
Author: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) // Editor: Alex Koyfman, MD (@EMHighAK)
Your next patient is a 42-year-old male who presents with fever, headache, and rash. He says this began several days ago, and his appetite has also been poor. His VS include T 101.8 F, HR 122, BP 91/45, RR 21, and room air O2 saturation 98%. You see a diffuse maculopapular rash with dry oral mucous membranes, but the rest of the exam is normal. Fever, rash, hypotension, tachycardia…. doesn’t sound good. As you consider your next steps, the patient asks, “Could it be my new therapy for lymphoma?” You reconsider the all-important history. The patient hands you a sheet of paper that says “Chimeric Antigen Receptor (CAR) T-Cell Therapy”. What is this therapy, and what else should you consider?
What is this therapy?
CAR T-Cell therapy refers to a relatively newer immunotherapy for several specific types of malignancy. This therapy is now becoming more common, which means emergency physicians may evaluate these patients in greater number. This post will provide a brief background on the therapy and a closer look at potential complications.
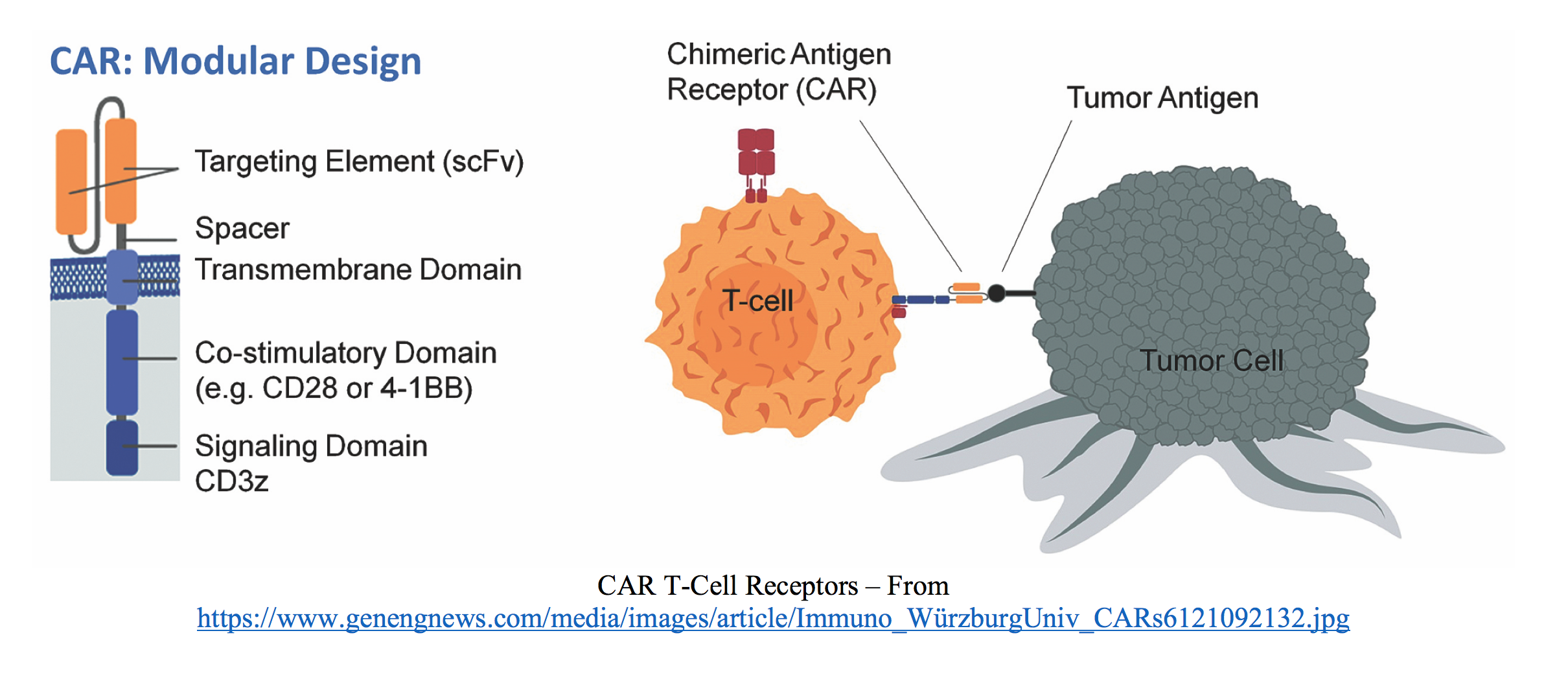
CAR T-Cell therapy uses the patient’s own immune cells (specifically T cells) to find and kill cancerous cells after some genetic modification of the patient’s immune system. The specific component of the T cell modified is the chimeric antigen receptor, which allows the T cell to recognize and destroy cancerous cells. Upon reinfusion after laboratory modification, these T cells can continue to multiply. They may last for longer time periods as well.1-6
What does it entail?
The first step is the removal of T cells from the patient’s blood via leukapheresis. These T cells are taken to a lab and modified (often with a disarmed virus) so they produce chimeric antigen receptors. These cells are then multiplied in the lab over approximately a two week period. During the laboratory step, the patient undergoes a chemotherapy regimen. Once enough numbers are obtained, the cells are then infused into the patient.1-4 As discussed, these receptors target and attach to a specific antigen on malignant cells.

What is it used for?
Genetically equipping lymphocytes with chimeric antigen receptors has been used since the late 1990’s. In 2017, two CAR T-Cell therapies were approved by the FDA for pediatric acute lymphoblastic leukemia (mostly B cell lymphomas) and adult advanced lymphoma that are resistant to standard therapies.1-6 However, this treatment strategy is evolving for use in other malignancies such as solid tumors (over 50 clinical trials are underway).1-3 For now, researchers are focusing primarily on hematologic malignancies.
