
Author: Lloyd Tannenbaum, MD (EM Attending Physician, APD, Geisinger Wyoming Valley, PA) // Reviewer: Brit Long, MD (@long_brit)
Hello and welcome back to ECG Pointers, a series designed to make you more confident in your ECG interpretations. This week, we feature a post from Dr. Tannenbaum’s ECG Teaching Cases, a free ECG resource. Please check it out. Without further ado, let’s look at some ECGs!
“Hey Mrs. Robinson! Good to see you again. I really appreciate you coming in today to help teach the residents,” you tell one of your favorite patients as the weekly conference is about to begin.
“Of course, doctor. I’m happy to help! Now that I’m retired, I have plenty of time to come in and help you teach,” She responds.
“How do you want to play it this year? Do you want to give the residents a heads up? Or just let them go in blind like last time?”
“Oh, you know me! I love to be a surprise. Let’s see if anyone can figure me out!”
*******
“Ok guys, for conference this week, we’re going to break up into groups of three. One intern, a second year, and a third year. Each group will rotate through 5 different sim stations. One will even have a real patient that you have to work up and diagnose. Have fun everyone. We’ll touch base after you finish all the stations.”
********
“Hello Ma’am! I’m one of the interns in the ED. What’s bringing you in today?” the intern asks Mrs. Robinson.
“Hello young doctor,” she responds. “I’m Tina Robinson, and I’m a 75-year-old lady who feels a little silly coming in to the emergency room, but I passed out this morning and my family doctor told me to come in right away. I really feel fine. I don’t think I need to be here wasting your time.”
“Ma’am, we should really run some tests and check you out to make sure you’re alright. Did you fall or hit your head when you passed out?”
“Well, if you insist, I guess that’s ok. No, I didn’t hit anything. My son was right there and he caught me and lowered me to the ground. Whole episode lasted about 10 seconds, maybe less. And I feel totally fine now.”
“Well, that’s good!” The intern replies. “I’m glad you didn’t hit your head. Let’s get an ECG and see what’s going on with you.”
“That sounds great,” Mrs. Robinson says with a smirk.
“Here is Mrs. Robinson’s ECG.” You tell the residents as you hand it over for the team to review.
“Alright intern, go ahead and take a look. Tell us what you see…” the senior asks.
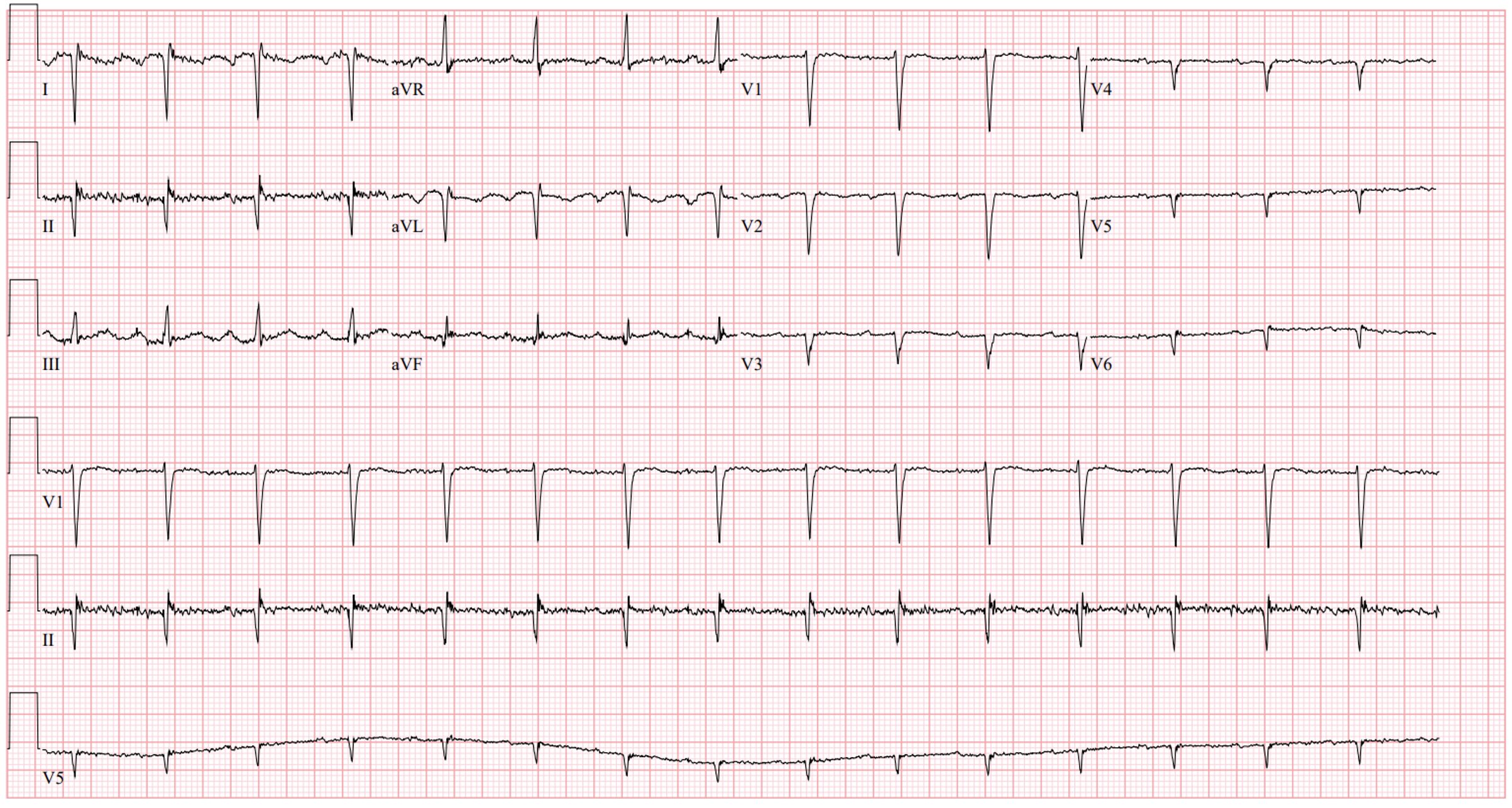
Rate: around 85-90 beats per minute
Rhythm: Normal Sinus
Axis: Right axis
Intervals: narrow QRS, PR is a touch long, probably a first-degree AV block, QTc looks reasonable
Morphology: Some nonspecific ST-T wave changes, flattening of the T waves in the anterior leads, but overall looks reasonable. Poor R wave progression.
