
Author: Lloyd Tannenbaum, MD (EM Attending Physician, APD, Geisinger Wyoming Valley, PA) // Reviewer: Brit Long, MD (@long_brit)
Hello and welcome back to ECG Pointers, a series designed to make you more confident in your ECG interpretations. This week, we feature a post from Dr. Tannenbaum’s ECG Teaching Cases, a free ECG resource. Please check it out. Without further ado, let’s look at some ECGs!
“TRAUMA TEAM TO THE TRAUMA ROOM, TRAUMA TEAM TO THE TRAUMA ROOM” the hospital voice calls out.
“Hey Shannon, what’s coming in?” you ask your charge nurse as you hustle over to the trauma bay and glove up.
“Well doc, it doesn’t sound great. 75-year-old male in a motor vehicle roll over. He’s complaining of severe back pain and can’t move his lower extremities. EMS has him fully immobilized and they should be here any second…
“Hey Doc!” the paramedics call out as they come into the bay, “This is Justin, he’s a 75-year-old male who was in a pretty severe MVC. He flipped his car and has severe back pain. Cannot move his legs or feel anything below roughly his umbilicus. We’re very worried about a cord injury. We have him completely immobilized. He was a prolonged extrication. Let’s carefully get him moved over to your bed in 3 … 2 … 1… Good luck guy. We’ll call in a bit for follow up.”
“ABCs intact! Patient is speaking in complete sentences with a GCS of 14. He’s a little confused. I have good bilateral breath sounds and a strong radial pulse.” you hear the trauma intern call out.
“I have a manual pressure of 60/31” you hear your tech call out.
“60/31?! Are you sure? Please check it again.” You ask.
“Repeat manual pressure is 63/27” the tech calls out.
“What are the rest of the vitals, please?” you ask.
“Heart rate is 67, blood pressure is 63/27, Respiratory rate is 18, SpO2 is 100% on RA and GCS is 14, he loses one for confusion.
“Please call out the physical exam!” you call to your resident.
“Bilateral upper extremity strength is 5 out of 5. Both lower extremities are flaccid. He has normal sensation down the chest until an inch or two above the umbilicus. After that, no sensation. Along the spine, there feels like there is a step off in the mid thoracic region and the patient has no rectal tone,” The resident tells you.
You and the trauma attending look at each other. “That’s not good.” You both think.
“Intern!” you hear the trauma attending call out, ‘Explain to me why this patient’s blood pressure is low and your plan to fix it!”
“Yes Sir!” You hear the trauma intern call out. “I am worried about a spinal cord injury. I think his low blood pressure is due to the injury and we need to treat it with pressors.”
“Give me a little more,” the trauma attending says. “Why does a spinal cord injury cause hypotension and what’s the first line pressor?”
Great questions, you think to yourself. One of the techs hands you this ECG to interpret as you watch the EM intern and the trauma intern exchange glances and look to the senior resident for help. Let’s read this quick while the patient get a CT scan and then listen in on her explaining shock secondary to a spinal cord injury.
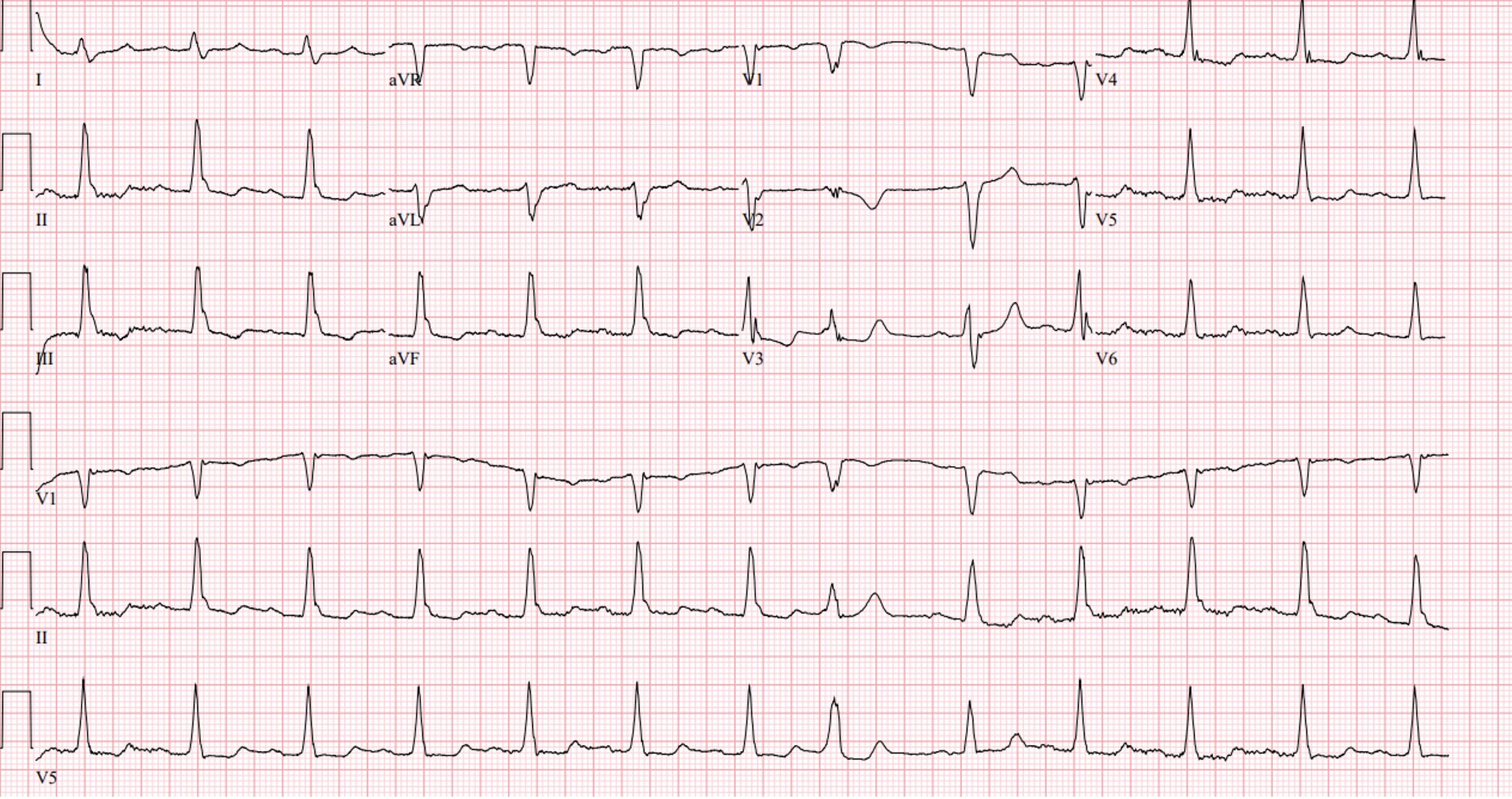
Rate: 75
Rhythm: Normal sinus
Axis: Normal
Intervals: overall pretty good. Normal QRS duration, no 1st deg AV block, QTc looks overall ok
Morphology: Again, pretty good. Some nonspecific ST-T wave changes, like T wave inversions in some of the inferior leads, but not terrible overall, especially for 75 years old
Final Read: Normal sinus rhythm
“Ok guys, listen up, we don’t have a lot of time before the trauma attending notices I’m going over this with you.” You hear the senior resident start to explain…
(Note, in 2024, the Global Spine Journal put out a paper called, “Clinical Practice Guidelines for the Management of Patients with Acute Spinal Cord Injury: Recommendations on Hemodynamic Management” which can be found here. Most of the information in this write up comes from that paper)
“In 2013, the American Association of Neurological Surgeon and the Congress of Neurological surgeons put out guidelines for the management of acute cervical spine and spinal cord injuries (which can be found here). One of the major recommendations to come out of that paper was that patients who have an acute spinal cord injury should have a MAP between 85 to 90 for 3-7 days to make sure that the spinal cord has adequate perfusion. As you can imagine, it is incredibly challenging to keep a MAP strictly between 5 points for 3-7 days, especially after a spinal cord injury. The Global Spine Journal article attempted to look at new evidence and find a better MAP goal. They also sought information on the best pressor to recommend for patients in shock due to do a spinal cord injury.” She begins.
“After reviewing the available literature, the writers recommend keeping the MAP between a lower limit of 75-80 and an upper limit between 90-95 to optimize spinal cord perfusion (see editor note below). They also recommended maintaining this MAP goal for 3-7 days. There really weren’t a lot of studies to base this on, so they note a very low quality of evidence and acknowledge this is a weak recommendation.” She continues. “Finally, in terms of a specific pressor, the authors left that up to the attending physician, as they noted no studies showing a definitive pressor of choice.”
