
Authors: Brooke Moungey, MD (Senior EM Resident at the University of Wisconsin) and Christopher Stahmer, MD (Clinical Assistant Professor at the University of Wisconsin) // Edited by: Jennifer Robertson, MD, MSEd and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW Medical Center / Parkland Memorial Hospital)
It is a busy day in the emergency department (ED) when a 35-year old male presents with an insect in his right ear. In the next room, a 3-year old girl presents with her mother after having placed a plastic bead in her left nostril. And just then, a 2-year-old boy is brought in to the ED by his parents because he had just swallowed a coin.
With all the possible tools and techniques for foreign body removal, choosing a method that is most likely to be successful for your patient can sometimes be a daunting task. In addition, it can be challenging when trying to determine if a patient will be cooperative and whether analgesia or sedation will be required.
Here are a few tips to help you remove those foreign bodies like a pro and get your patient safely on his or her way.
Foreign Bodies of the Ear Canal:
While foreign bodies in children often include a wide range of objects such as toys, rocks, beads, crayons, and cotton swabs, foreign bodies in adults are most commonly insects.
There is a wide array of tools available to assist in removal and this can often be confusing for providers as these tools are not created equal for all types or locations of foreign bodies.
- You should always check for tympanic membrane (TM) perforation. If this is present, the patient should not undergo removal in the ED and should be referred to otolaryngology (ENT) for removal.
- In general, you should avoid sharp instruments if you are not getting adequate visualization of the foreign body. Additionally, sharp objects should not be used if the patient is not cooperative with your exam so that accidental TM damage can be avoided.
- Side effects of these removal techniques include tissue damage such as abrasions, lacerations or TM perforations. These techniques can also push the object further back in the ear canal and make removal even more difficult.
- There are several different types of otoscopes. Some include those with removable lenses and operating otoscopes that allow tools to pass through the otoscope head while directly visualizing foreign bodies.
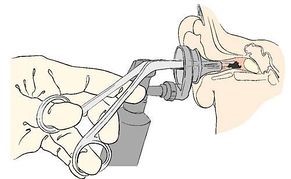
Alligator forceps and curettes:
Curettes are best for foreign bodies that can be well visualized but are small enough that the curette can be pushed beyond the object and pulled from behind. Forceps can also be used to directly grasp objects but are less effective when used for round objects or larger objects. They are more effective for soft or irregularly shaped objects that can be grasped firmly to prevent pushing them further out of reach.


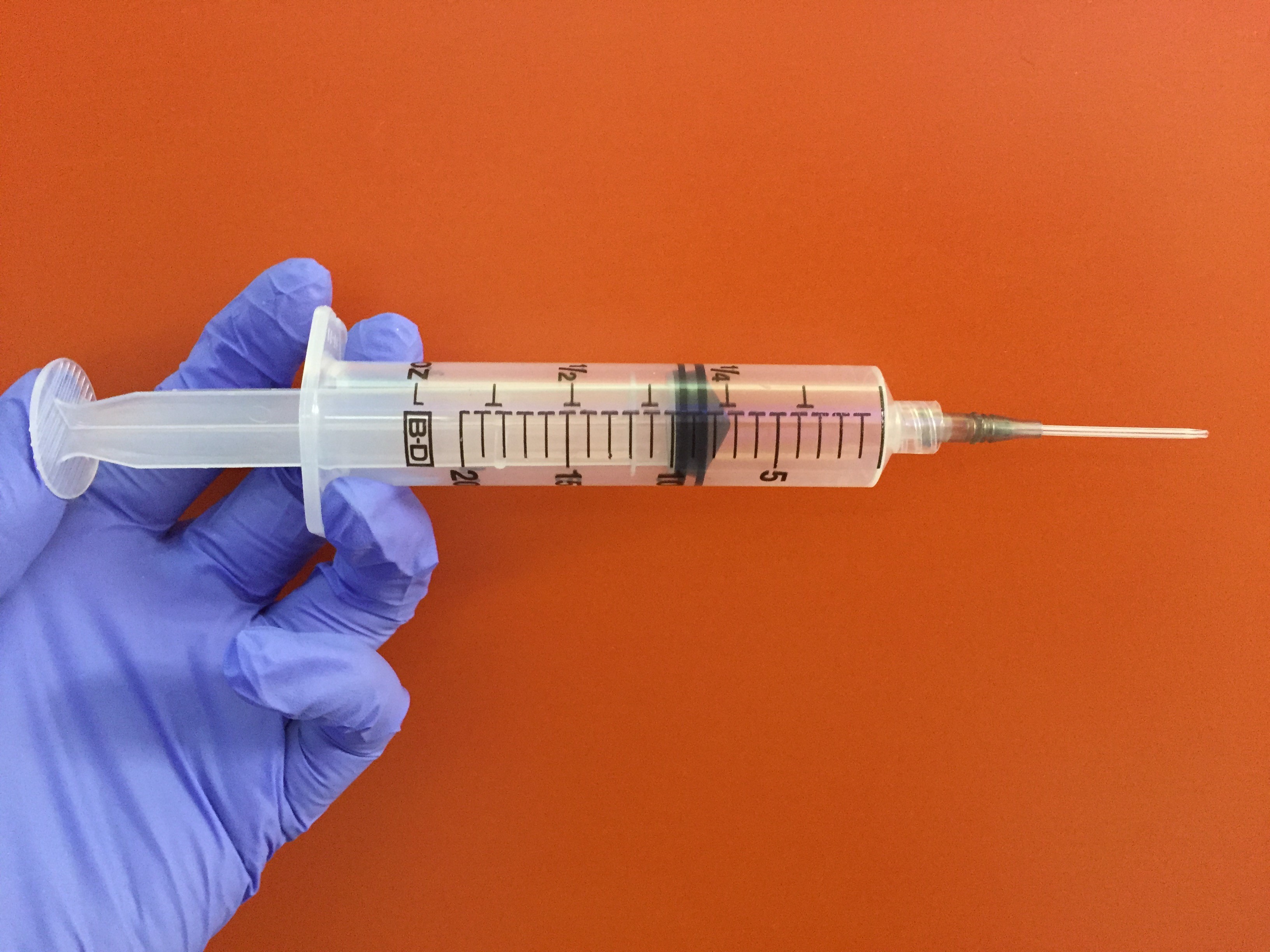
Irrigation:
Can be done using a 20 mL syringe and 16 gauge angiocatheter filled with water or normal saline. A plastic basin may be used to catch the fluid. This technique can be helpful for a variety of foreign body shapes and sizes and is safe for normal TMs. However, irrigation should not be used in patients with a history of TM perforation or instrumentation including myringotomy tubes. This method should not be used for foreign bodies made of organic material as they will soak up the fluid and expand. This will cause further difficulty with extraction. Irrigation should also never be used if the foreign body is a button battery.
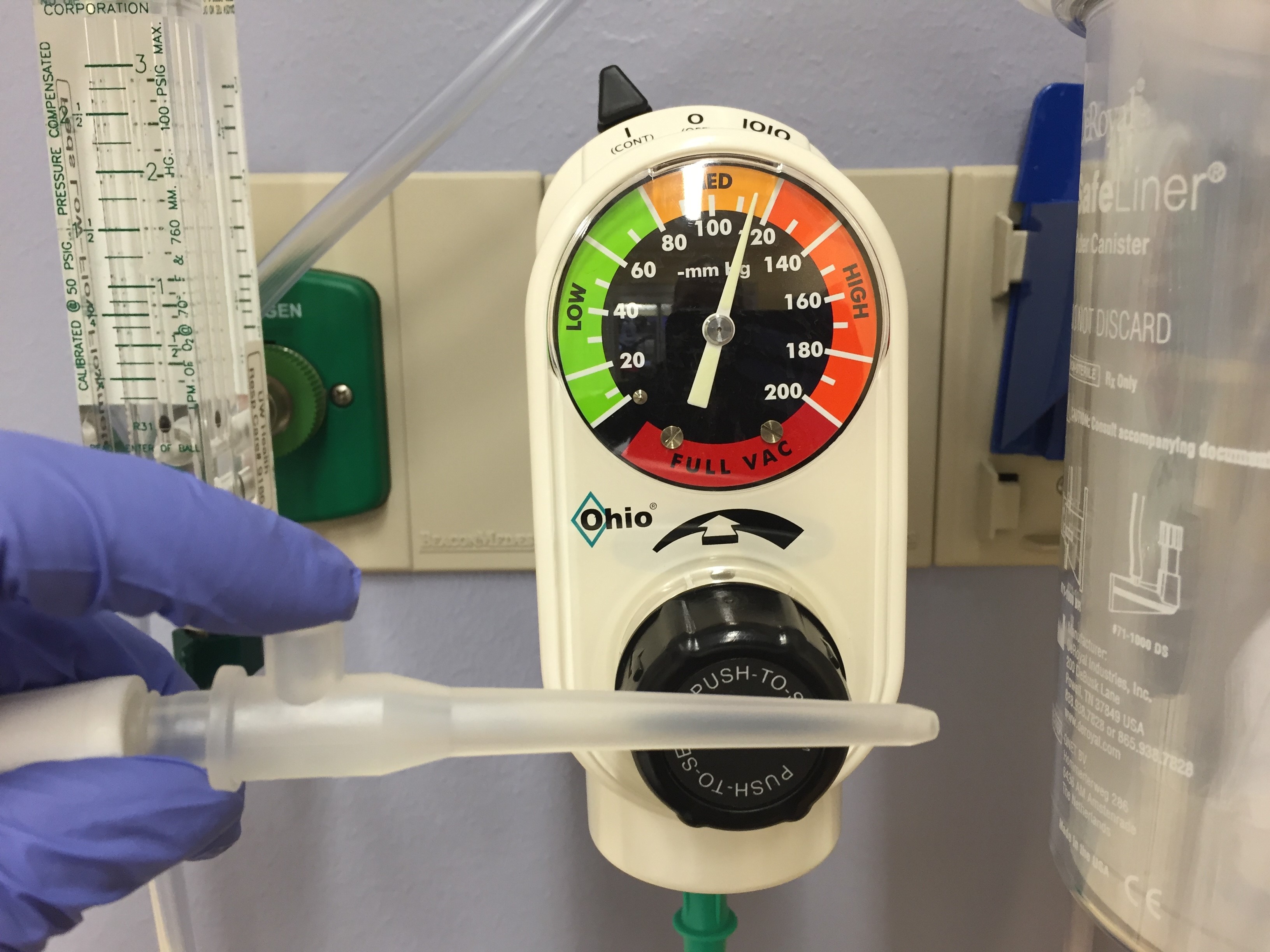
Suction:
Suction tpically requires 100 mmHg or more of negative pressure with a soft-tipped plastic suction catheter placed against the object. The side port can be occluded to capture the object and pull it out. Tip: Best for hard, round foreign bodies.
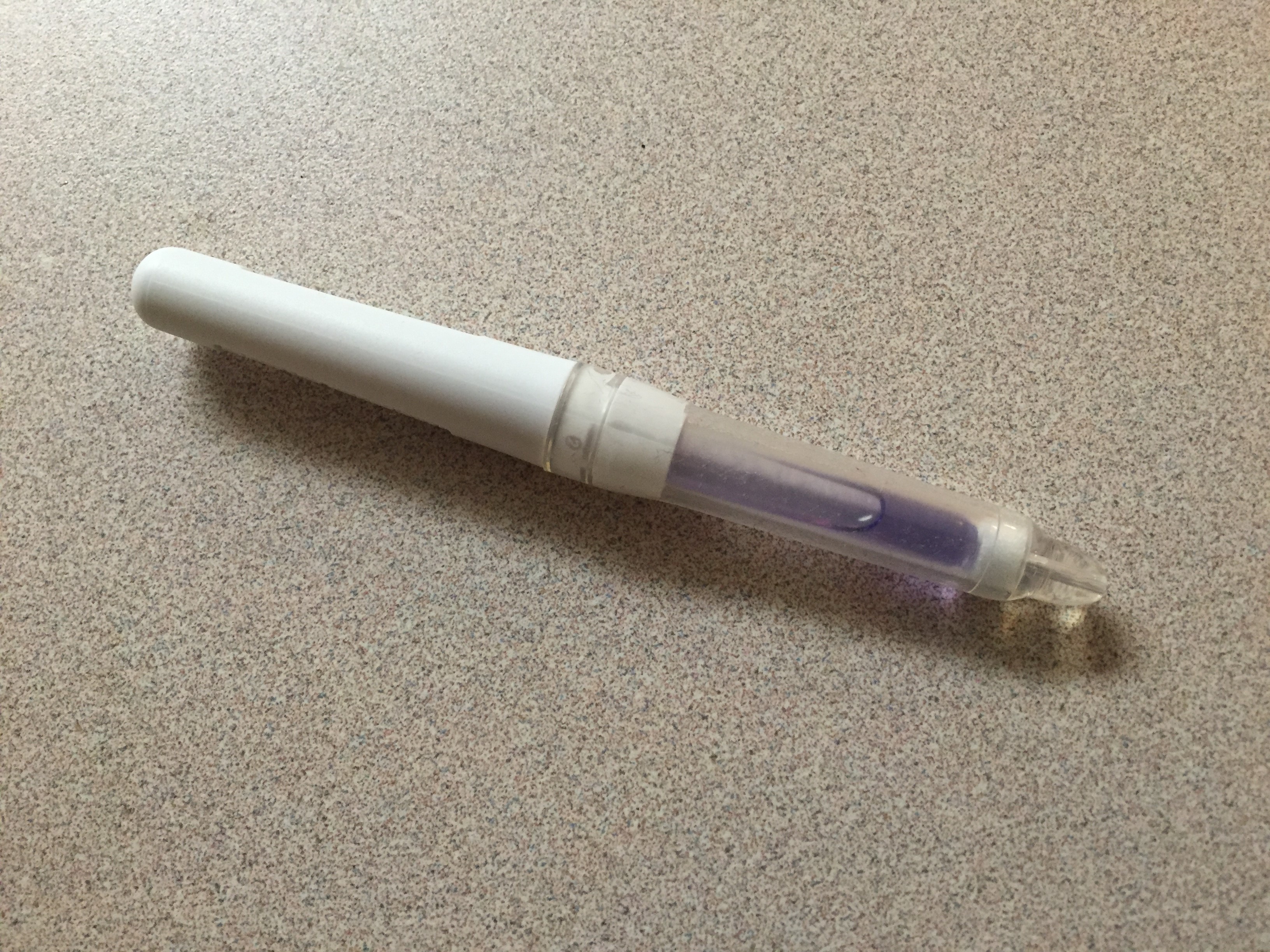
Superglue:
Can be placed on the end of a cotton-tipped applicator that is advanced into the ear canal and pressed against the foreign body until dry. The foreign body can then be pulled out. Be very cautious as glue can be accidentally applied to the ear canal or TM itself and cause tissue damage.
Tip: Best used to extract round objects which are well visualized.
Magnet:
Can be used for removing metal foreign bodies. It works best for smaller metal objects and those in the more distal portion of the ear canal.
Bugs:
Can be manually extracted with forceps or a curette, or irrigated out of the ear canal as previously described. However, live bugs often cause significant patient discomfort with attempted removal. This can be prevented by using a syringe and angiocatheter to fill the ear canal with viscous lidocaine and allowing it to sit for 15 minutes prior to removal. Mineral oil is also an alternative to viscous lidocaine.
Anesthesia/sedation:
A small amount of viscous lidocaine can be a helpful local anesthetic. However, sedation may be needed in younger pediatric patients. Several common options include:
- Intranasal midazolam 0.3-0.5 mg/kg
- Oral midazolam 0.5 mg/kg
- Ketamine IV 1 mg/kg or IM 2-3 mg/kg
Take Away Points:
- Referral to ENT will be necessary if extraction in the ED fails, the foreign body has been in place long enough to cause acute otitis media or other surrounding infection, or if there is a TM perforation.
- Antibiotics will be necessary for abrasions or lacerations of the ear canal, even if extraction is successful. Prescribe ofloxacin 0.3% otic drops 10 drops once daily for 7 days.
- Use different tools and techniques to your advantage to successfully address different types of foreign bodies in the ear canal.
- When one foreign body is found, check for additional foreign bodies in the ears, nose and mouth (especially in pediatric patients).
- Never apply a liquid to a button battery.
Nasal foreign bodies:
Nasal foreign bodies are most commonly found in pediatric patients and often include many of the same objects as foreign bodies in the ear canal. Once the foreign body is located, there are several easy techniques to remove them without additional instrumentation.
- Side effects of these removal techniques include abrasions, lacerations, and epistaxis. Another side effect is potentially moving the object further back, which will increase the risk of aspiration or ingestion.
- A nasal speculum is beneficial to aid in visualizing the object.

Positive pressure:
If the patient can assist with removal, then nose blowing while sitting forward and occluding the other nostril is often effective. If the child is unable to participate in nose-blowing the “big kiss” technique is an alternative. With this technique, have the parent blow into the child’s mouth while occluding the patent nostril. This can also be modified to apply high flow supplemental oxygen or a Bag Mask Valve (BVM) into the mouth while again occluding the patent nostril. Please use caution due to a risk of barotrauma if oxygen or a BVM is used.

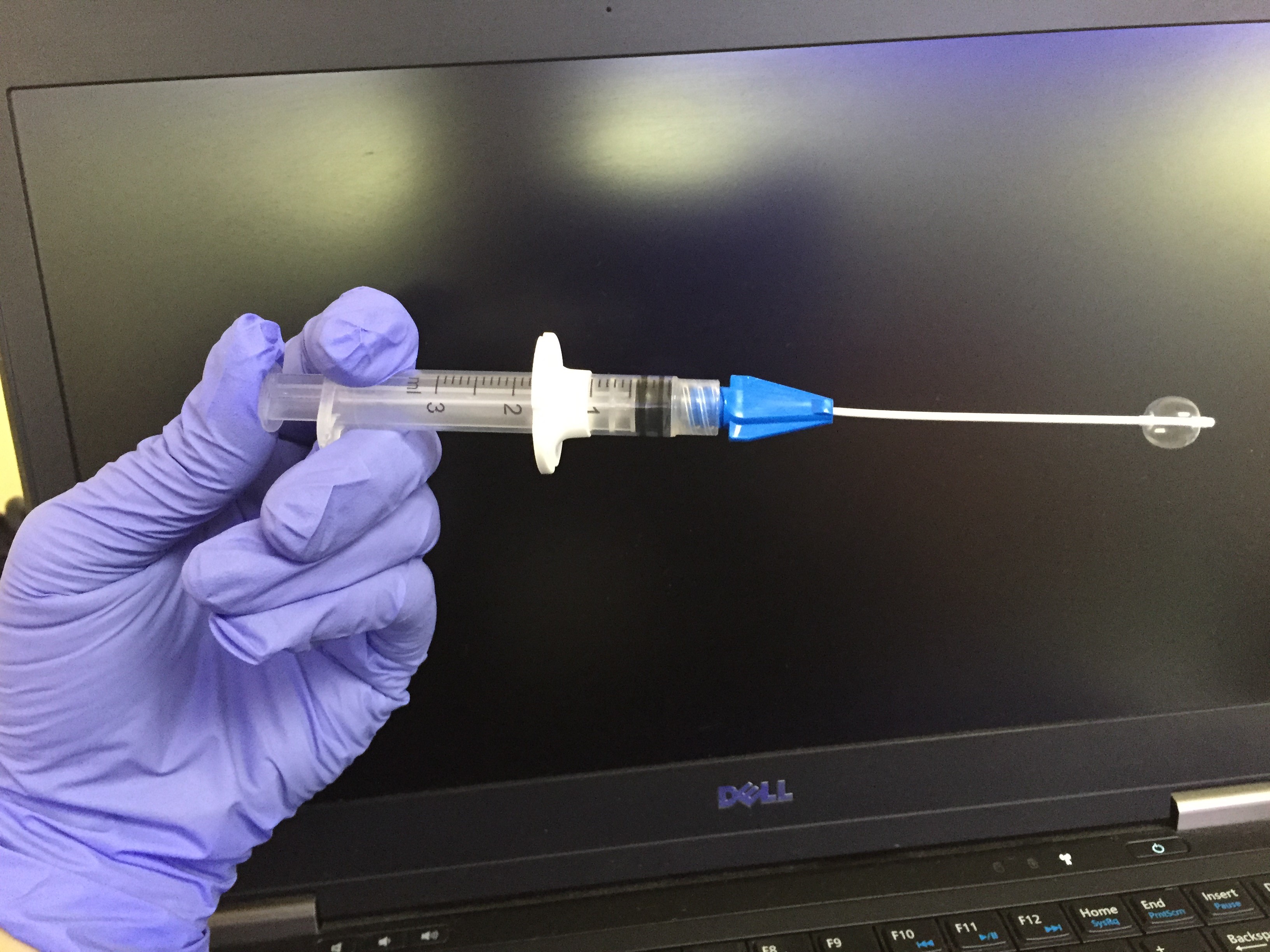
Balloon catheters:
Small balloon catheters such as a Fogarty or Katz extractor can be attached to a 5 mL syringe. Check the balloon function and then advance the deflated catheter tip into the nostril until the entire balloon is past the foreign body. Then inflate the balloon until it fills the space behind the object and pull the balloon catheter out along with the object.
Forceps/Curettes:
Can also be used similarly to foreign bodies of the ear canal. However, they are more effective for nasal foreign bodies if advanced past the object and then used to pull the object forward. If they are used to directly grasp the object, then the object can be pushed further back, which may lead to aspiration, ingestion, or more a difficult extraction.
Anesthesia/Sedation:
Lidocaine or phenylephrine spray can be used to prevent swelling and pain, but should be rarely used due to the risk of causing sneezing and associated aspiration or ingestion of the object. Both of these medications should be avoided in the case of button batteries.
Sedation options are similar to those as listed above for ear foreign bodies; however, no intranasal medications such as intranasal midazolam should be used due to risk of aspirating/ingesting the object.
Take Away Points:
- Referral to ENT will be necessary if ED extraction fails, extraction causes uncontrolled epistaxis or if the foreign body is aspirated.
- When possible, avoid anesthetic sprays and intranasal medications to prevent aspiration or ingestion.
- Non-invasive techniques with positive pressure and the assistance of the child and/or parents are often most successful for nasal foreign bodies.
- Always look for other foreign bodies and never apply liquids to a button battery.
Foreign Bodies of the Throat:
In adults, these foreign bodies often represent food boluses, fish bones, and dentures. In children, they may include a number of objects from coins and button batteries to food, toys, and crayons. If a patient presents with stridor or respiratory distress, it is best to leave him or her in a position of comfort while getting airway equipment ready and gathering resources such as anesthesia and ENT, if available. Airway intervention may become necessary at any time and can include attempting to remove the foreign body with Magill forceps if visible or intubating the patient with an attempt to force the object into the right mainstem bronchus to relieve a complete obstruction.

For patients who are not in respiratory distress, radio-opaque foreign bodies can be located in the esophagus or trachea/bronchus with AP and lateral neck X-rays and an abdominal x-ray can often be used to identify objects in the stomach or further along the GI tract. If the object is radiolucent and suspected to have been aspirated due to respiratory symptoms, then bilateral decubitus X-rays may show air trapping in the affected side such that the lung does not deflate appropriately when the affected side is down. Inspiratory and expiratory films may also show air trapping on the affected side during expiration and pushing of the mediastinum to the opposite side. Any objects located in the respiratory tract will likely have to be removed by bronchoscopy.
Esophageal Foreign Bodies:
Objects that are blunt and small (<2.5 cm wide) may be pushed forward into the stomach as they will likely be small enough to pass the pylorus and pass from the GI tract on their own. This is typically done with application of lidocaine spray to the oropharynx and advancement of a bougie which the patient swallows and is then advanced until the object is dislodged. If this is not an option or this method fails then endoscopy will be needed for removal. Any objects that are sharp, regardless of their location in the GI tract, or too large to pass the pylorus must also be removed by endoscopy. If there are signs the object has caused a perforation, then surgery will likely be indicated for definitive care.
Button batteries:
Regardless of whether the button battery is located in the respiratory tract or GI tract, this is a medical emergency and the battery should be removed by endoscopy or bronchoscopy within 6 hrs of aspiration to prevent necrosis or perforation.
Food bolus:
Administration of glucagon is unlikely to be of benefit as its use in clearing a food bolus is likely related to causing retching and emesis, which can also increase the risk of perforation or tearing of the esophageal mucosa. Food boluses can also be pushed forward into the stomach or removed by endoscopy as listed above for blunt objects in the esophagus.
Take Home Points:
- Most foreign bodies of the throat will be aspirated or ingested and will likely require bronchoscopy, endoscopy or surgery for appropriate treatment. Thus, get your specialty services on board early.
- Button batteries as a foreign body in any location are an emergency and every effort should be made to remove them as quickly as possible, preferably within 6 hrs of ingestion.
- Small blunt foreign bodies (<2.5 cm) and food boluses can be pushed forward into the stomach and passed safely.
- Always evaluate your patient for signs of perforation even after the foreign body has been removed.
References / Further Reading
-Baker MD. Foreign bodies of the ears and nose in childhood. Pediatr Emerg Care 3: 67, 1987.
-Botma M, Bader R, Kubba H. “A parent’s kiss”: evaluating an unusual method for removing nasal foreign bodies in children. J Laryngol Otol 114: 598, 2000.
-Figueiredo RR, Azevedo AA, Kos AO, Tomita S. Complications of ENT foreign bodies: a retrospective study. Rev Bras Otorrinolaringol (English ed) 74: 7, 2008.
-Kadish HA, Corneli HM. Removal of nasal foreign bodies in the pediatric population. Am J Emerg Med 15: 54, 1997.
-Kalan A, Tariq M. Foreign bodies in the nasal cavities: a comprehensive review of the aetiology, diagnostic pointers, and therapeutic measures. Postgrad Med J 76: 484, 2000.
-Marin JR, Trainor JL. Foreign body removal from the external auditory canal in a pediatric emergency department. Pediatr Emerg Care 22: 630, 2006.
-Marx JA, Hockberger RS, Walls RM. Rosen’s Emergency Medicine Concepts and Clinical Practice, 8e. Chapter 60.
-Roberts JR, Custalow CB, Thomsen, TW, Hedges JR. Roberts and Hedges’ Clinical Procedures in Emergency Medicine, 6e. Chapter 63.
-Tintinalli JE, Stapczynski JS, Ma OJ, Kline DM, Cydulka RK, Meckler GD, The American College of Emergency Physicians. Tintinalli’s Emergency Medicine, A Comprehensive Study Guide, 7e. Chapters 80, 119, 143.
-Triadafilopoulos G, Saltzman JR, Travis AC. Ingested Foreign Bodies and Food Impactions in Adults. www.uptodate.com





2 thoughts on “Ear, Nose, and Throat Foreign Bodies”
Pingback: Asynchronous Learning: ENT, OMFS, Ophtho - Bold City Emergency Medicine
Pingback: emDOCs.net – Emergency Medicine EducationEM@3AM: Esophageal Foreign Bodies - emDOCs.net - Emergency Medicine Education