
Authors: Mikella Washburn, MD (EM Resident Physician / University of Missouri- Columbia); Jessica Pelletier, DO, MHPE (APD/Assistant Professor of EM/Attending Physician, University of Missouri-Columbia) // Reviewed by: Sophia Görgens, MD (EM Physician, Yale University, CT); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 24-year-old female G4P1 who is 9 weeks pregnant by last menstrual period presents to the ED with abdominal pain and vaginal bleeding. She reports the abdominal pain is in the bilateral lower quadrants and describes it as “cramping.” She endorses vaginal bleeding with passage of clots for 3 days.
Vital signs include HR 115, BP 100/76, T 38.7, RR 13, SpO2 99% on RA. She is ill-appearing and has tenderness to palpation of the bilateral lower quadrants and suprapubic region. Pelvic exam reveals blood in the vaginal vault and foul-smelling discharge from the cervix with no other abnormalities.
What is the diagnosis?
Answer: Septic Abortion
Background:
- Definition: Infection of uterine products (including placenta and fetal tissue) in the setting of a terminated pregnancy (whether iatrogenic or spontaneous).1
- Common cause of pregnancy-related mortality.
- More commonly secondary to spontaneous and unsafe abortions as compared to medically-induced abortions.2
Etiology:
- Ascension of bacteria from the vagina into the uterus, which can then be followed by invasion into the decidua of endometrium/myometrium.1
- Invasion into myometrium can occur as quickly as 6 hours.
- Often polymicrobial secondary to normal vaginal flora.2
- Most commonly occurs after unsafe abortion due to introduction of new bacteria into vagina/cervix or cervical/uterine trauma from instrumentation; however can also occur after spontaneous or medication-induced abortion.1
Epidemiology:
- Septic abortion is the second most common serious complication of abortion after hemorrhage.1
- Prevalence varies widely.
- It is a significant cause of mortality after induced and spontaneous abortion.
- Increased rate of septic abortion seen in developing countries, likely secondary to:
- More unsafe abortions are attempted by patients and unlicensed personnel, and
- Scarcity of physicians able to surgically remove retained products of conception after incomplete spontaneous or unsafe abortion.
Clinical Presentation:1
- Most common signs and symptoms: fever, vaginal bleeding.
- Other common signs: abdominal pain, uterine tenderness (often times less tender than you might expect).
- Signs of sepsis: hypotension, fever, changes in mentation, tachycardia, oliguria.
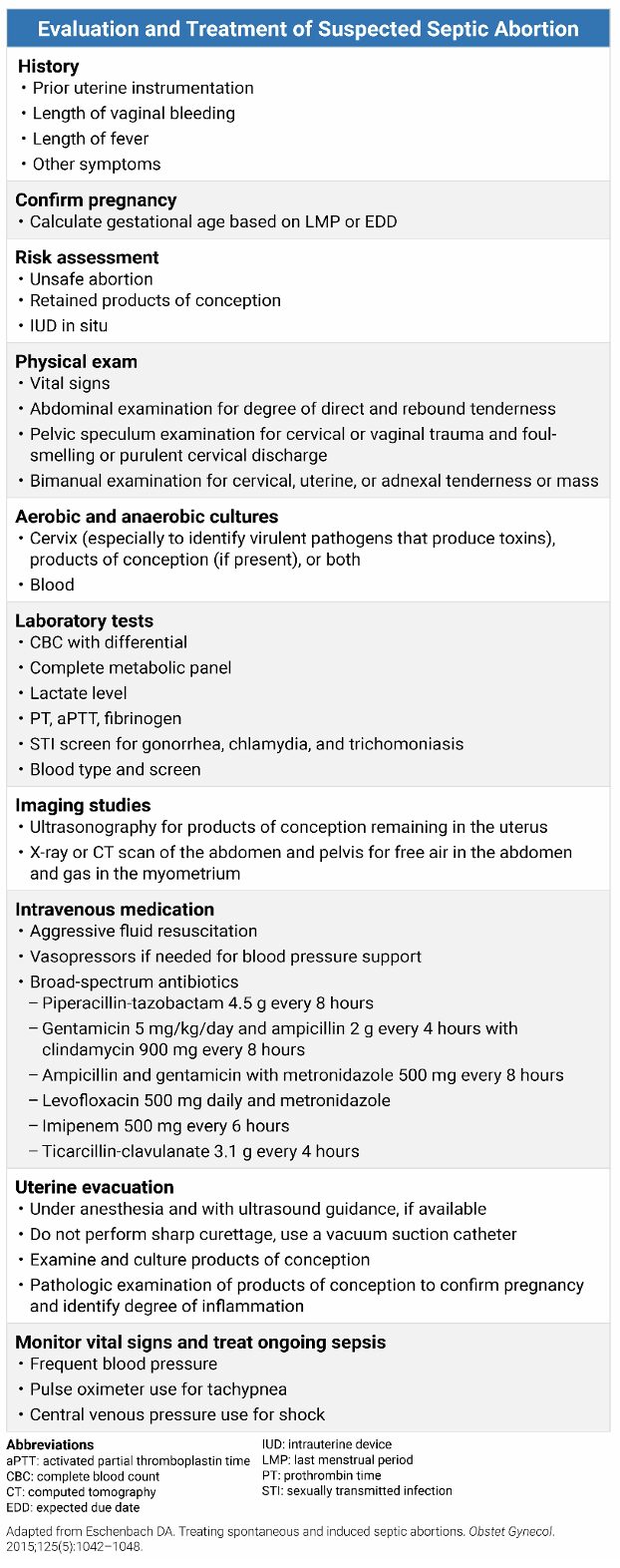
Evaluation:
- Presentation: ABCs.
- Airway/breathing: increased likelihood of acute respiratory distress syndrome (ARDS) secondary to septic abortion.4,5
- Circulation: patient may require cardiovascular support (intravenous [IV] fluids, vasopressors, blood transfusion).
- Increased likelihood of disseminated intravascular coagulation (DIC)/hemolysis.1
- Important to inquire about recent gynecologic procedures or pregnancies.
- Patients may be unwilling to provide this information due to concern for legal repercussions.
- Physical exam, including speculum and/or bimanual exams, to assess for:4
- Significant pain with manipulation of uterus/cervix,
- Vaginal lacerations/tears from instrumentation,
- Bleeding or passage of products of conception,
- Purulent discharge from the cervix,
- Products of conception in the vagina.
- β-hcg to confirm pregnancy, Rh studies, cervical culture (including anaerobic and aerobic cultures), also consider wet prep, gonorrhea, and C. trachomatis swabs.1
- After a complete first-trimester abortion (whether spontaneous or iatrogenic), ꞵ-hcg will remain positive for a median of 19-30 days.6,7
- ꞵ-hcg will remain elevated longer in the setting of incomplete abortion, but an elevated ꞵ-hcg is not diagnostic of retained products of conception.8
- Laboratory workup similar to non-obstetric related infection or sepsis:9
- Complete blood count to assess for anemia, leukocytosis.
- Complete metabolic panel and coagulation studies to evaluate for end-organ damage of the kidneys or liver.
- Lactic acid and blood gas (venous blood gas should be adequate).
- Blood cultures X 2.
- Urinalysis and urine culture.
- Chest x-ray to look for pneumonia.
- Consideration of viral testing (i.e., influenza, COVID-19).
- Perform bedside followed by formal ultrasound of the uterus, preferably transvaginal, to evaluate for retained products of conception (POC).1
- Presence of an echogenic mass is the most useful indicator of retained POC.10
- Sensitivity: 92%.
- Specificity: 84%.
- Presence of an echogenic mass is the most useful indicator of retained POC.10
Diagnosis:
- Signs of infection (hypotension, tachycardia, fever, etc.) PLUS:1
- Diagnosis is made clinically, and there should be a low threshold for treatment with empiric antibiotics.1
Treatment:
- Initial management with respiratory support (if needed), IV fluids, antibiotics, and vasopressors.
- Consultation with obstetrician/gynecologist.