Final read: Sinus rhythm with a right axis
“I see sinus rhythm with a right axis!” The intern exclaims.
“Tell me a little more…” The upper year residents ask.
“Well, the QRS complex is negative in I and positive in aVF, which is suggestive of a right axis…” he begins.
“Keep looking at lead I and tell me what else you see,” The senior asks.
“Well, actually everything is inverted. The P wave is negative and so is the T wave too. That’s not normal. That means… hmmmm. Limb lead reversal! This ECG is no good.” And he turns to Mrs. Robinson.
“Mrs. Robinson, we’re going to have to repeat the ECG, I think the tech may have made a small mistake when she performed this test. I hope you don’t mind.” He says to her.
“Not at all, dear. Go right ahead.”
“Here’s the ECG machine, go ahead and get started” you say as you roll an ECG machine into Mrs. Robinson’s room.
You watch the intern struggle a little bit more than he should, but eventually, all of the leads end up in the right spot. The senior resident double checks the leads and gives him a thumbs up. He hits print and pulls up the ECG to show the team.
“Wait. What did I do wrong? It’s still inverted in lead I. We double checked the leads. What the heck?” you hear the intern ask the team.
You and Mrs. Robinson exchange a knowing smile as the team puzzles through what could be going on with her ECG.
What else could be going on here? Is there anything else that could cause a complete inversion in lead I?
Helping me explain Mrs. Robinson’s case today is Dr. Ioannis Protonotarios, resident physician at University Hospital Southampton in the UK! He writes the excellent substack “Squiggly Lines,” designed to make ECG interpretation easier by understanding the science behind it! Take it away Ioannis:
The intern’s reasoning was solid. Globally inverted Lead I almost always means someone swapped the arm electrodes (right-arm/left-arm lead reversal). It is the most commonly recognized lead misplacement, and checking for it first is the right instinct.
But the leads were checked. Twice. The ECG didn’t change.
So, before we look anywhere else, we need a more careful question: do we have enough on this ECG to call it a lead reversal at all?
Let’s look at what happens to each one when the arm cables get swapped (For a deeper dive into how the leads are produced see here):
- Lead I inverts. Recorded Lead I is the negative of true Lead I. P, QRS, and T are all mirrored across the baseline.
- Leads II and III swap. What gets printed as Lead II is the formula for true Lead III, and vice versa.
- aVR and aVL swap. The augmented formulas trade places.
- aVF is preserved. It compares the leg signal against the average of both arm signals. Swap the arm cables, and the average doesn’t change [1].
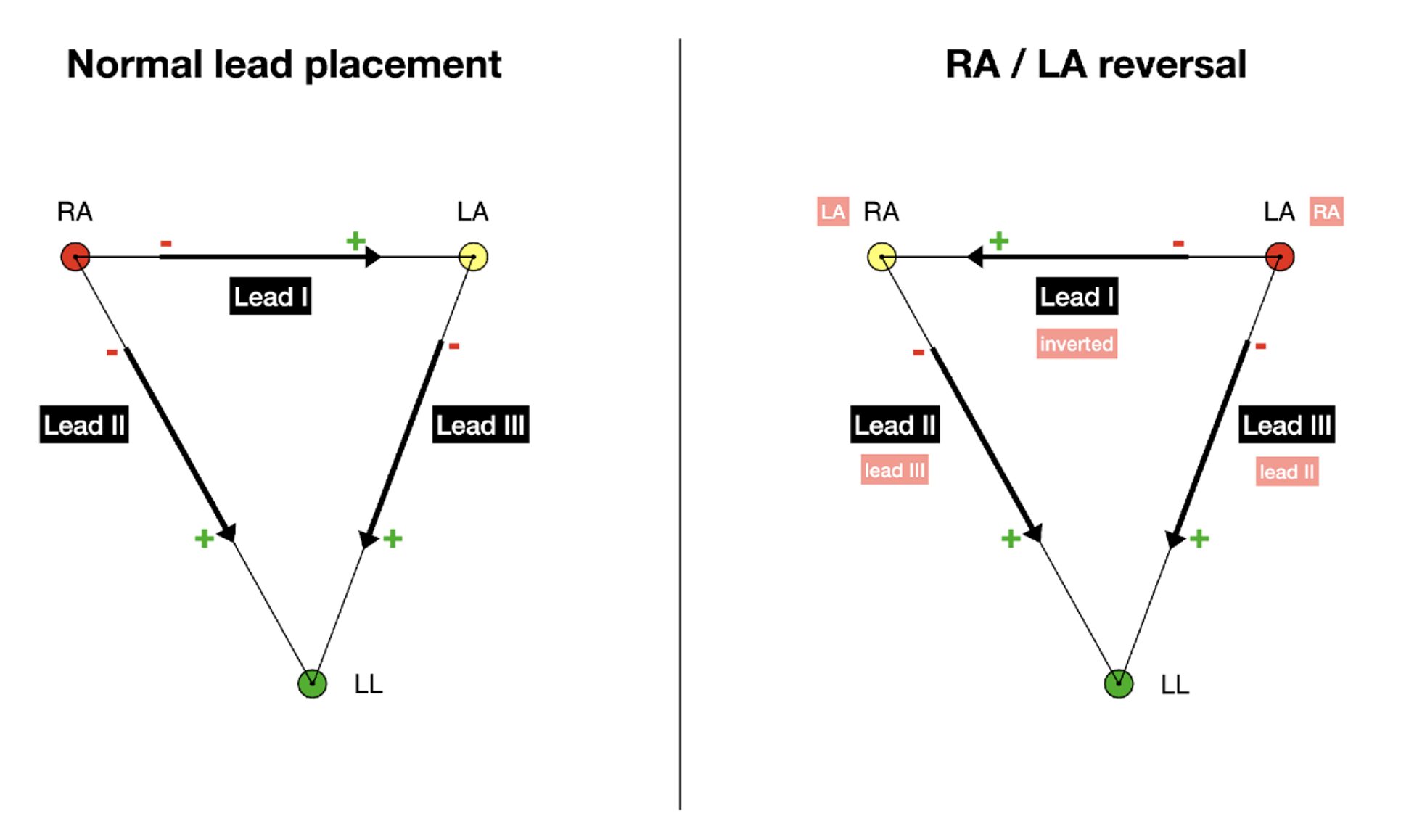
This image shows limb leads with normal cabling (left) vs RA/LA reversal (right). On the right panel, black labels show what the machine prints; soft-red tags show what the trace actually is. The cable physically attached to the left arm sits at the RA position (and vice versa); Lead I is inverted; the trace printed as Lead II is true Lead III, and the trace printed as Lead III is true Lead II.

Lead aVR with normal cabling (left) vs RA/LA reversal (right). Same color key (black = printed label, soft red = actual content): the aVR arrow still points at the upper-left vertex, but that cable is now physically attached to the left arm, so the trace printed as aVR is true aVL.
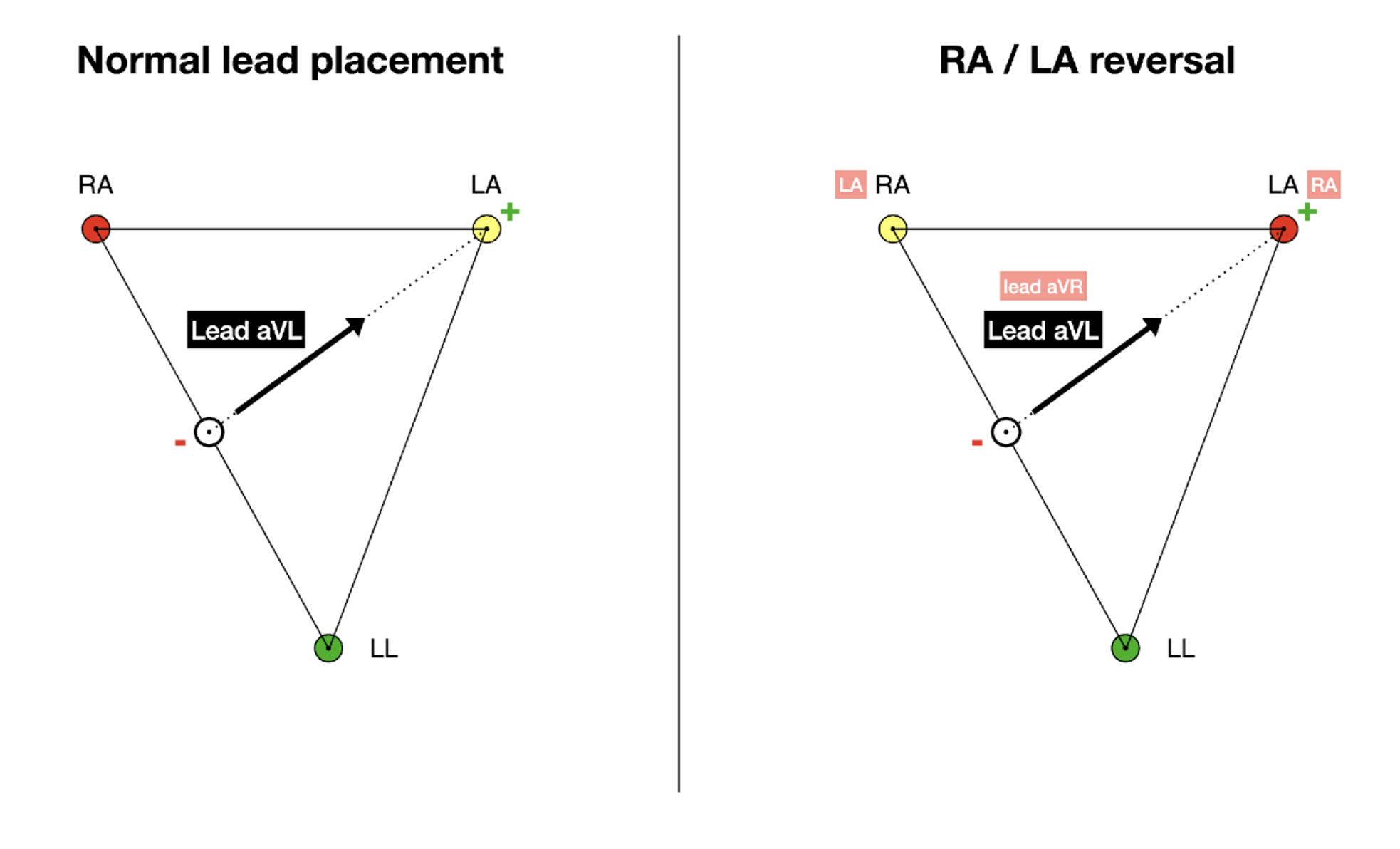
Lead aVL with normal cabling (left) vs RA/LA reversal (right). Same colour key. The aVL arrow still points at the upper-right vertex, but that cable is now physically attached to the right arm, so the trace printed as aVL is true aVR.
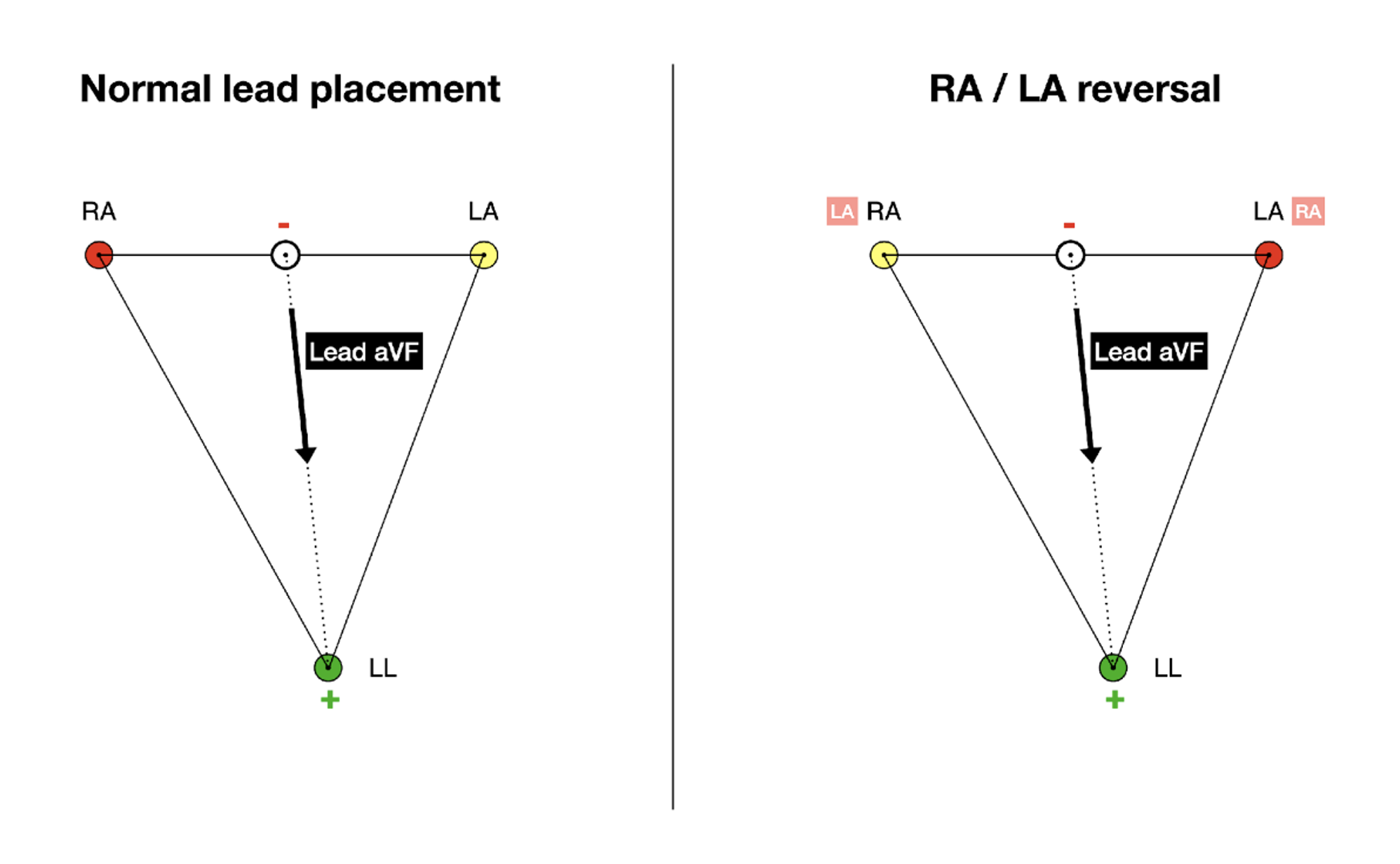
Lead aVF with normal cabling (left) vs RA/LA reversal (right). The arm cables swap, but (RA + LA)/2 equals (LA + RA)/2 and the leg cable hasn’t moved, so the aVF arrow gets no soft-red tag. The trace printed as aVF is true aVF.
Crucially, the precordial leads are untouched. The chest electrodes haven’t moved. The heart hasn’t moved. R wave progression is normal.
That is the fingerprint of a true RA/LA reversal.
Compare a textbook RA/LA reversal (shown below) to Mrs. Robinson’s actual ECG above.

License: Derivative of CardioNetworks: Drj (CC BY-SA 3.0, via Wikimedia Commons), modified by Ioannis Protonotarios with AI assistance. Distributed under CC BY-SA 3.0.
The precordial leads tell a different story
In the textbook reversal above, V1 to V6 shown normal R wave progression. The heart is on the left, and the precordial electrodes walk across the chest toward it.
Mrs Robinson’s tracing does the opposite. V1 carries the tallest R wave on the strip (albeit still small). Each subsequent precordial lead has a smaller R, and by V4 the positive deflection has vanished.
