First Visit
- HPI
- 61 year old female complaining of one day of dull, crampy, lower abdominal pain with nausea, vomiting and watery, non-bloody diarrhea. Pain is worse in the left lower quadrant. Positive fevers and chills at home. Vomit x 1 today with stomach contents. No recent travel, antibiotic use, or sick contacts. No cardiopulmonary complaints.
PMH/PSH: Asthma, remote hernia repair
Meds: Ibuprofen PRN
All: NKDA
Pertinent Exam
Vitals: 100.1 (temporal) P:110 BP:118/76 RR:16 O2:97% RA
Gen: NAD, lying on stretcher
Abd: Normal bowel sounds, non-distended, mild TTP in LLQ, no involuntary guarding, no rebound.
Cardiopulmonary/GU: WNL
Rectal: Guaiac negative
Labs
WBC: 10.3 (77%neut), Hgb: 15, BMP/LFTs/lipase: WNL, UA: WNL
ED Course
Given Tylenol, IVF, and zofran in ER with moderate improvement of symptoms. Tolerating PO at time of discharge but mild LLQ pain still present. Discharge VS with fever of 101, HR of 105, BP of 122/80.
D/C Diagnosis
Given her good appearance, acute onset diarrhea and vomiting with normal labs, viral syndrome/gastroenteritis was diagnosed and she was discharged with instructions to follow up with her primary physician within the week as needed.
Bounce Back Visit
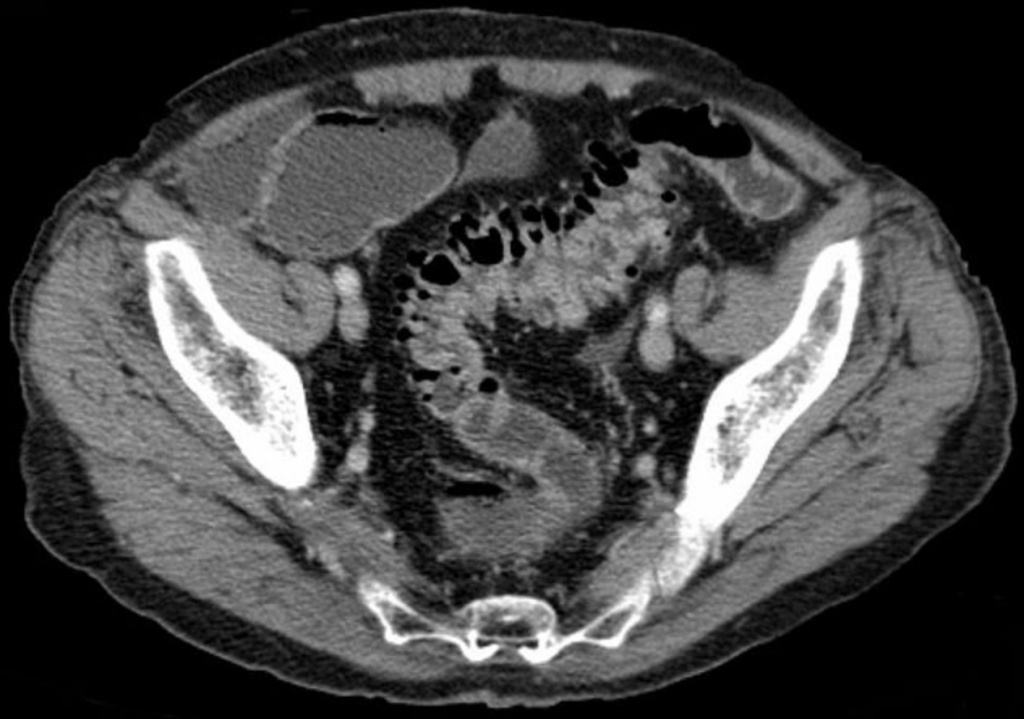
Patient returned 24 hours later due to continued LLQ pain, vomiting, and fevers. Labs again were WNL with no change from the day prior. A CT with PO/IV contrast of the abdomen and pelvis was performed which demonstrated acute descending diverticulitis with micro-perforations, free air, and significant phlegmon without clear abscess formation. Admitted for 7 days on IV Unasyn, diet was advanced, and she was eventually discharged on Augmentin to complete a 14 day course of antibiotics. No surgical intervention needed.
