Authors: Jessica Nguyen, MD (EM Resident Physician, Virginia Tech Carilion Clinic) and Mary Carroll Lee, MD (EM Attending Physician, Clinical Faculty at Virginia Tech Carilion Clinic) // Editors: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
45-year-old male with a history of hypertension and GERD presents with complaints of chest pain, right shoulder pain, and back pain. Pain is constant, with no exertional symptoms. Also mentions recent cough with a couple episodes of post tussive vomiting for two weeks. Per chart review, he was seen by another EM provider yesterday with a 2 EKG/troponin rule out, then sent home with outpatient follow up. He’s back today because he has continued pain.
Initial vitals: T 37, HR 88, BP 160/80, Sat 98% RA, RR 14
When you arrive in the room, he appears uncomfortable, but non-toxic. His exam is normal including his cardiac, shoulder, neurologic, and abdominal exams. EKG, CXR, CBC, BMP, and troponin are normal. A CTA chest is ordered with concern for aortic dissection. It is negative for dissection and pulmonary embolus, but instead you find a small amount of air just behind his carina.
Where is the air coming from? Who do you consult? Does he need antibiotics? Does he need surgery? What is his disposition?
Background
Pneumomediastinum occurs when air infiltrates the mediastinal structures after a rupture of the esophagus, trachea, or lung.1 Sometimes it occurs spontaneously, with the cause never determined.
-Esophageal: Boerhaave syndrome, Mallory-Weiss tear, complication of endoscopy, blunt or penetrating trauma, foreign body ingestion. Carries a mortality rate of 30-50% from ensuing mediastinitis.2
-Pulmonary: Asthma (most common source in pediatrics), barotrauma, vigorous coughing, vomiting, childbirth, weightlifting, valsalva, rapid ascent while scuba diving, blunt or penetrating trauma, toxic inhalants. Usually self-limiting without intervention and does not carry a mortality risk.3
Pneumomediastinum can present with sore throat, chest pain radiating to back or neck, voice distortion, or shortness of breath.4 You may feel the characteristic crepitus if air infiltrates the subcutaneous tissue resulting in subcutaneous emphysema. It is more common in children, males, and those with pre-existing lung disease.5
A review of published case series revealed that the most common signs and symptoms include chest pain (61%), cough (41%), dyspnea, subcutaneous emphysema (40%), persistent cough (20%), neck pain (17%), dysphagia (14%), and Hamman’s sign, which is a characteristic click at the end of respiration (14%).3
Initial steps: sick or not sick?
If you find or suspect pneumomediastinum, be on the hunt for life-threatening conditions. If the patient is unstable, follow your basic resuscitation guidelines, and be prepared for a thoracostomy. Tension physiology may occur rarely if there is a significant amount of mediastinal air compressing cardiac outflow. If during your exam you feel crepitus along the chest wall or neck, you should quickly perform a bedside US to evaluate for pneumothorax.
