
Author: Lloyd Tannenbaum, MD (EM Attending Physician, APD, Geisinger Wyoming Valley, PA) // Reviewer: (Brit Long, MD (@long_brit)
Hello and welcome back to ECG Pointers, a series designed to make you more confident in your ECG interpretations. This week, we feature a post from Dr. Tannenbaum’s ECG Teaching Cases, a free ECG resource. Please check it out. Without further ado, let’s look at some ECGs!
Operator: 911 what’s your emergency?
Frantic shouting: Hello?? HELLO?! Help help! My wife. She’s not breathing! Send an ambulance quick! Help!! I don’t think I feel a pulse!
Operator: Sir, Sir! What happened? I’m dispatching police and EMS to your location now; can you tell me what’s going on?
Far away shouting: Tell them to hurry! I’m starting CPR!
*********
“This is Medic 10. We are 5 minutes out. Coming to your location priority one, hospital, do you copy?”
You and your charge nurse, Shannon, hustle over to the EMS phone. It’s never good when they’re coming in priority one. “Go ahead Medic 10, hospital standing by.”
“Hey Doc, this is Medic 10. We have a 36-year-old female coming to you from home. Husband woke up to her having agonal respirations. He called 911 and started CPR. We arrived on scene and found the husband distraught, actively performing CPR. We took over, got her hooked up to monitor and found her in ventricular fibrillation. She was still agonally breathing. We defibrillated her immediately and continued CPR. Got access, gave epi and got her tubed. After a few rounds of CPR and I think 3 shocks, we got ROSC. We got her loaded onto the truck and lost pulses again. Another 2 shocks and an amiodarone bolus got ROSC again. BP soft at 90/36 but holding. We are pulling in now, see you in a sec. Medic 10 clear.”
You and Shannon give each other the look that says, “That’s not good” and hustle to get set up. “I’ll call respiratory to get a vent ready, can you let pharmacy know we’ll need them in bed 10?” you ask Shannon.
“Sure, Doc, I’ll let Scott know we need him. Hope you’re ready, that’s the ambulance doors opening.”
You see Medic 10 moving fast, bringing in an ill appearing female, the LUCAS device still on her chest, but not actively performing CPR.
“Hey Doc! We came as fast as we could. Not a ton more to tell you than we did over the radio. No idea why she arrested. According to her husband, no history of high blood pressure, high cholesterol, diabetes, or anything! She doesn’t smoke, drink or use drugs. He says she’s very healthy, goes to the gym 3-4 times a week. Was complaining of chest pain for the past 2-3 days but kept brushing it off. Keep us posted on what you find! Moving her over to your bed in 3 .. 2.. 1.. Good luck doc!”