Background Information
- EPIDEMIOLOGY/PATHOPHYSIOLOGY
- Diverticulitis is inflammation within existing diverticula resulting in micro or macroscopic perforation. Around 10-15% of pts with diverticulosis will develop diverticulitis and incidence increases with age with a mean of 63 yrs. About 75% of diverticulitis is classified as simple, with the remaining being complicated diverticulitis (abscess, obstruction, perforation, fistula).
- MEDICOLEGAL
- Abdominal pain remains a leading cause of malpractice litigation in emergency medicine. Common features in cases include lack of distress, no rebound or guarding on examination, a nonspecific discharge diagnosis of gastroenteritis, and lack of timely follow up.
- DIAGNOSIS/PRESENTATION
- No individual sign, symptom, or lab test can reliably diagnose or exclude diverticulitis. Most common symptom is left lower quadrant abdominal pain for 3-4 days preceding ER visit, however this varies widely. Nausea and vomiting are present in around 50% of patients, and constipation is a more common symptom than diarrhea. A normal WBC is found in 45% of patients. GU symptoms such as urgency and frequency are also common due to local irritation of the bladder from surrounding colon inflammation, this can be misleading.
- IMAGING
- CT is best test for diagnosis with a sensitivity of around 94% and specificity of 99%. You’ll see bowel wall thickening > 4mm with inflammation of the pericolonic fat, in addition to the presence of colonic diverticula. Complications are also easily visualized. Abscess, bowel wall thickening, and diverticula can be all visualized on US, however it is less sensitive with significant operator variation.
- TREATMENT
- Although there have been some recent studies challenging the benefits of antibiotics in uncomplicated diverticulitis, the recommended treatment remains antibiotics for gram (-)/anaerobic coverage with Cipro + Flagyl or Augmentin being the preferred outpatient regimens. Total antibiotics course is 10-14 days and bowel rest or a clear liquid diet is also a cornerstone of treatment.
For simple diverticulitis hospitalization is recommended in the elderly, immunosuppressed, patients with significant medical problems, inability to tolerate PO, or those with significant fever and leukocytosis. IV antibiotic regimens include Unasyn, Ceftriaxone + Flagyl, or Zosyn. All complicated diverticulitis requires admission and often surgical intervention/IR drainage.
Follow-up CT 4-6 weeks after completion of treatment is recommended to exclude underlying colonic malignancy.
Errors in Management
- Older patient with localized abdominal pain and fever without definitive diagnosis
- Failure to broaden differential diagnosis and to address more serious diagnoses
- Abnormal vital signs at discharge without improvement after treatment
- Vague discharge instructions without clear/appropriate follow-up (12 hours!)
Take Away Points
- Identify high risk patients while in the ER; those who are older, homeless, with a psychiatric illness, or those with a high risk complaint such as chest or abdominal pain without definitive diagnosis. In general, ask yourself “is this a patient I’ll be worrying about after I’ve left the ED?”
- In high risk patients you’re discharging, make sure to review labs, all chart notes (including nursing notes!), and to consider serious diagnoses you may be missing.
- Older patients with abdominal pain often present with atypical exam findings and normal labs (see references 2 and 3 below).
- Gastroenteritis is a term found on the charts of more malpractice cases than any other diagnosis in EM. Weinstock describes gastroenteritis bluntly as “the refuge of the intellectually destitute”. If the diagnosis is not known, then vomiting, diarrhea or abdominal pain of unknown etiology are all acceptable to use as impressions.
- If a CT scan is not done, the patient should understand that their current clinical presentation is “lower risk” (not “no risk”), and if symptoms change/persist/worsen, they need to return for re-evaluation.
- All patients who are being discharged with non-specific abdominal pain should be told to follow-up for re-evaluation within 8-12 hours.
References
- Cosby, Karen S. A Framework for classifying factors that contribute to error in the Emergency Department. Annals of Emergency Medicine. Dec 2003 42:6 pg 815.
- Bugliosi TF, Meloy TD, Vukov LF. Acute abdominal pain in the elderly. Annals of Emergency Medicine. 1990; 19(12):1383.
- Parker LJ, Vukov LF, Wollan PC. Emergency department evaluation of geriatric patients with acute cholecystitis. Academic Emergency Medicine. 1997;4(1):51.
- Weizman A, Nguyen G. Diverticular disease: Epidemiology and management. Canadian Journal of Gastroenterology. 2011 July;25(7):385-389.
- Weinstock M, Longstreth R. Bouncebacks! Emergency Department Cases: ED Returns. Anadem Publishing 2005