- Source control, i.e., surgical removal of infected tissue (usually only includes fetal tissue and placenta) via dilation and curettage (D&C).1
- May require hysterectomy if no improvement in clinical status or if uterine necrosis develops despite D&C, resuscitation, and antibiotics.4
- Generally agreed upon to use broad-spectrum IV antibiotics (e.g., clindamycin 900mg TID + gentamicin 5mg/kg once daily) for 48 hours after the patient starts improving clinically, followed by transition to oral doxycycline (200 mg/day) for a total of 14 days of treatment.4,5
- Penicillin G must be added for clostridial coverage when this organism is suspected (Table 1).4
Table 1. Recommended intravenous antibiotic regimens for septic abortion.1,4,5
| Antibiotic regimen | Dose |
| Clindamycin
Gentamicin |
900 mg TID
5 mg/kg once daily |
| Ampicillin
Gentamicin Metronidazole |
2 g q4 hours
5 mg/kg once daily 500 mg q8 hours |
| Levofloxacin
Metronidazole |
750 mg daily
500 mg q8 hours |
| Imipenem | 500 mg q6 hours |
| Penicillin G* | 4 million units q4h |
| Piperacillin-tazobactam | 4.5 g q6 hours |
| Ticarcillin-clavulanate | 3.1 g q4 hours |
*Added when there is suspicion of clostridial infection.
Prognosis:
- In cases where infected tissue is removed and antibiotics are initiated promptly, patients generally do well.5
- Common complications include: peritonitis, pelvic abscess, and renal failure.11
- Less commonly: septic shock, uterine perforation, bladder injury, DIC/coagulopathy.
- Worst outcomes are associated with toxin-producing bacteria (e.g., Group A Streptococcus [GAS], C. perfringens or sordellii, or specific E. coli strains).1
- Clostridium sordellii is being implicated more often in cases of death secondary to post-abortion infection.12
Pearls:
- Diagnosis is based on signs of infection combined with pregnancy loss and retained products of conception.
- Patients should receive aggressive resuscitation with IV fluids, antibiotics, and vasopressors (as needed) for sepsis.
- Source control via D&C followed by hysterectomy if there is no improvement.

A 26-year-old G2P1 woman at 10 weeks gestation by last menstrual period presents to the ED with severe lower abdominal pain, heavy vaginal bleeding, and fever. She reports she underwent an elective termination of pregnancy at a local clinic 3 days ago. Vital signs include a T of 39.2°C (102.6°F), HR of 118 bpm, and BP of 94/56 mm Hg. Pelvic examination reveals exquisite cervical motion tenderness and malodorous purulent discharge. Which of the following is the most appropriate treatment, in addition to IV antibiotics, for this patient’s most likely diagnosis?
A) Administration of intramuscular methotrexate
B) Dilation and evacuation of the uterus
C) Expectant management with serial beta-hCG monitoring
D) Immediate laparotomy and total abdominal hysterectomy
Answer: B
Septic abortion is a medical emergency defined as any spontaneous or induced abortion complicated by a pelvic infection. This patient presents with the classic triad of fever, abdominal pain, and malodorous vaginal discharge following a recent pregnancy termination. Bedside ultrasound findings might show thickened endometrial echoes and echogenic foci with shadowing, which is highly suggestive of retained products of conception and the presence of gas-forming organisms within the uterine cavity. The primary goal of management in septic abortion is the rapid stabilization of the patient with IV fluids and broad-spectrum antibiotics, followed immediately by the surgical evacuation of the infected uterine contents.
Dilation and evacuation, or sharp curettage, is the definitive treatment for removing the source of infection. Delaying the removal of infected tissue can lead to rapidly progressing pelvic cellulitis, peritonitis, septic shock, and disseminated intravascular coagulation. In this patient, who is already showing signs of systemic inflammatory response syndrome and borderline hypotension, the removal of the nidus of infection is critical. Antibiotics should be started as soon as possible, typically involving a regimen that covers anaerobic and aerobic organisms (e.g., ampicillin, gentamicin, and clindamycin).
While medical stabilization is the first step, the definitive treatment of a confirmed septic abortion is ensuring surgical clearance of the uterus. This procedure should not be delayed by attempts at medical management alone. The clinician must also monitor for complications such as uterine perforation or the development of clostridial toxic shock syndrome, which is associated with a high mortality rate. In the majority of cases, prompt antibiotic therapy combined with dilation and evacuation results in a rapid clinical improvement.
Methotrexate (A) is a folate antagonist used primarily for the medical management of stable ectopic pregnancies or in specific cases of gestational trophoblastic disease. In the case of a septic abortion, the patient has an intrauterine infection associated with retained products of conception, making methotrexate completely inappropriate. Using methotrexate would fail to address the underlying infection or the need for physical removal of the infected tissue. Given this patient’s febrile and tachycardic state, the administration of a chemotherapy agent instead of performing a dilation and evacuation would result in a dangerous delay in care.