Imaging
Radiographically you may see subcutaneous emphysema, pneumopericardium, ring around artery sign (gas around the pulmonary artery and main branches), tubular artery sign (gas outlining the aorta), double bronchial wall, (gas outlining the bronchial wall), or extrapleural sign (gas between the parietal pleura and the diaphragm).6 Lateral soft tissue neck x-ray is the most sensitive x-ray if you have a concern for this. Otherwise CT is the best imaging tool to evaluate for pneumomediastinum, with a sensitivity approaching 100% and specificity of 85%.5

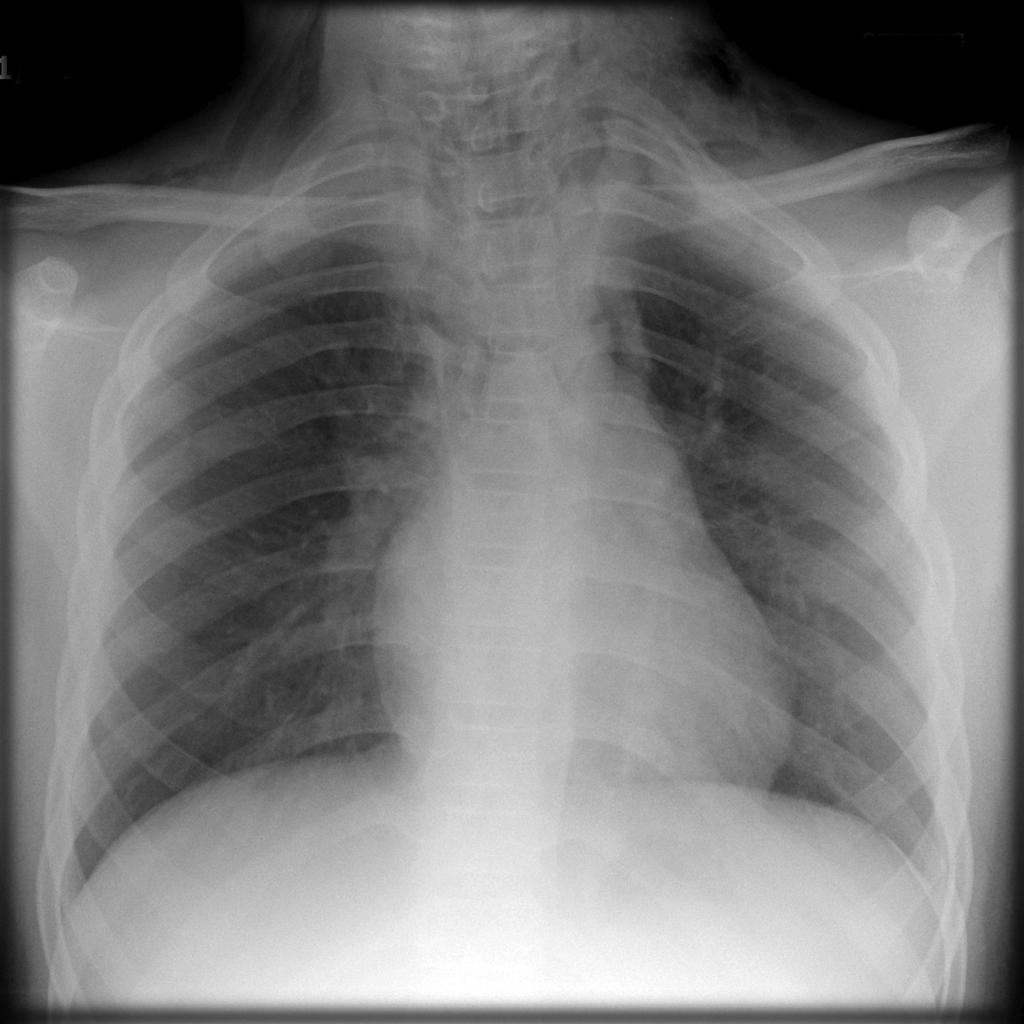
Case courtesy of A.Prof Frank Gaillard, <a href=”https://radiopaedia.org/”>Radiopaedia.org</a>. From the case <a href=”https://radiopaedia.org/cases/8282″>rID: 8282</a>
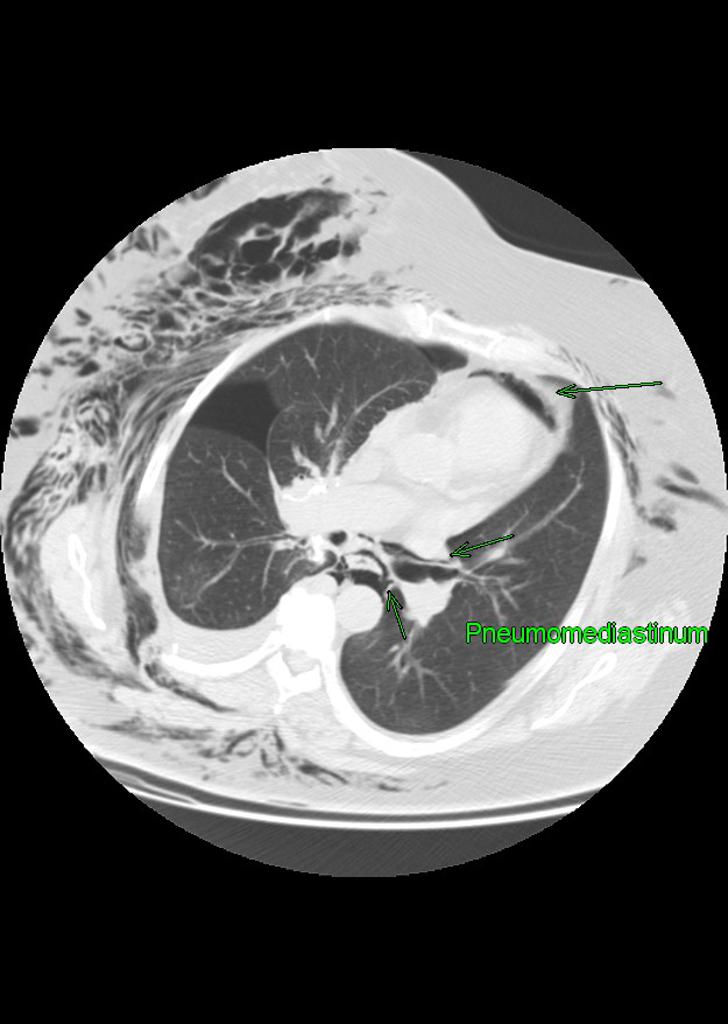
Case courtesy of <a href=”https://radiopaedia.org/”>Radiopaedia.org</a>. From the case <a href=”https://radiopaedia.org/cases/11793″>rID: 11793</a>
How can you determine the source? It’s all about the patient appearance, history, exam, and your studies!
Suspect pulmonary source
Air coming from a ruptured pulmonary tree is a different animal than air coming from the esophagus. A small pulmonary leak is more benign than an esophageal leak.7 If the patient has a history of cough, asthma, or some other respiratory process and is well appearing, then most likely the free air is due to alveolar or bronchial leak. The patient may be observed for 2-4 hours in the ED, and if the patient remains stable, he/she can be safely discharged with good follow-up. The affected tissues will eventually resorb the air. If the patient is unstable, in