What are some potential problems?
There are a significant number of side effects. Patients typically demonstrate B cell aplasia from the therapy, but they may also develop other blood line abnormalities such as anemia or thrombocytopenia.1-3
Autoimmune toxicity, cytokine release syndrome (CRS), and neurologic issues are potentially major side effects. Autoimmune toxicity is due to antigen-specific attack on host tissues by the modified T cells if the targeted antigen is present on nonmalignant cells. This is not as common with newer CAR T-cell therapies.1-3,7
CRS, or cytokine storm, is due to massive release of cytokines and other immunologic actors that destroy tumor cells. This condition may occur in a variety of noninfectious and infectious diseases, often due to a medical intervention. Cytokines are small proteins secreted by cells for cellular signaling and communication with a variety of effects. These cytokines result in systemic inflammation, causing high fevers, rash, fatigue, dyspnea, loss of appetite, headache, seizures, tachycardia, and hypotension (with wide pulse pressure). Patients with extensive cancers can demonstrate severe disease. CRS typically occurs 1-5 days after infusion of CAR T-cells; however, it may occur weeks later. Most cases are mild.1-3,7

Classification of CRS includes:
Grade 1 – Mild reaction with fever => provide symptomatic therapy, assess for infection, may continue infusion.
Grade 2 – Moderate reaction with hypotension that responds to fluids or one vasopressor or hypoxia that responds to < 40% O2 => infusion should be interrupted; symptomatic treatment (acetaminophen, NSAIDs, IV fluids) should alleviate symptoms, but assess for infection.
Grade 3 – Hypotension requiring multiple pressors, hypoxia requiring > 40% O2, or symptoms recur after sudden improvement => hospitalization needed for therapy, stop infusion, treat for infection, consider tocilizumab +/- steroids.
Grade 4 – Severe, life-threatening sequelae (ARDS, depressed cardiac function, DIC, renal/hepatic failure) => Treatment same as Grade 3.
Grade 5 – Death
Lab testing often includes elevated liver function tests, increased bilirubin, elevated or low WBC, elevated or low platelets, low fibrinogen, elevated BUN, and elevated D dimer. Biomarkers such as cytokine levels, CRP, and ESR can be used to assist with diagnosis, but they should not be relied on in the ED. Management is based on the grade of CRS. Severe cases require discontinuing the infusion and providing supporting therapies. Other therapies include tocilizumab, a monoclonal antibody against IL-6, with or without steroids. Most importantly, differentiating this reaction from infection/septic shock is difficult in the ED, and patients should receive antibiotics and resuscitation.1-3,7
Neurologic complications are also a component of CRS and may present with a wide variety of symptoms ranging from mild headache to severe confusion, delirium, and seizures. This can be due to neurotoxicity or cerebral edema from the therapy.1-3,7 If presenting acutely, evaluation should be based on severity of the symptoms and neurologic status. Patients with the severe symptoms should likely be evaluated with imaging and laboratory assessment to rule out other life-threatening conditions (stroke, bleed, tox, infection, etc.). If concerned for severe cerebral edema, consider your standard ICP-lowering therapies.
Complication Bottom Line: Patients with complications from CAR T-cell therapy can present with a wide variety of symptoms. Life-threatening conditions should be considered first before assuming the patient’s presentation is due to the therapy. Consultation with hematology/oncology, resuscitation with fluids/pressors, and broad-spectrum antibiotics are recommended. Severe neurologic symptoms require imaging, and treatment to lower ICP may be needed.
Back to our case…
You order 2 L LR and several assessments including CBC, renal function, liver function, coagulation panel, lactate, TSH, ECG, urinalysis, and CXR. His lactate is 3.3, and his WBC returns at 2.2 and platelets at 62,000. His CXR and UA are normal, but with the story and patient appearance, you order cefepime and vancomycin and consult hematology/oncology. They agree with your treatments and ask you to add a CRP and ESR to your orders, and they will admit the patient.
Key Takeaways
– CAR T-cell therapy is a relatively newer cancer therapy which utilizes the patient’s own immune system to fight malignancy.
– The therapy is completed through several stages: 1) obtain patient T cells, 2) genetically modify T cells, 3) expand in laboratory, 4) infuse into the patient.
– This therapy is predominantly used for lymphoma, but new targets are being tested.
– Complications include cytokine storm, neurologic issues, and autoimmune toxicity. Patients presenting with complication require consultation and resuscitation, while assuming the “worst first”.
Resources / Further Reading
- Pagel JM, West H. Chimeric Antigen Receptor (CAR) T-Cell Therapy. JAMA Oncol.2017;3(11):1595.
- National Cancer Institute. CAR T Cells: Engineering Patients’ Immune Cells to Treat Their Cancers. Available at https://www.cancer.gov/about-cancer/treatment/research/car-t-cells
- Jackson, H. J. et al. Driving CAR T-cells forward. Nature Reviews Clinical Oncology 13, 370–383 (2016).
- Brentjens, R. J.et al. CD19-targeted T cells rapidly induce molecular remissions in adults with chemotherapy-refractory acute lymphoblastic leukemia. Transl. Med. 5, 177ra138 (2013).
- Lee, D. W.et al. T cells expressing CD19 chimeric antigen receptors for acute lymphoblastic leukaemia in children and young adults: a phase 1 dose-escalation trial. Lancet 385, 517–528 (2015).
- Maude, S. L.et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. Engl. J. Med. 371, 1507–1517 (2014).
- Lee, Daniel W. et al”Current concepts in the diagnosis and management of cytokine release syndrome.” Blood 2:188-195 (2014).