“Taking pressor of choice one step further, there was an article published in the Journal of Intensive Care Medicine in 2025 called ‘A Guide to the Use of Vasopressors and Inotropes for Patients in Shock.’ For neurogenic shock, they note that traditionally 3 different pressors, dopamine, norepinephrine, and phenylephrine, are traditionally used. They cite a small trial of 11 patients showing that norepinephrine was able to maintain MAP with a lower intrathecal pressure and higher spinal cord perfusion pressure compared to dopamine. Another review shows higher complications of dopamine in spinal cord injury patients as compared to phenylephrine. Finally, a recent review suggests that norepinephrine may be the pressor of choice for these patients, however, due to a lack of high quality evidence, the authors agree with the prior paper and leave pressor of choice up to the attending physician,” she concludes.
“OK enough helping!” you hear the trauma attending call out. Now, intern, take a look at the CT scan and tell me about why this patient is in shock and what’s causing it?”
“Uhh… well…” you hear him start to stutter. “Neurogenic shock is a form of distributive shock. It often occurs when there is damage to the spinal cord causing a loss of sympathetic control of the vascular tone. It’s usually seen due to injuries at or above T6.”

“What I’m seeing on CT appears to be a T6 burst fracture with significant bleeding around the fracture and protrusion into the spinal canal…” the intern finishes.
“That’ll do intern,” the trauma attending cuts in. “Get on the phone with Neurosurgery and get this patient admitted to the surgical ICU.” The trauma attending adds as he walks off.
Case Wrap Up
For real life advice on these patients, I reached out to my friend and neurosurgeon, Dr. Tony Stefanelli. Dr. Stefanelli works in Philadelphia and specializes in complex spinal procedures. When I ran this case by him and asked what he would consider recommending for a patient like this, he suggested keeping the map between 85-100 for 5-7 days. Personally, he likes to use norepinephrine as his pressor of choice, and he recommends against giving these patients steroids, which have not demonstrated improved patient outcomes. Thanks Tony!
Recap:
- Neurogenic Shock is caused by a spinal cord injury leading to loss of sympathetic control of vascular tone.
- It is a form of distributive shock.
- Often due to an injury above T6.
- Pressor of choice in neurogenic shock remains understudied and at the discretion of the attending physician, with most preferring phenylephrine or norepinephrine.
- After an injury, prior guidelines recommended keeping MAP between 75-80 up to 90-95 for 3 to 7 days; however, the guidelines admit that this is a weak recommendation based on not very many studies. See editor note below.
- More data are needed to determine how to best care for these complex patients
- Thanks for your insights Dr. Stefanelli!
Editor Note: A 2025 RCT including 92 patients with spinal cord injury randomized patients to augmented (>85-90 mm Hg) or conventional (>65-70 mm Hg) MAP for 7 days or until ICU discharge. Authors found no mean differences in change from baseline in upper extremity motor scores (34.95 [3.25] vs 32.95 [3.65]; difference, 2.48; 95% CI, −5.93 to 10.90; P = .55), lower extremity motor scores (18.53 [4.62] vs 19.95 [4.59]; difference, −4.56; 95% CI, −16.11 to 7.03; P = .43), or total sensory scores (108.47 [12.49] vs 130.89 [14.87]; difference, −32.00; 95% CI, −65.40 to 1.40; P = .06) between the groups. The augmented group had higher mean modified SOFA scores (excluding cardiovascular components) at day 3 (1.65 [1.79] vs 0.80 [1.10]; difference, 0.85; 95% CI, 0.23-1.47; P = .008) and day 6 (1.55 [1.82] vs 0.80 [1.35]; difference, 0.74; 95% CI, 0.05-1.44; P = .04), longer mechanical ventilatory support (9.44 [15.27] vs 3.78 [8.42] days; difference, 5.67 days; 95% CI, 0.48-10.85 days; P = .03), and more respiratory complications (36 [78%] vs 18 [39%]; risk difference, 40%; 95% CI, 22%-58%; P < .001) than the conventional group. This study requires further validation, but it calls into question targeting higher MAP.