Expectant management (C) is a strategy sometimes used for early, uncomplicated spontaneous abortions in which the patient is hemodynamically stable and shows no signs of infection. However, this patient clearly has sepsis and is presenting with a high fever and purulent discharge. Expectant management in the setting of a septic abortion is contraindicated and would likely lead to maternal death from overwhelming sepsis or multisystem organ failure.
While a hysterectomy (D) may be required in severe, refractory cases of septic abortion, such as those involving uterine myonecrosis, clostridial infections, or pelvic abscesses that do not respond to curettage, it is not the standard first-line surgical intervention. A laparotomy is a major surgical procedure that carries its own set of risks and is generally reserved for patients who do not improve after dilation and evacuation or those with evidence of uterine perforation. Starting with a dilation and evacuation is a less invasive and effective way to remove the source of infection while potentially preserving the patient’s fertility.
Further Reading:
Further FOAMed:
- https://www.emdocs.net/emdocs-podcast-episode-57-post-abortion-complications-part-i/
- https://www.emdocs.net/emdocs-podcast-episode-58-post-abortion-complications-part-ii/
- https://www.emra.org/emresident/article/management-and-treatment-of-septic-abortion
References:
- Eschenbach DA. Treating Spontaneous and Induced Septic Abortions. Obstet Gynecol. 2015;125(5):1042-1048. doi:10.1097/AOG.0000000000000795
- Pek Z, Heil E, Wilson E. Getting With the Times: A Review of Peripartum Infections and Proposed Modernized Treatment Regimens. Open Forum Infect Dis. 2022;9(9):ofac460. doi:10.1093/ofid/ofac460
- Aronoff DM, Marrazzo JM. Infections caused by Clostridium perfringens and Paeniclostridium sordellii after unsafe abortion. Lancet Infect Dis. 2023;23(2):e48-e55. doi:10.1016/S1473-3099(22)00590-4
- Harris LH, Grossman D. Complications of Unsafe and Self-Managed Abortion. Campion EW, ed. N Engl J Med. 2020;382(11):1029-1040. doi:10.1056/NEJMra1908412
- Savaris RF, De Moraes GS, Cristovam RA, Braun RD. Are antibiotics necessary after 48 hours of improvement in infected/septic abortions? A randomized controlled trial followed by a cohort study. Am J Obstet Gynecol. 2011;204(4):301.e1-301.e5. doi:10.1016/j.ajog.2010.11.017
- Marrs RP, Kletzky OA, Howard WF, Mishell DR. Disappearance of human chorionic gonadotropin and resumption of ovulation following abortion. Am J Obstet Gynecol. 1979;135(6):731-736. doi:10.1016/0002-9378(79)90383-1
- Steier JA, Bergsjø P, Myking OL. Human chorionic gonadotropin in maternal plasma after induced abortion, spontaneous abortion, and removed ectopic pregnancy. Obstet Gynecol. 1984;64(3):391-394.
- Smorgick N, Segal H, Eisenberg N, Dovev MN, Dvash S, Rabinovich I. Serum β-HCG Level in Women Diagnosed as Having Retained Products Of Conception: A Prospective Cohort Study. J Minim Invasive Gynecol. 2022;29(3):424-428. doi:10.1016/j.jmig.2021.11.006
- Gauer R, Forbes D, Boyer N. Sepsis: Diagnosis and Management. Am Fam Physician. 2020;101(7):409-418.
- Sundararajan S, Roy S, Polanski LT. The accuracy of ultrasound scan in diagnosing retained products of conception: a systematic review and meta-analysis. Am J Obstet Gynecol. 2024;230(5):512-531.e3. doi:10.1016/j.ajog.2023.11.1243
- Sreelakshmi U, Thejaswini J, Bharathi T. The Outcome of Septic Abortion: A Tertiary Care Hospital Experience. J Obstet Gynecol India. 2014;64(4):265-269. doi:10.1007/s13224-014-0509-4
- Dempsey A. Serious Infection Associated With Induced Abortion in the United States. Clin Obstet Gynecol. 2012;55(4):888-892. doi:10.1097/GRF.0b013e31826fd8f8