significant pain or anxiety, or cannot obtain adequate follow-up, admission is recommended. Coughing should be suppressed, and underlying respiratory disease, as well as pain and anxiety, should be treated. Patients do not need prophylactic antibiotics. The choice of who admits may vary by institution and mechanism: consider cardiothoracic surgery, trauma surgery, and medicine.
Suspect esophageal source
Patients with an esophageal source of pneumomediastinum should be regarded as critically ill. If there is concern for esophageal source of pneumomediastinum (history of vomiting, recent endoscopy, etc), the patient should receive antibiotics (piperacillin-tazobactam is first choice for broad coverage including anaerobes) and CT surgery and/or GI should be consulted, followed by admission. Severe sepsis with overwhelming bacterial mediastinitis often develops within 24-48 hours.8 CT scan of the chest with IV contrast should be obtained if not already done.9 An esophagram with water-soluble contrast should also be ordered to evaluate for any ongoing leaks.10 In patients with a high suspicion for leak, or for those who can’t swallow contrast, a flexible endoscopy may be considered.
Key Points
-The source for pneumomediastinum needs to be identified, as the morbidity/mortality, and treatment differ greatly. A careful history and physical exam are important. What risk factors do they have for esophageal versus pulmonary sources? How long have they had symptoms? Are they sick?
-Patients with an esophageal source require admission, broad spectrum antibiotics, resuscitation, and a surgical consult (CT surgery) due to high mortality.
-Patients with a pulmonary source may or may not be sick and may require admission. This depends on their mechanism, level of pain/anxiety, baseline health, and degree of air leak, and ability to follow up. They don’t need antibiotics unless there’s already an infection.11-14
References / Further Reading
- Oshiro Y, Murayama S. Subcarinal Air Cysts. J Comput Assist Tomogr. 2010;34(3):402-405. doi:10.1097/RCT.0b013e3181ccbef8
- Cheng G-S, Varghese TK, Park DR. Pneumomediastinum and Mediastinitis. Murray Nadel’s Textb Respir Med. January 2016:1496-1510.e12. doi:10.1016/B978-1-4557-3383-5.00084-1
- Rezende-Neto JB, Hoffmann J, Al Mahroos M, et al. Occult pneumomediastinum in blunt chest trauma: Clinical significance. Injury. 2010;41(1):40-43. doi:10.1016/j.injury.2009.06.161
- Bejvan SM, Godwin JD. Pneumomediastinum: old signs and new signs. Am J Roentgenol. 1996;166(5):1041-1048. doi:10.2214/ajr.166.5.8615238
- Matsuoka S, Kurihara Y, Yagihashi K, Okamoto K, Niimi H, Nakajima Y. Thin-section CT assessment of spontaneous pneumomediastinum in interstitial lung disease: Correlation with serial changes in lung parenchymal abnormalities. Respir Med. 2006;100(1):11-19. doi:10.1016/j.rmed.2005.04.016
- Weissleder R, Weissleder R. Primer of Diagnostic Imaging. Mosby; 2007.
- Caceres M, Ali SZ, Braud R, Weiman D, Garrett HE. Spontaneous Pneumomediastinum: A Comparative Study and Review of the Literature. Ann Thorac Surg. 2008;86(3):962-966. doi:10.1016/j.athoracsur.2008.04.067
- Dajer-Fadel WL, Argüero-Sánchez R, Ibarra-Pérez C, Navarro-Reynoso FP. Systematic review of spontaneous pneumomediastinum: A survey of 22 years’ data. Asian Cardiovasc Thorac Ann. 2014;22(8):997-1002. doi:10.1177/0218492313504091
- Torigian DA, Lau CT, Miller WT. Mediastinal Diseases. Radiol Secrets Plus. January 2011:469-477. doi:10.1016/B978-0-323-06794-2.00067-5
- Brant WE, Helms CA. Fundamentals of Diagnostic Radiology. Williams & Wilkins; 1999.
- Bakhos CT, Pupovac SS, Ata A, Fantauzzi JP, Fabian T. Spontaneous Pneumomediastinum: An Extensive Workup Is Not Required. J Am Coll Surg. 2014;219(4):713-717. doi:10.1016/j.jamcollsurg.2014.06.001
- Takada K, Matsumoto S, Hiramatsu T, et al. Management of spontaneous pneumomediastinum based on clinical experience of 25 cases. Respir Med. 2008;102(9):1329-1334. doi:10.1016/j.rmed.2008.03.023
- Nwiloh J. Spontaneous pneumomediastinum: Is elaborate workup chasing shadows for a known benign condition? Niger J Cardiovasc Thorac Surg. 2017;2(1):17. doi:10.4103/njct.njct_5_17
- Ebina M, Inoue A, Takaba A, Ariyoshi K. Management of spontaneous pneumomediastinum: Are hospitalization and prophylactic antibiotics needed? Am J Emerg Med. 2017;35(8):1150-1153. doi:10.1016/J.AJEM.2017.03.017








1 thought on “A Case of the Incidentally Discovered Pneumomediastinum”
Thanks. Just saw a patient with N/V and sudden left flank pain radiating to the left shoulder. CT showed pneumomediastinum from the esophagus. Given antibiotics and admitted. Thanks much for the article