“Thanks Medic 10. Ok team, let’s get her hooked up to the monitors and get a set of vitals. It’s also been about 10 minutes since Medic 10 got ROSC, let’s get an ECG and see what’s going on.
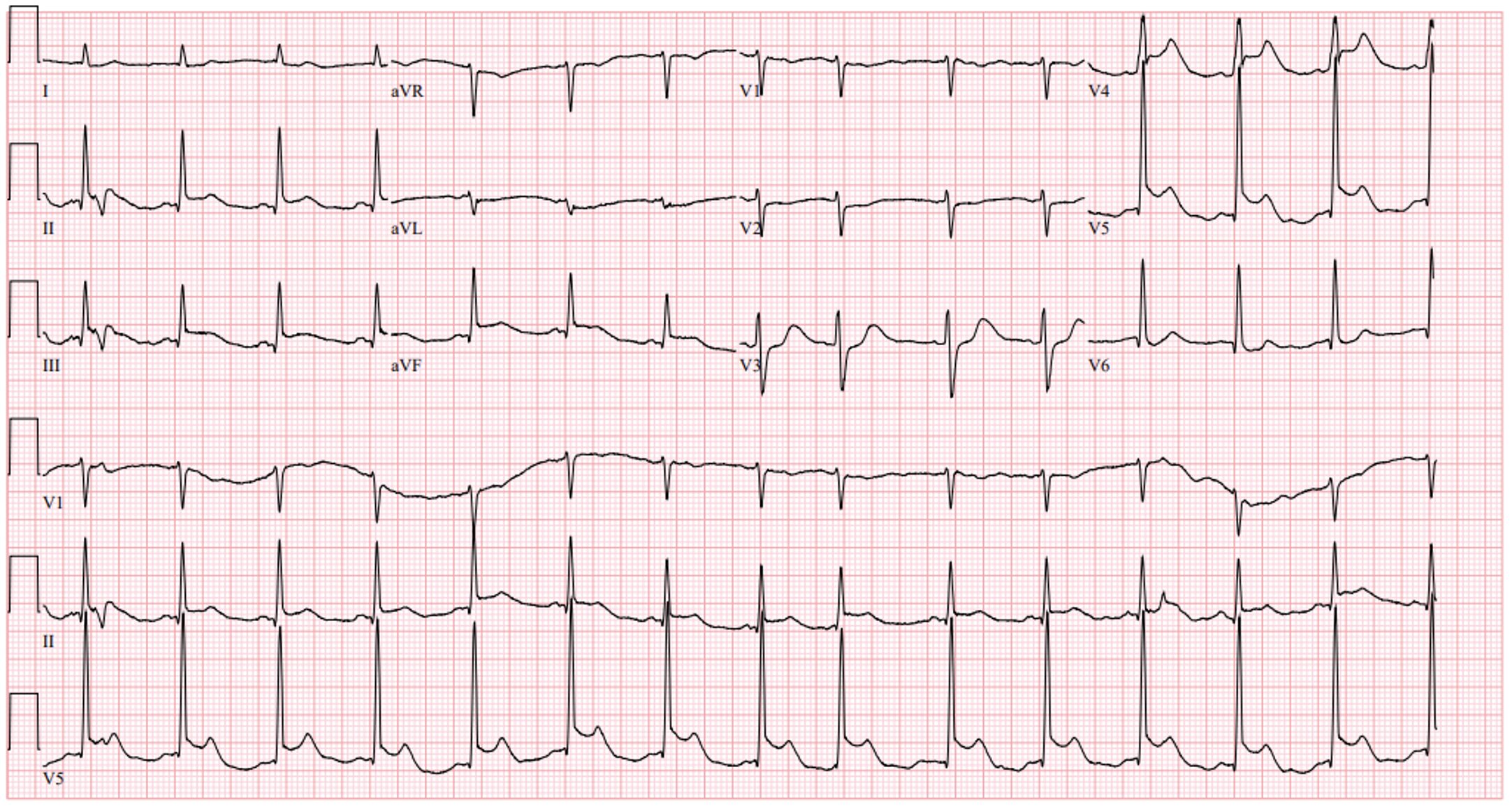
Rate: 95
Rhythm: Normal sinus rhythm
Axis: Normal
Intervals: Normal PR, narrow QRS, QTc looks reasonable, intervals look good.
Morphology: There is ST segment elevation in leads II, III and aVF and V4/V5. There is a slight amount of ST segment depression in V3
Final read: This ECG is concerning for an Inferior MI! Given the ST elevation in V4/V5, there is likely some lateral involvement too.
“Doc, vitals show a heart rate of 95, BP is 100/42, RR of 18 on the vent, 99% on 70% FiO2, afebrile. Glucose is 126. How does that ECG look?”
“It looks like an inferior STEMI. I just texted interventional cards, they’re going to rush her to the lab.”
*********
What a whirlwind adventure! But, why would a 36-year-old otherwise healthy female have a STEMI? Maybe bad genes? Or could there be another process going on?
Well, On November 12th, 1930, Dr. Harold Pretty was called to see one of his patients who had become ill at home after eating at a neighborhood fish fry. His patient, who he had known for most of her life, had been previously healthy with no chronic medical conditions. She had nausea and vomiting, was given symptomatic treatment, and diagnosed with a stomach illness, likely from the fish fry. After symptomatic treatment, she was doing better and seemed to be recovering well. Then, at 3 am on the 13th, Dr. Pretty was called emergently back to the patient’s home, as she had woken up, complained of severe chest pain, vomited once, and then suddenly died. She was only 42 years old.
Shocked, Dr. Pretty performed an autopsy later that day. The patient’s abdomen was fine, but when he opened up the pericardium, it was full of blood. Further examination revealed that the right coronary artery had developed a dissecting aneurysm which had burst into the pericardium. This case was published in the British Medical Journal, and can be found here (Reports of Societies | The BMJ). This was one of the first case reports of Spontaneous Coronary Artery Dissection (SCAD)!
Spontaneous Coronary Artery Dissection is a nonatherosclerotic, nontraumatic cause of acute coronary syndrome. Interestingly, 87-95% of SCAD cases affect females and the average age at presentation is between 44-53 years old. Most of the information in this write up comes from an awesome review by the Journal of the American College of Cardiology, which can be found here (Spontaneous Coronary Artery Dissection: JACC State-of-the-Art Review – PubMed). SCAD was initially considered extremely rare, but recent reviews have found it more prevalent than previously believed. Some studies have reported that SCAD is responsible for up to 4% of all cases of ACS and 35% of ACS cases in women under 50!
One major risk factor for SCAD is pregnancy. Most patients who have pregnancy associated SCAD are postpartum and present within one week of giving birth. These patients tend to have severe complications, such as impaired LV function, shock, and multivessel disease. Between 5-17% of SCAD cases are associated with pregnancy and SCAD affects around 1.8/100,000 pregnant women.
SCAD patients often present exactly like a typical ACS patient. They can have crushing chest pain, diaphoresis, and vomiting. They’ll often have elevated troponins and ischemic changes on ECG. As with our patient today, they can have ventricular dysrhythmias, shock, or even sudden cardiac death. Because they have minimal or no risk factors for “typical” ACS, these patients can be minimized, so keep a high index of suspicion to make sure they get optimal care.
What do we do with these patients? Do they still need a cath? Yes, sorta! The patients need to go to the cath lab to have coronary angiography. However, once SCAD is diagnosed, treatment differs from traditional PCI for atherosclerotic lesions. SCAD patients are at high risk for multiple complications during cath, including abrupt vessel occlusion, iatrogenic dissection, hematoma propagation, and vessel rupture. None of this sounds good. What we’ve seen in recent literature is that, when these patients do not have high risk features (ongoing chest pain, ischemia, left main artery dissection, ventricular dysrhythmias, or hemodynamic instability), they do well with medical management. Let’s dive into that a bit more with this article, (Spontaneous Coronary Artery Dissection (SCAD) from an Interventionalist Perspective – PubMed) titled, “Spontaneous Coronary Artery Disease from an Interventionalist Perspective published in Current Cardiology Reports in 2024.
This report notes that initial ER management of SCAD is the same as atherosclerotic ACS. We give anticoagulation, antiplatelet meds and activate the cath lab. Interestingly, thrombolytics are CONTRAINDICATED in SCAD, but current guidelines recommend anticoagulation and antiplatelet therapy in the ER. That being said, once SCAD is diagnosed, anticoagulation should be stopped. The authors then cite three reasons why a conservative approach is favored over an aggressive interventional approach. First, most medically managed SCAD lesions heal on their own within 30 days (as seen on repeat imaging). Secondly, if another SCAD lesion were to recur, it is typically in a different location or vessel, so stenting does not prevent future dissections. Finally, PCI is extremely difficult and technically challenging in these patients.
What about high-risk patients? Recall, patients with an occluded vessel, ongoing cardiac ischemia, dysrhythmias, or hemodynamic compromise are considered high risk with respect to SCAD. These patients will need intervention, but the goal is to just restore TIMI grade 3 flow, not restore coronary structure, as with atherosclerotic lesions. Remember, this is a high-risk PCI. They are associated with significantly higher rates of complications and failures, with PCI failure being reported as high as 53%!
So, if PCI fails and the patient is still critically ill, what can we do? Coronary Artery Bypass Grafting (CABG) would be considered as a last-ditch effort, but is often wrought with complications, possibly due to grafting with damaged vessels. Despite the severity of this disease, in-hospital mortality is relatively low (1.4-3%) and long-term mortality is also fairly low with a 3-year mortality rate of 0.8%.
Case Wrap Up:
The patient was taken upstairs to the cath lab where coronary angiography showed a wrap-around LAD (an LAD also supplying the inferior wall) with a SCAD lesion in the distal portion. Anticoagulation was stopped and no stents were placed during the cath. She was transferred to the ICU for further medical management.
Recap:
- Yes, young healthy females can have heart problems!
- Spontaneous Coronary Artery Dissection should be on your differential for a young, healthy female who presents with ACS.
- SCAD is associated with pregnancy and is most often seen in the first week postpartum period.
- From the ER’s point of view, these patients should be treated like a “normal” STEMI and given antiplatelet and anticoagulation, per your hospital’s guidelines.
- If you somehow know that it’s SCAD, DO NOT give thrombolytics, as they are contraindicated.
- Once SCAD is diagnosed in the cath lab, anticoagulation can be discontinued.
- A “less is more” approach appears to be the best management for SCAD patients, as PCI is often fraught with complications.
- Intervention should be reserved for high-risk patients.
- When managed medically, SCAD lesions often heal on their own.





