib in the TPA group (supplemental text).
- Otherwise relatively balanced; Median NIHSS 17 in both groups.
- No significant differences in baseline characteristics
Intervention:
- Intravenous TNK
- 25 mg/kg; maximum dose 25 mg
Comparator:
- Intravenous TPA
- 9 mg/kg; maximum dose 90mg
Outcome:
Primary outcome:
- TNK was noninferior to TPA in reperfusion or absence of retrievable clot.
- 22% in TNK groups vs. 10% in TPA group
- Difference of 12% (95% C.I. 2-21), p=0.002 for non-inferiority
- Adjusted odds ratio for superiority 2.6 (95% C.I. 1.1-5.9), p=0.02
- Number Needed to Treat (NNT) = 9
- Fragility Index (FI) = 1
- Secondary outcomes:
- Statistically significant
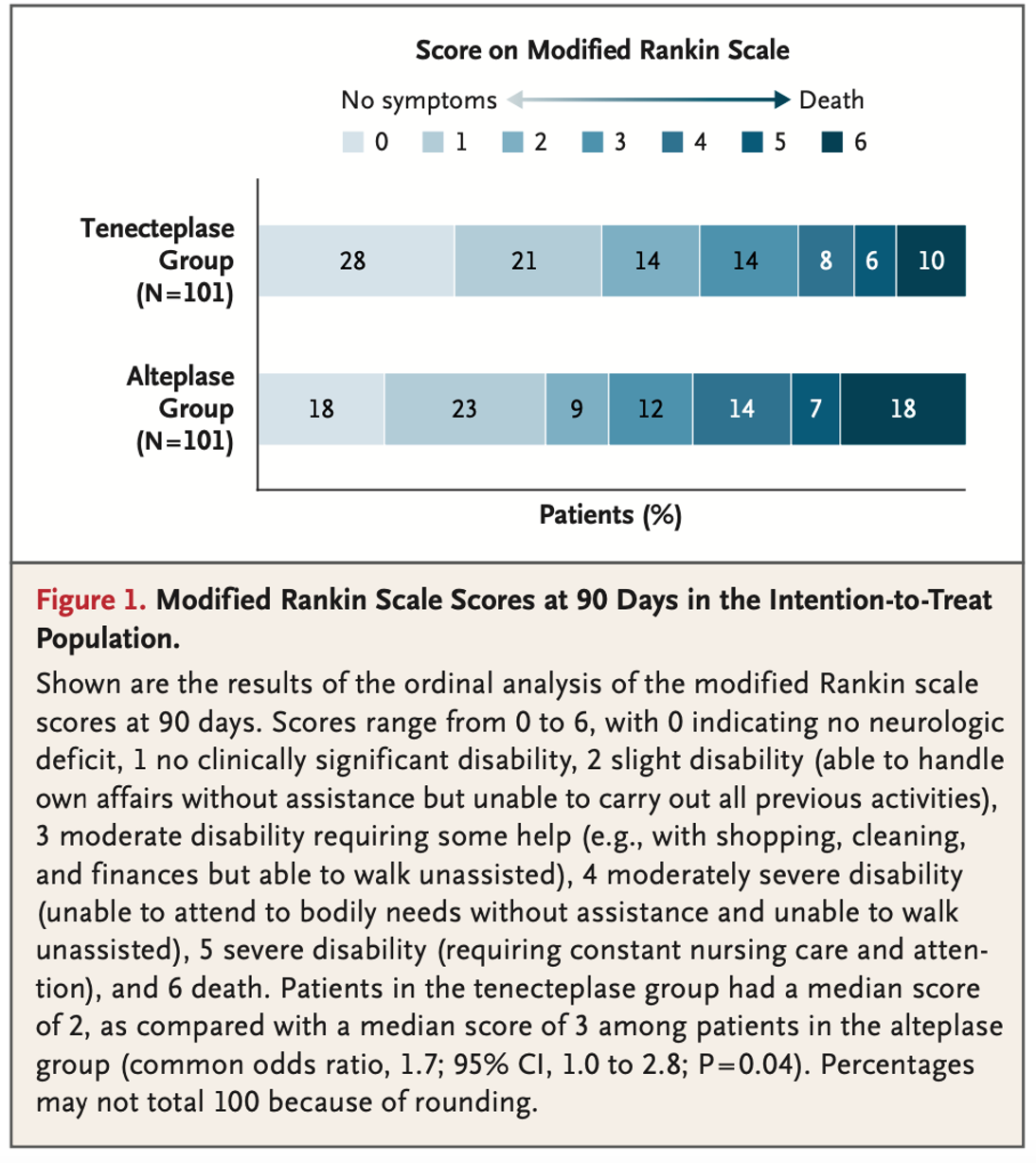
- Median modified Rankin Scale Score at 90 days: 2 (IQR 0-3) vs. 3 (IQR 1-5)
- OR 1.7, 95% C.I. 1.0-2.8, p=0.04
- Median modified Rankin Scale Score at 90 days: 2 (IQR 0-3) vs. 3 (IQR 1-5)
- Not statistically significant
- Early neurological improvement at 24 hours: Median NIHSS score 3 (IQR 1-12) vs. 6 (IQR 2-14), OR 1.4 (95% C.I. 1.0-1.9, p=0.06)
- Recovery to independent function (mRS 0-2, or no change from baseline) at 90 days: 64% vs. 51%, adjusted incidence ratio 1.2 (95% C.I. 1.0-1.5, p=0.06)
- Intracerebral hemorrhage: 1% vs. 1%
- Mortality: 10% vs. 18%, adjusted OR 0.4 (95% C.I. 0.2-1.1, p=0.08)
- Time to thrombectomy post initiation of thrombolysis: 54 vs. 56min
- Most patients who achieved reperfusion had a middle cerebral artery occlusion
- 20/22 patients in the intervention group vs. 6/10 patients in the control group
- Statistically significant

Take Aways:
- TNK is non-inferior to TPA for vessel re-cannulation and thrombus/embolus obliteration during index intervention.
- This was an open label study, and thus physicians and other staff were not blinded to randomization.
- As these patients were required to have arterial puncture within 6 hours of stroke onset, these data may not apply to patients who are not presenting to a stroke center. For example, a patient with an LVO stroke presenting to a hospital and needing transfer for endovascular thrombectomy, or a patient getting endovascular thrombectomy within 24 hours.
- Prespecified superiority analysis suggests TNK may result in better functional outcomes. However, ultimately this study was powered and conducted as a non-inferiority study, so this is only hypothesis-generating.
- This study did change its enrollment criteria after 80 patients were already enrolled.
- There existed a substantively larger proportion of patients with MCA occlusion in the TNK arm. Given the smaller infarct territory, this could reasonably be expected to have consequential impacts on long term outcomes.
My take:
- These data suggest TNK is non-inferior to TPA for patients requiring thrombectomy for anterior circulation LVO undergoing thrombectomy. Given the ease of use and pharmacodynamics, I would favor use of TNK over TPA for this patient population.
Source Article:
- Campbell BCV, Mitchell PJ, Churilov L, et al; EXTEND-IA TNK Investigators. Tenecteplase versus Alteplase before Thrombectomy for Ischemic Stroke. N Engl J Med. 2018 Apr 26;378(17):1573-1582. doi: 10.1056/NEJMoa1716405. PMID: 29694815.




