Authors: Brit Long, MD (@long_brit, EM Physician at SAUSHEC, USAF) and Barry Sheridan, DO (EM Staff Physician and Professor at SAUSHEC) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) & Justin Bright, MD (@JBright2021, Senior Staff Physician, Henry Ford Hospital)
The first patient of your shift is a 24 year-old male involved in an MVA. He is brought in by EMS on a backboard and C-collar and is screaming “Get this collar off me; I can’t breathe!” He is hemodynamically stable with a GCS of 15, no distracting injuries, and no signs of ETOH or other toxidrome. He has some paravertebral neck pain but no midline tenderness. The nurses ask if they can remove the C-collar. You try to recall the NEXUS criteria, but also remember there is the Canadian C-Spine Rule as well. You begin to wonder which to use, which fits this particular scenario, and once you choose, is it sensitive and specific enough to ensure your patient’s safety?
How often have you been in similar situations and begin to wade your way through multiple clinical decision rules that were made to help make clinical decisions easier, but in fact, may add indecision and confusion to the situation?
This series of articles will attempt to demystify the selection and use of clinical decision rules in Emergency Medicine.
Decision rules for many conditions can be hard to search for considering their nomenclature is not standardized e.g., Ottawa Ankle Rule, Canadian C-Spine Rule, Nexus. Our recent search for an idea of the number of Clinical Decision Rules that exist led to a Pub Med report of over two thousand possibilities. Also there is a difference between Clinical Decision Rules and Clinical Scores. Clinical scores, in particular risk stratification scores or scales, take into account complex conditions such as COPD or CHF, seeking to estimate the risk of bad outcome. This can assist a provider in determining appropriate disposition, such as the PORT score for pneumonia or Ottawa Heart Failure Risk Scale. Each answers a question in a different way and needs to be used in the appropriate situation to answer the question at hand.
Background
Emergency physicians make countless decisions during each shift. Medicine is an art, one that often requires quick decisions based on limited data. We take a thorough history, perform a pertinent physical exam, and order labs and imaging to help us form a clinical impression. Each new piece of data helps us through this process, making some diagnoses more likely and others less likely.
Clinical decision rules (CDRs) are everywhere in medicine today. They were developed to improve our decision-making capability. We are constantly under stress to improve throughput and diagnostic capabilities. CDRs are appealing in that they strive to take murky, unclear variables and change them into a structured tool or assessment. They can potentially take more factors into account than the typical physician at the bedside and give consistent results if applied appropriately.
However, these rules are not always “user friendly.” They may take into account too many variables, not answer an appropriate clinical question, or not improve our clinical gestalt. Multiple CDR’s may exist for one clinical entity, forcing us to decide which we will follow e.g. NEXUS C Spine Rules and The Canadian C-Spine Rule.
Clinical Decision Rules: Part 1 – What makes a CDR useful?
There are many nuances when using CDRs in emergency medicine. This is the first of a three-part series in the pearls and pitfalls of CDR’s. This first post will evaluate what makes a CDR useful.
In the ideal world, a clinical model combines high sensitivity and specificity. It would correctly identify with reliability those patients with high likelihood for a specific outcome, while at the same time excluding those who will not. Unfortunately, this is often not possible, as sensitivity and specificity are usually mutually exclusive: as one rises the other tends to fall.
How are CDRs created?
There are four predominant stages of CDR creation. 1) A derivation study seeks to create/derive the rule. 2) A validation study prospectively assesses the rule’s accuracy, reliability, and impact. 3) An implementation study then assesses the rule’s impact on patient care. 4) And finally, an evaluation of the adoption of the rule and barriers occurs.
What makes a CDR good?
When considering use of a CDR, look at the following:
- Does it address a relevant question? Some CDRs look at irrelevant, uncommon, or trivial clinical situations. These CDRs likely will not help you.
- Does it address a common condition? You don’t need a decision rule for arterial air embolism or pituitary apoplexy. On the other hand, a child who falls and hits his head is a very common chief complaint.
- Has it been derived? This requires the provider to evaluate the rule methodology. Or you can take the easy way and use FOAM such as The Skeptics Guide to Emergency Medicine or other EBM resource to evaluate the rule. If it’s not rigorously derived, it is likely weak and will not help.
- Has it been externally validated? This is an important step, as rules usually perform well in the initial derivation population. This is where the rubber meets the road. Does the rule work in a different population? If it continues to work well when retested, move on to the next step.
- Does it improve on existing clinical practice? The goal of a CDR is to improve patient care, not just predict something we are already doing. If it doesn’t improve clinical gestalt, it isn’t helpful.
- Is it applicable to your practice and patient? This is really important, as not all CDRs apply to your practice setting, population, or style. If your setting does not match the derivation or validation populations, then be wary of confidently using a CDR.
- Is it easy to remember and use? EM providers have way too much to remember as it is, and we have to keep up with an ever-evolving field. CDRs must be easy to use or easy to find and calculate. If not, then it is likely more trouble than it’s worth.
Example
Let’s look at the Ottawa Ankle Rules. Ankle and foot injuries are very common in the ED. The premise of the rules is to help providers determine who needs radiographs while not missing significant fractures.
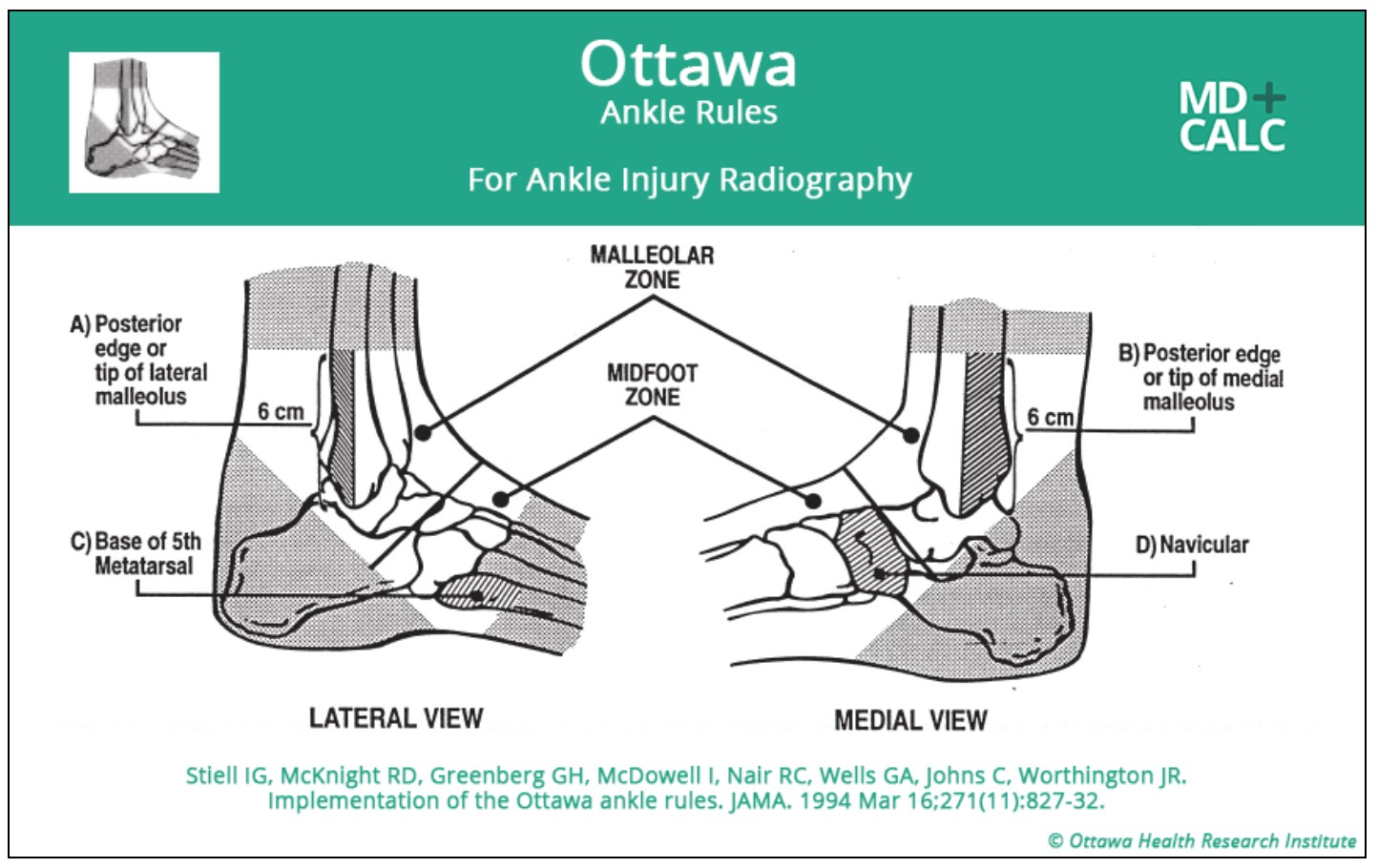
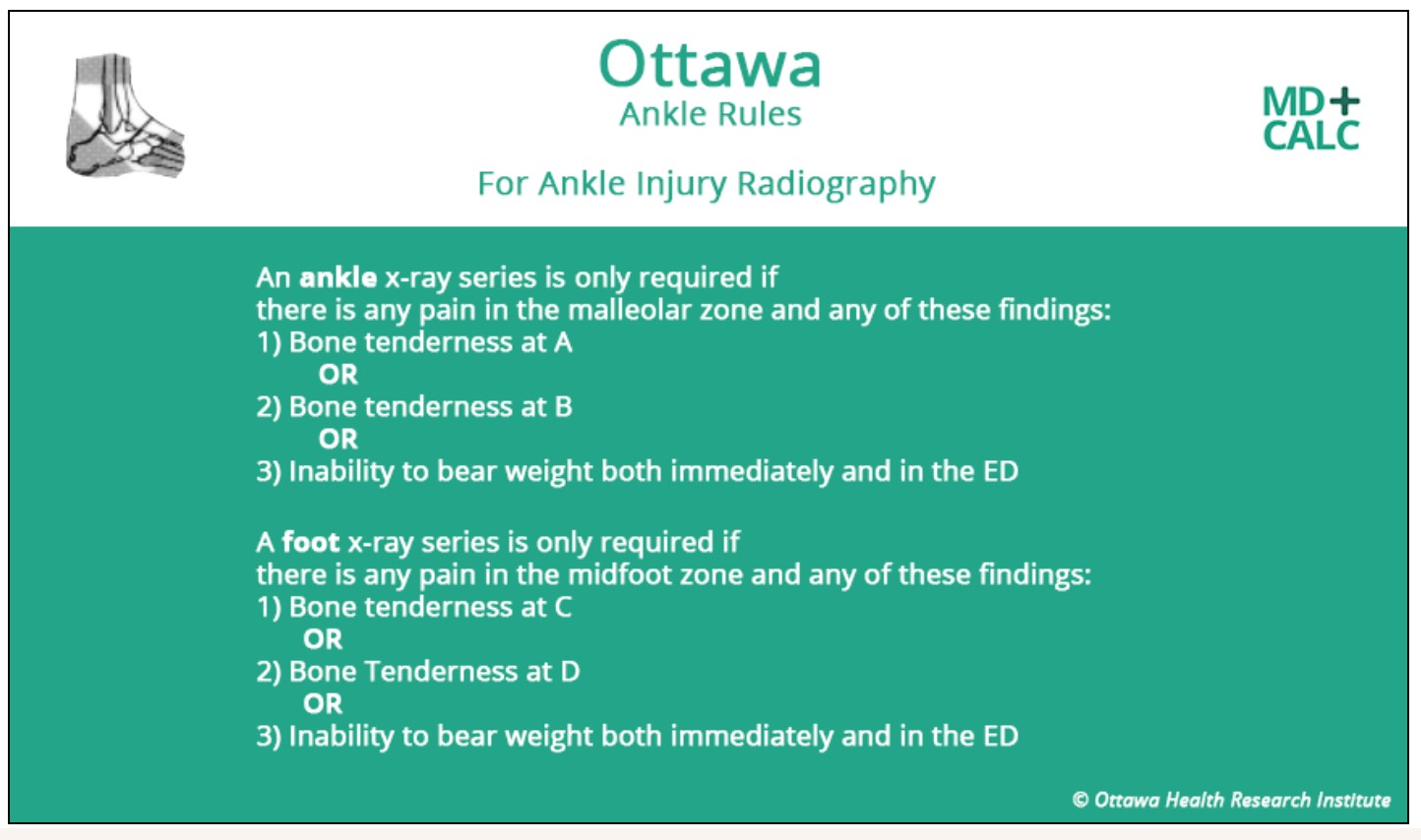
The rules are very sensitive, but specificity for fracture does suffer. This is an important aspect of CDRs which will be explored in the series. The rules do address a relevant question, as these injuries are common and we are always trying to not miss injuries while speeding disposition. The rules have undergone multiple derivation studies and have been externally validated. The rules do improve on clinical practice, as reduction in radiographs by 25-30% has been observed in multiple trials. Applicability to your practice and the patient in front of you does have several caveats: care should be taken with unreliable examinations in patients who are intoxicated, uncooperative, have distracting injuries, diminished sensation in legs (i.e. neuropathies), and have gross swelling preventing palpation. Finally, it is easy to remember and use, and multiple resources have the tool listed (such as MDCalc, WikEM, PalmEM, etc.).
Summary
