Originally published at CoreEM.net, dedicated to bringing Emergency Providers all things core content Emergency Medicine available to anyone, anywhere, anytime. Reposted with permission.
Follow Dr. Swaminathan and CORE EM on twitter at @EMSwami and @Core_EM
Hypokalemia
Background
Definition: A serum potassium level < 3.5 mEq/L. Severe hypokalemia < 2.5 mEq/L
Epidemiology
- Common electrolyte disorder – 20% of hospitalized patients
- 10-40% of patients on thiazide diuretics (Rosen 2014)
Causes
- Renal Losses (diuretics, steroid use, DKA, hyperaldosteronism)
- Increased non-renal losses (vomiting, diarrhea, sweating)
- Decreased intake (malnutrition)
- Intracellular shift (metabolic alkalosis)
- Endocrine (Cushing’s disease, Insulin therapy)
Clinical Manifestations
- Mild hypokalemia often asymptomatic
- Non-specific Symptoms
- Palpitations
- Nausea
- Muscle Weakness
- Myalgias
- Fatigue
- Neurological Effects
- Paresthesias
- Weakness
- Confusion
- Decreased Deep Tendon Reflexes
- Hypokalemic Periodic Paralysis (rare)
Diagnostics
- Serum potassium
- 12-Lead EKG
- Classic Findings
- Flattened T waves
- U waves
- Prolonged QT Interval
- Non-specific ST segment changes
- Note: Hypokalemia is a common predisposing condition for Torsades de Pointes
- Classic Findings
- Urine potassium level (spot): Elevation of urine potassium indicates renal losses as cause of hypokalemia
EKG Gallery

Hypokalemia – U Waves
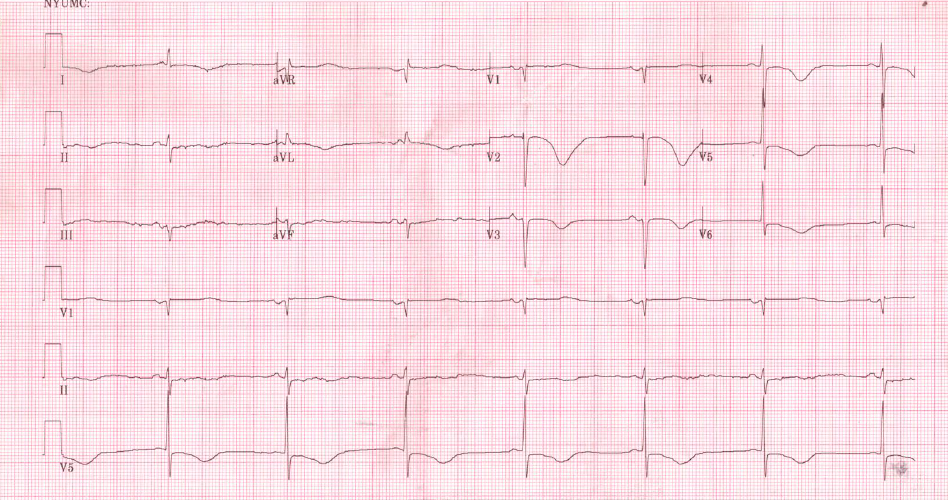
Hypokalemia – QT Prolongation
Life in the Fastlane: Hypokalemia ECG Library
Management
Basics: ABCs, IV, Cardiac Monitor and, 12-lead EKG
Potassium Repletion
- Every drop in serum potassium of 0.3 mEq = 100 mEq total body depletion (Gennari 1998)
- Oral Replacement
- Potassium chloride (KCl) typically used
- Readily absorbed
- Intravenous Replacement
- Rapidly raises serum potassium levels
- Mild to moderate symptoms: 10-20 mEq/hour
- Severe symptoms/critically ill
- Up to 40 mEq/hour
- Consider administration through central line
- Keep patient on cardiac monitor
- Check serum potassium hourly
- Magnesium Co-administration
- Hypokalemia is associated with hypomagnesemia (Boyd 1984)
- Potassium will not move intracellularly (and thus will not replete total body stores) without concomitant magnesium repletion
- Dose: 0.5-1 g/hour
Note: Potassium replacement (particularly IV) is a leading cause of hyperkalemia. Replete cautiously
Take Home Points
- Severe hypokalemia can lead to lethal dysrhythmias typically by prolongation of the QT interval.
- Patients receiving intravenous potassium repletion at more than 20 mEq/hour should have continuous cardiac monitoring and frequent serum potassium evaluations.
- Always replete magnesium when repleting potassium.
Read More
Emergency Medicine Updates – Correction of Critical Hypokalemia
LITFL – Hypokalemia
References
Pfenning CL, Slovis CM: Electrolyte Disorders; in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2014, (Ch) 125: p 1636-1653.
Gennari FJ: Hypokalemia. N Engl J Med 1998; 339:451-458. PMID: 9700180
Boyd JC et al. Relationship of potassium and magnesium concentrations in serum to cardiac arrhythmias. Clin Chem 1984; 30(5): 754-7. PMID: 6713638