That is reverse R wave progression, and it is not what a lead reversal produces. The chest electrodes have not moved. So, if they are now recording a pattern that looks like the heart is somewhere unusual, the most likely explanation is that the heart actually is somewhere unusual. Take a look at Mrs. Robinson’s chest Xray and a shot from her chest CT:
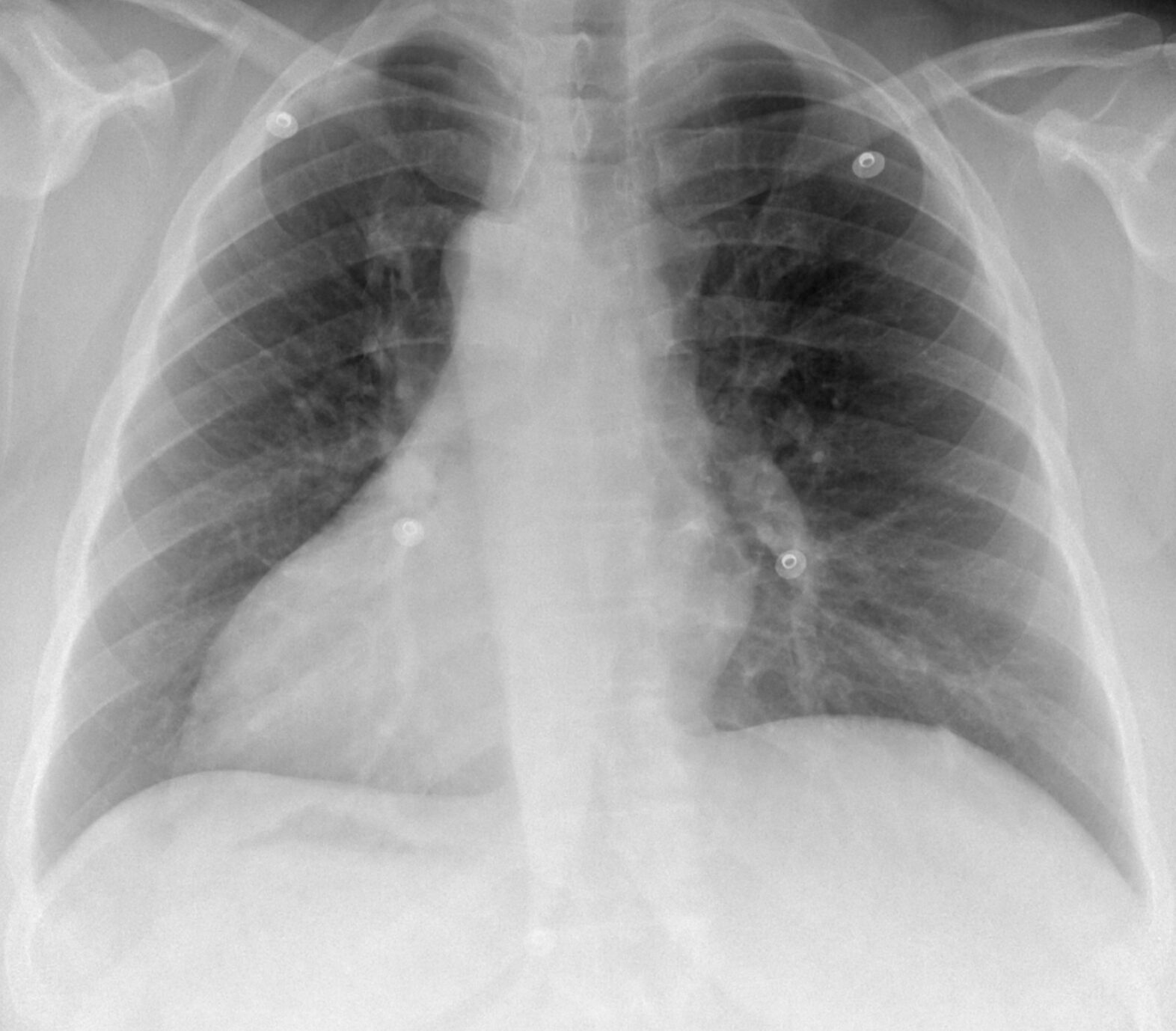
Mrs. Robinson’s chest X-ray. Three findings of situs inversus: cardiac silhouette on the right, dense liver shadow under the left hemidiaphragm, gastric bubble under the right.
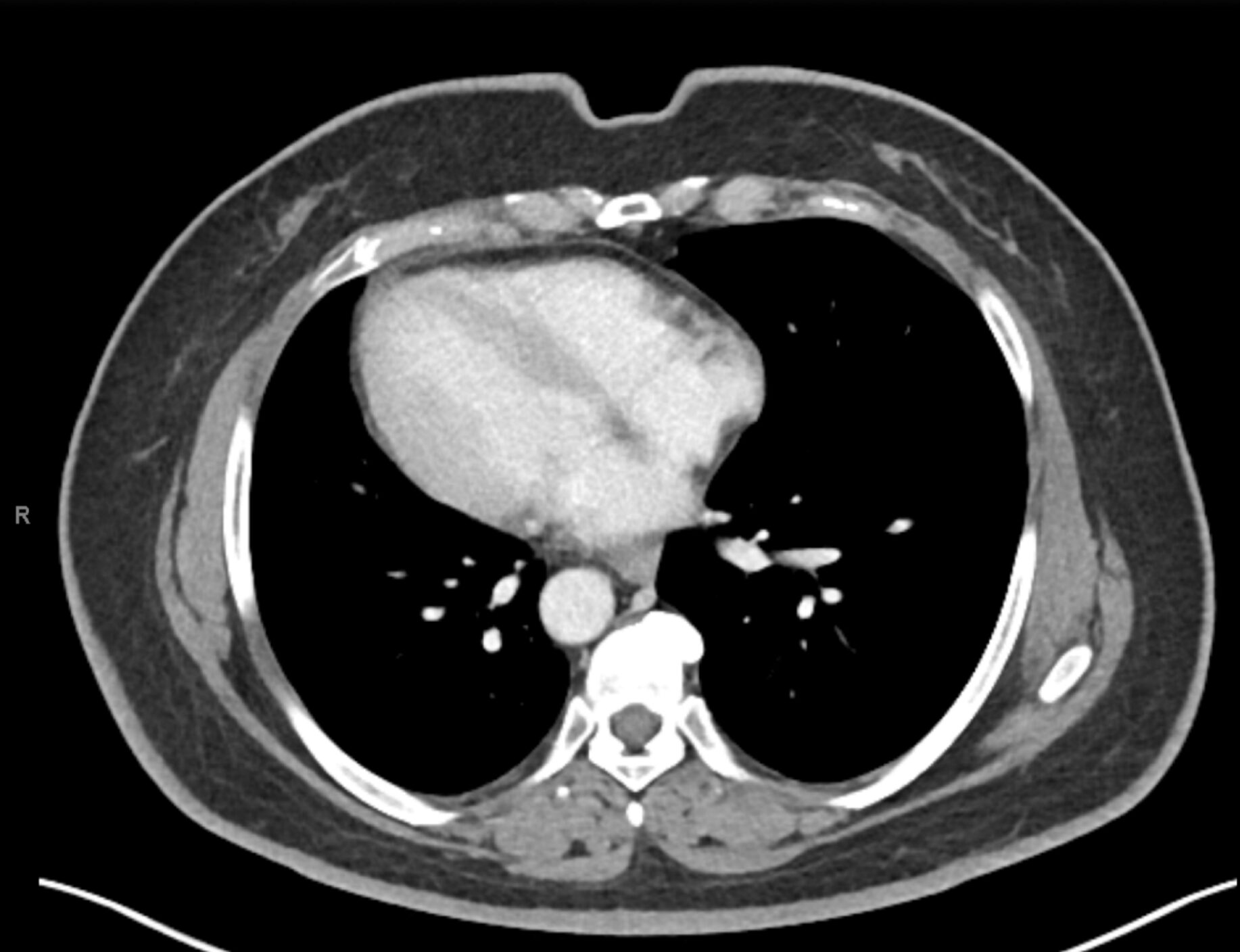
Transverse CT slice through Mrs. Robinson’s thorax. The cardiac mass fills the right hemithorax, a mirror image of normal anatomy.
Mrs. Robinson has dextrocardia. Her heart sits on the right side of her chest, a complete mirror image of normal. The chest X-ray shows more than just the cardiac position: the dense liver shadow sits under the left hemidiaphragm and the gastric air bubble sits under the right. The abdominal viscera are mirrored too. The diagnosis is situs inversus totalis: every thoracic and abdominal organ is reflected across the midline, the heart included [2,3].
What changes would we expect to see on an ECG in situs inversus?
- Lead I goes globally negative. Depolarization now heads away from the left arm (the positive pole), so P, QRS, and T are all inverted.
- aVR turns positive, aVL turns negative. With the apex now on the right, aVR points toward it and aVL points away.
- Lead III becomes more positive than lead II. Lead III’s axis lines up with the new vector. Lead II flattens or becomes negative.
- aVF is preserved. The mirror is left to right. The superior-inferior component of the vector is unchanged.
- Right axis (or extreme axis) deviation is automatic. Lead I negative: by definition, the axis sits beyond +90°.
Case Wrap up:
You let the team struggle for a few minutes before you nod to Mrs. Robinson.
“Would anyone like to listen to my heart? It may help!” You hear her call out to the residents.
“Sure, I’ll take a listen!” The intern replies. Suddenly you see his face fall. “Mrs. Robinson,” he says, “I’m not sure if it’s my stethoscope, but I can’t really hear very much of a heartbeat.”
“Well please don’t start CPR…” she tells him dryly. “Perhaps try listening on the other side. You see, I have dextrocardia…”
You and Mrs. Robinson exchange glances. “Maybe next year!” she tells you.
Recap:
This chart summarizes the major differences between Levocardia (traditional anatomy), Situs Inversus, and a RA/LA lead swap.
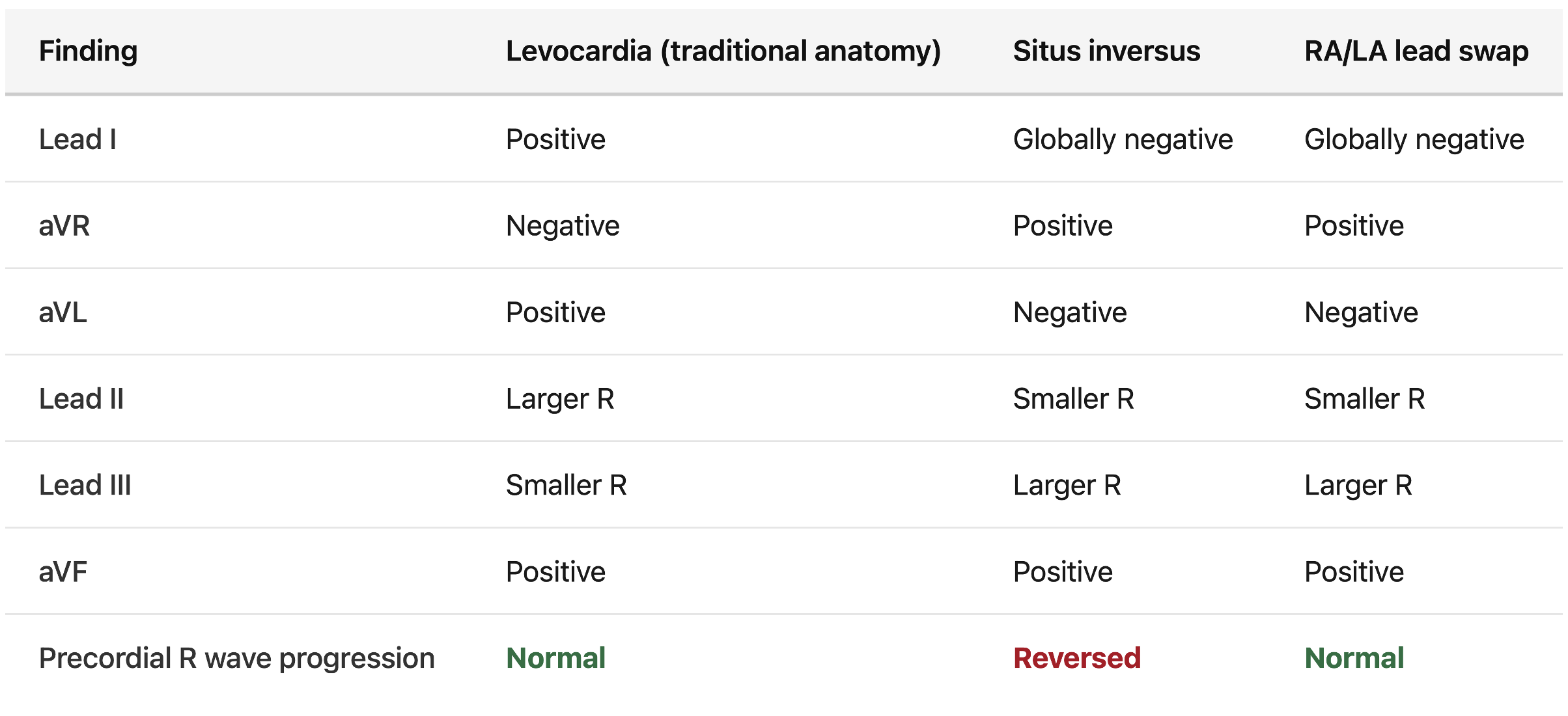
Levocardia: the common anatomy, with the heart sitting in the left hemithorax. Findings in this column assume a normal P-wave and QRS axis.
References:
– Paul A, Jacob JR. Electrocardiographic lead reversals. Indian Pacing Electrophysiol J. 2023 Nov-Dec;23(6):205-213. doi: 10.1016/j.ipej.2023.09.005. Epub 2023 Sep 20. PMID: 37739313; PMCID: PMC10685096.
– Maldjian PD, Saric M. Approach to dextrocardia in adults: review. AJR Am J Roentgenol. 2007;188(6 Suppl):S39-S38. doi:10.2214/AJR.06.1179
– Nair R, Muthukuru SR. Dextrocardia. [Updated 2022 Sep 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK556074/