Clinical decision rules are used to improve decision-making capabilities of providers. This first part of CDR series evaluates how CDRs are created and what makes a CDR useful. Stay tuned for future posts detailing other aspects of CDRs.
References/Further Reading:
- Ingul BJ, Rogers MAM. Searching for clinical prediction rules in MEDLINE. Journal of the American Medical Informatics Association 2001;8(4):391-97.
- Stiell IG, Bennett C. Implementation of clinical decision rules in the emergency department. Acad Emerg Med 2007;14:955-59.
- Stiell IG. Clinical decision rules in the emergency department. CMAJ 2000;163(11):1465-66.
- Green SM. When do clinical decision rules improve patient care? Ann Emerg Med 2013;62:132-35.
- Adams ST, Leveson SH. Clinical prediction rules. BMJ 2012;344:d8312 doi: 10.1136/bmj.d8312.
- Helman A. Episode 56 The Stiell Sessions: Clinical Decision Rules and Risk Scales. Emergency Medicine Cases. http://emergencymedicinecases.com/episode-56-stiell-sessions-clinical-decision-rules-risk-scales/.
- Stiell IG, et al. Implementation of the Ottawa ankle rules. JAMA 1994;271(11):827-832.
- Anis AH, et al. Cost-effectiveness analysis of the Ottawa Ankle Rules. Ann Emerg Med 1995;26(4):422-428.
- Bachmann LM, et al. Accuracy of Ottawa ankle rules to exclude fractures of the ankle and mid-foot: systematic review. BMJ 2003;326.7386:417.




