
Author: Eric Sulava, MD (EM Resident, USUHS, USN) and Erica Simon, DO, MHA (@E_M_Simon, EM Chief Resident, SAUSHEC, USAF) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Attending Physician, SAUSHEC, USAF)
Welcome to EM@3AM, an emdocs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 36-year-old male presents to the emergency department after being found down at home by his spouse. Per the man’s wife, the patient is a heavy drinker – often consuming two to three pints of vodka daily. Upon EMS arrival the male is noted to be anxious and tremulous with a GCS of 14.
Initial vital signs: HR 136, BP 172/82, RR 24, T 37.2, SpO2 97% RA
What do you suspect as the diagnosis? What is the next step in evaluation and treatment?
Answer: Alcohol Withdrawal Syndrome (AWS)1-6
- Pathophysiology: Alcohol => CNS depressant. It potentiates GABA receptors (enhances inhibitory tone) and antagonizes the NMDA receptors (inhibits excitatory tone).1 Withdrawal => CNS hyperexcitation and hyperstimulation.
- Presentation: Four stages (clinically unreliable due to non-sequential progression and overlap of signs/symptoms):2,3
- 6-12 Hours => Tremors, anxiety, gastrointestinal upset, anorexia, nausea, diaphoresis, palpitations, tachycardia, hypertension
- 12-24 Hours => Alcoholic hallucinations (visual, auditory, or tactile in nature); occur in 3-5% of patients3
- 24-48 Hours => Withdrawal seizures (generalized tonic-clonic)
- 3-5 Days => Delirium Tremens
- Evaluation: AWS is a diagnosis of exclusion. The use of a grading scale to assess symptoms is advised (Clinical Institute Withdrawal Assessment – Alcohol, revised (CIWA-Ar)).2-5
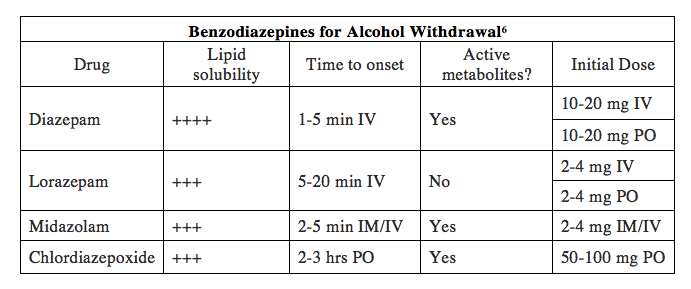
- Treatment: Address ABCs. Benzodiazepines are first line (no single agent demonstrates superiority in treatment6):
- Pearls:
- Consider structural CNS pathology, metabolic abnormalities, infection, and toxicologic etiologies prior to assigning a diagnosis of AWS.
- When interviewing the patient, question specifically regarding reasons for cessation of alcohol consumption =>may allow for identification of a concomitant condition (MI, pancreatitis, etc.)
References:
- Kosten T, O’Connor P. Management of drug and alcohol withdrawal. N Engl JMed. 2003; 348:1786-1795.
- Gortney J, Raub J, Patel P, et al. Alcohol withdrawal syndrome in medical patients. Cleve Clin J Med. 2016; 83(1): 67-79.
- Muncie H, Yasinian Y, Oge L. Outpatient management of alcohol withdrawal syndrome. Am Fam Physician. 2013; 88(9): 589-595.
- Perry E. Inpatient management of acute alcohol withdrawal syndrome. CNS Drugs. 2014; 28(5): 401-410.
- Sullivan J, Sykora K, Schneiderman J, et al. Assessment of alcohol withdrawal: the revised clinical institute withdrawal assessment for alcohol scale (CIWA-Ar). Br J Addict. 1989; 84(11): 1353-1357.
- Yanta J, Swartzentruber G, Pizon A. Alcohol withdrawal syndrome: improving outcomes through early identification and aggressive treatment strategies. Emerg Med Pract. 2015; 17(6): 1-19.
For Additional Reading:
Alcohol Withdrawal: Pearls and Pitfalls:




