
Author: Rachel Bridwell, MD (@rebridwell, EM Attending Physician) // Reviewed by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital); Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 33-year-old male presents to the ED for odynophagia and mild dyspnea. He has had pain with swallowing for the past 24 hours and it has gotten progressively worse. He is having difficulty tolerating oral secretions. Review of systems is otherwise unremarkable, and he is up to date on immunizations.
Triage vital signs include BP 91/49, HR 130, T 102.2 temporal, RR 25, SpO2 91% on room air. He appears toxic. The ENT exam reveals a midline uvula; cervical lymphadenopathy; soft mouth floor, and no evidence of dental infection, no neck erythema, though voice changes. He has severe pain with palpation of the hyoid bone.
What’s the most likely diagnosis?
Answer: Epiglottitis1-35
Epidemiology
- Steadily increasing with an incidence of 1/100,000 to 4/100,000 in the U.S. in adults
- Pediatric incidence has decreased to 0.5/100,000
- Previously more common in unvaccinated children, but now more common in adults
- Life-threatening infection of epiglottis
- Occurs via direct invasion of the epithelial layer by the organism or by bacteremia
- Bacteremia more commonly associated with pediatric epiglottitis, though does not correlate to the severity of infection
- Edema and inflammatory cell accumulation in the potential space between the epiglottic cartilage and epithelial layer, resulting in swelling of the epiglottis and supraglottic structures
- Occurs via direct invasion of the epithelial layer by the organism or by bacteremia
- Often bacterial though can occur via viral or fungal infection, foreign body ingestion, thermal injury, lymphoproliferative disease or graft-versus-host disease, chronic granulomatous diseases, and caustic ingestions.
Microbiology
- Often polymicrobial, and predominant bacteria include:
- Streptococcus pyogenes (group A strep), Staphylococcus aureus (MSSA, MRSA)
- Pseudomonas aeruginosa should be considered in immunocompromised patients
Evaluation
- Adult patients present with:
- 90-100% with odynophagia
- 85% with dysphagia
- 74% with voice changes
- Tripod positioning less common in adults due to larger airway caliber, occurring in less than 50% of adult patients
- Voice change
- Retractions
- Rapid onset of symptoms within 12-24 hours is a harbinger of severe disease, though adults usually present in subacute fashion
Examination
- 90% of patients with epiglottitis with have a normal oropharyngeal exam
- Fever in 26-90%
- Muffled voiced in 50-65%
- Difficulty handling secretions 50-80%
- Cervical lymphadenopathy
- Severe pain with palpation of the external larynx or hyoid bone
- Direct visualization of the epiglottis with nebulized lidocaine
- Clinician should face the patient and places the Macintosh blade onto patient’s tongue.
- Ask patient to speak in a high-pitched tone, raising the supraglottic structures several centimeters for potential visualization
Laboratory analysis
- Limited utility since clinical diagnosis:
- Cultures
- Blood: 0-17% yield
- Throat: 10-33% yield
- Epiglottis: 75% yield
- Dehydration due to odynophagia
- Cultures
Imaging
- Upright lateral neck radiograph
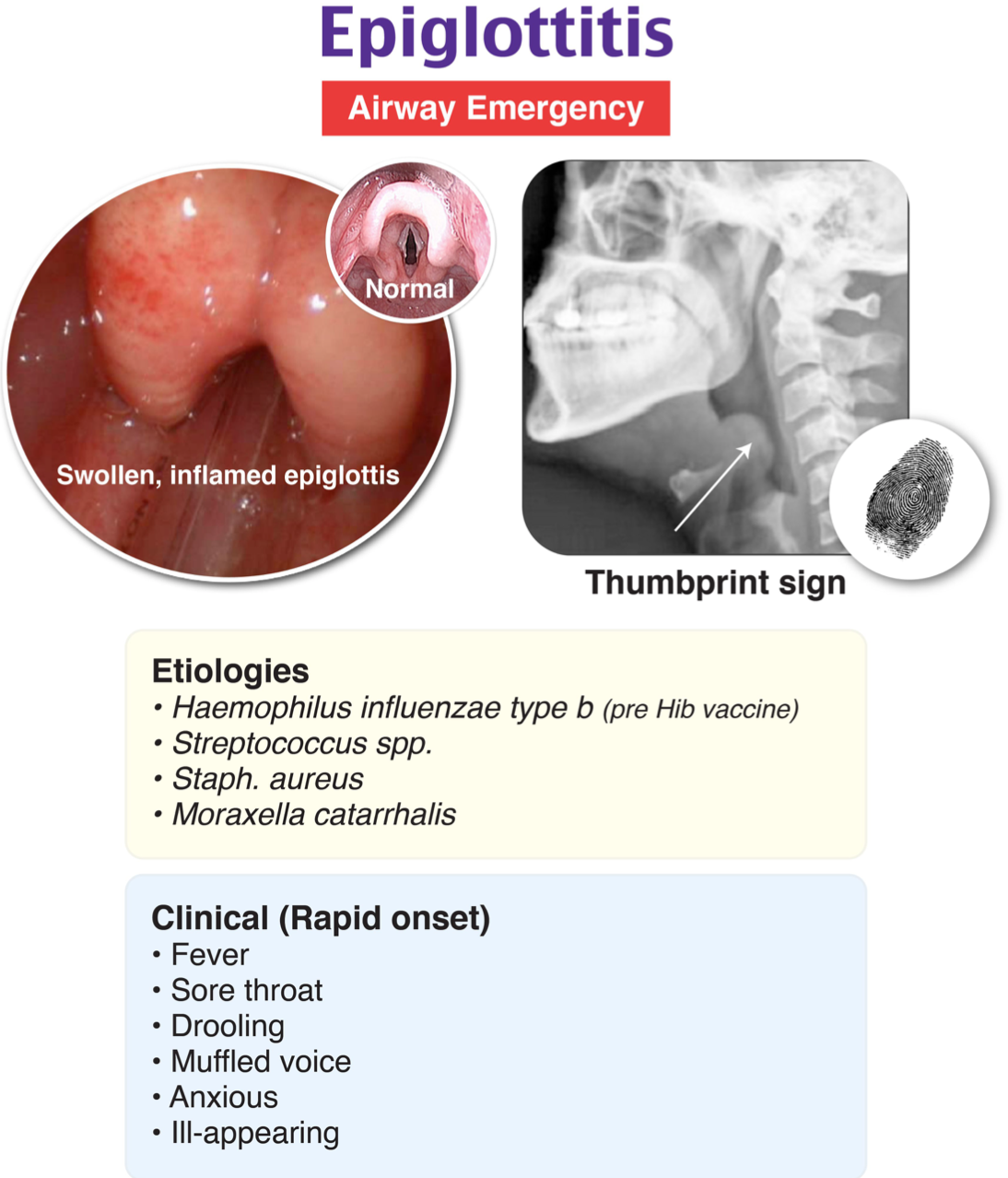
- Thumbprint sign: epiglottic swelling with a sensitivity of 89.2% and specificity of 92.2%
- Vallecula sign: normal deep linear air space from the base of the tongue to the epiglottis is shallow or absent
- Epiglottic width greater than 6.3 mm demonstrates has a sensitivity of 75.8% and a specificity of 97.8%.
- False negative rate of 31.9% so negative radiograph does not rule out diagnosis
- Computed Tomography (CT) with contrast of the neck
- Requires patient to lay supine
- May aggravate impending airway occlusion
- Sensitivity of 88-100% and specificity of 97-96%
- Can show:
- Effusion
- Obliteration of surrounding fat planes
- Thickening of false vocal cords
- Retropharyngeal enhancement and edema
- Epiglottic abscess: Associated with a high likelihood of requiring airway
- Requires patient to lay supine
- Point of care ultrasound
- Allows for evaluation in position of comfort
- Increased anteroposterior diameter of the midpoint and lateral epiglottis associated with epiglottitis
- Alphabet P sign is also suggestive of epiglottitis
- hypoechogenicity on a longitudinal view at the thyrohyoid membrane level
- Direct visualization of epiglottis confirms diagnosis—set up for therapeutic intervention simultaneously
Treatment
- Position of optimal patient comfort is key
- Airway management
- Intubation with flexible intubating endoscopy is the method of choice
- Intubation occurs in epiglottitis patients in 13.2% of cases
- Video laryngoscopy is used less commonly but is also an option
- Do not use supraglottic devices; may not seat well and may cause airway occlusion
- Factors associated with increased likelihood of intubation:
- Historical factors: Diabetes mellitus, subjective dyspnea, rapid symptom progression over 12-24 hours, stridor,
- Objective measures: 20 breaths per minute with subjective complaint of dyspnea required visualization of the airway, while a respiratory rate greater than 30 breaths per minute, hypercarbia (PCO2 greater than 45 mm Hg)
- Factors associated with increased likelihood of intubation:
- Antibiotics:
- Ceftriaxone 2g intravenous (IV) or ampicillin-sulbactam 3g IV with vancomycin 20 mg/kg IV for methicillin resistant Staphylococcus aureus (MRSA) coverage
- Severe penicillin allergy: levofloxacin 750 mg IV
- Immunocompromised: cefepime 2g IV is recommended for P. aeruginosa coverage
- Corticosteroids are controversial though between 20-83% will receive corticosteroids
- Have not demonstrated any improvement in ICU length of stay, hospital length of stay, or duration of intubation
- Nebulized epinephrine may help temporize airway by assisting with bronchodilation
- Do not use in children
- Generates additional agitation, laryngospasm and rapid deterioration though no benefit
- Do not use in children
Pearls
- More common in adults who present with odynophagia, dysphagia, and over a more subacute time frame
- Normal oropharynx occurs in 90% of adults with epiglottitis
- Lateral neck radiographs are a screening tool which may show the thumbprint or vallecula sign though have a high false positive rate
- Factors associated with increased rates of intubation are diabetes mellitus, symptoms over 12-24 hours, stridor, drooling, tachypnea, hypercarbia, epiglottic abscess, and subglottic extension
- Airway management has shifted from intubation/surgical airway in the operating room to awake fiberoptic intubation
- Corticosteroids and nebulized epinephrine may assist in decompensating patients, but the literature is controversial

A 4-year-old girl presents with fever and sore throat. Her symptoms started yesterday evening and became acutely worse today. Her vital signs are HR 165, RR 30, and temp 38.8 °C. She appears anxious and is maintaining a “sniffing” position with her jaw thrusting forward. She has audible stridor without wheezing. What is the most likely diagnosis?
A) Croup
B) Epiglottitis
C) Retropharyngeal abscess
D) Tracheitis
Epiglottitis is an inflammation of the epiglottis, aryepiglottic folds, arytenoids, and surrounding supraglottic tissues. This condition can be caused by an infection or by trauma. The classical organism that leads to epiglottitis is Haemophilus influenzae type b (Hib), but other types of Haemophilus influenzae can cause epiglottitis in addition to group A beta-hemolytic Streptococcus, Staphylococcus aureus, and Streptococcus pneumoniae. The introduction of the HIB vaccine has reduced the occurrence of this disease. Epiglottitis affects children between 3 and 7 years of age and has a worse presentation in younger patients. Epiglottitis is characterized by acute onset of upper airway obstruction. Drooling can be prominent, and patients maintain a tripod or “sniffing” position that helps open the airway. The diagnosis is clinical but a lateral neck X-ray can show a ‘thumbprint’ sign signifying an enlarged epiglottis. Direct examination or manipulation of the pharynx should be avoided in the initial evaluation as it can exacerbate symptoms. Supplemental oxygen can be provided by the least invasive method. A number of techniques can be attempted in patients who are rapidly deteriorating, and these include bag-valve-mask ventilation, fiberoptic intubation, needle cricothyroidotomy, or tracheostomy. These techniques should be used as a temporary measure until emergent expert consult in airway management is obtained from an anesthesiologist, otolaryngology, or general surgeon. Patients should be admitted to the pediatric critical care floor once the airway is secure for monitoring and treatment. They are usually kept intubated for three to five days while antibiotic therapy and time allow for an adequate decrease in edema.
Croup (A) is the most commonly assigned misdiagnosis of epiglottitis. Croup is a viral laryngotracheitis caused primarily by the parainfluenza virus. Patients with croup present with a barking cough and stridor. Drooling and difficulty swallowing are not prominent in patients with croup. Tracheitis (D) is usually caused by a bacterial infection of the trachea. It can also develop as a complication of croup. Tracheitis presents with several days of a prodrome of viral upper respiratory infection symptoms including cough and fever, which progress to inspiratory and expiratory stridor before becoming more severe. Retropharyngeal abscess (C) is often related to oral trauma and manifests with a muffled voice, dysphagia, and fever. Patients may also have pain with neck movement. A lateral neck X-ray in extension will show a widened retropharyngeal space, which is typically less than half of the vertebral body at C2 level in children less than 5 years of age. The rapidity of this patient’s symptom progression points more to a diagnosis of epiglottitis.
Further Reading
Additional FOAM Resources:
- https://coreem.net/core/epiglottitis/
- https://rebelem.com/rebel-core-cast-11-0-epiglottitis/
- https://emcrit.org/ibcc/epiglottitis/
- https://www.tamingthesru.com/blog/minor-care-series/more-than-a-sore-throat-acute-epiglottitis
References:
- Shah RK, Nussenbaum B, Kienstra M, et al. Wrong-site sinus surgery in otolaryngology. Otolaryngol Head Neck Surg. 2010;143(1):37-41. doi:10.1016/J.OTOHNS.2010.04.003
- Hermansen M, Schmidt J, Krug A, Larsen K, Kristensen S. Low incidence of children with acute epiglottitis after introduction of vaccination. Dan Med J. 2014;61(4):A4788.
- Guldfred LA, Lyhne D, Becker BC. Acute epiglottitis: epidemiology, clinical presentation, management and outcome. J Laryngol Otol. 2008;122(8):818-823. doi:10.1017/S0022215107000473
- Bizaki AJ, Numminen J, Vasama JP, Laranne J, Rautiainen M. Acute supraglottitis in adults in Finland: review and analysis of 308 cases. Laryngoscope. 2011;121(10):2107-2113. doi:10.1002/LARY.22147
- McVernon J, Slack MPE, Ramsay ME. Changes in the epidemiology of epiglottitis following introduction of Haemophilus influenzae type b (Hib) conjugate vaccines in England: a comparison of two data sources. Epidemiol Infect. 2006;134(3):570. doi:10.1017/S0950268805005546
- Mayo-Smith MF, Spinale JW, Donskey CJ, Yukawa M, Li RH, Schiffman FJ. Acute epiglottitis. An 18-year experience in Rhode Island. Chest. 1995;108(6):1640-1647. doi:10.1378/CHEST.108.6.1640
- Berger G, Landau T, Berger S, Finkelstein Y, Bernheim J, Ophir D. The rising incidence of adult acute epiglottitis and epiglottic abscess. Am J Otolaryngol. 2003;24(6):374-383. doi:10.1016/S0196-0709(03)00083-8
- Lichtor JL, Rodriguez MR, Aaronson NL, Spock T, Goodman TR, Baum ED. Epiglottitis: It Hasn’t Gone Away. Anesthesiology. 2016;124(6):1404-1407. doi:10.1097/ALN.0000000000001125
- Guardiani E, Bliss M, Harley E. Supraglottitis in the era following widespread immunization against Haemophilus influenzae type B: evolving principles in diagnosis and management. Laryngoscope. 2010;120(11):2183-2188. doi:10.1002/LARY.21083
- Felton P, Lutfy-Clayton L, Smith LG, Visintainer P, Rathlev NK. A Retrospective Cohort Study of Acute Epiglottitis in Adults. West J Emerg Med. 2021;22(6):1326-1334. doi:10.5811/WESTJEM.2021.8.52657
- Tanner K, Fitzsimmons G, Carrol ED, Flood TJ, Clark JE. Haemophilus influenzae type b epiglottitis as a cause of acute upper airways obstruction in children. BMJ. 2002;325(7372):1099. doi:10.1136/BMJ.325.7372.1099
- Madhotra D, Fenton JE, Maura ZGG, Charters P, Roland NJ. Airway intervention in adult supraglottitis. Ir J Med Sci. 2004;173(4):197-199. doi:10.1007/BF02914550
- Hébert PC, Ducic Y, Boisvert D, Lamothe A. Adult epiglottitis in a Canadian setting. Laryngoscope. 1998;108(1 Pt 1):64-69. doi:10.1097/00005537-199801000-00012
- Katori H, Tsukuda M. Acute epiglottitis: analysis of factors associated with airway intervention. J Laryngol Otol. 2005;119(12):967-972. doi:10.1258/002221505775010823
- Glynn F, Fenton JE. Diagnosis and management of supraglottitis (epiglottitis). Curr Infect Dis Rep. 2008;10(3):200-204. doi:10.1007/S11908-008-0033-8
- Frantz T, Rasgon B, Quesenberry Jr C. Acute epiglottitis in adults. Analysis of 129 cases. JAMA. 1994;272(17):1358-1360.
- Hafidh MA, Sheahan P, Keogh I, Walsh RMC. Acute epiglottitis in adults: a recent experience with 10 cases. J Laryngol Otol. 2006;120(4):310-313. doi:10.1017/S0022215106000399
- Sideris A, Holmes TR, Cumming B, Havas T. A systematic review and meta-analysis of predictors of airway intervention in adult epiglottitis. Laryngoscope. 2020;130(2):465-473. doi:10.1002/LARY.28076
- Smith M, Mukherji S, Thompson J, Castillo M. CT in adult supraglottitis. AJNR Am J Neuroradiol. 1996;17(7):1355-1358.
- Ramalanjaona G, Shpak M. Challenges in Diagnosing Adult Epiglottitis: Limitations of CT scan. Emerg Med – Open J. 2015;1(1):1-4. doi:10.17140/emoj-1-101
- Lee SH, Yun SJ, Kim DH, Jo HH, Ryu S. Do we need a change in ED diagnostic strategy for adult acute epiglottitis? Am J Emerg Med. 2017;35(10):1519-1524. doi:10.1016/J.AJEM.2017.04.039
- Hung TY, Li S, Chen PS, et al. Bedside ultrasonography as a safe and effective tool to diagnose acute epiglottitis. Am J Emerg Med. 2011;29(3):359.e1-359.e3. doi:10.1016/J.AJEM.2010.05.001
- Pineau PM, Gautier J, Pineau A, Emam N, Laccourreye L, Boucher S. Intubation decision criteria in adult epiglottitis. Eur Ann Otorhinolaryngol Head Neck Dis. 2021;138(5):329-332. doi:10.1016/J.ANORL.2020.12.001
- Shah RK, Stocks C. Epiglottitis in the United States: national trends, variances, prognosis, and management. Laryngoscope. 2010;120(6):1256-1262. doi:10.1002/LARY.20921
- Mathoera R, Wever P, van Dorsetn F, Balter S, de Jager C. Epiglottitis in the adult patient. Neth J Med. 2008;66(9):373-377.
- Zulliger JJ, Schuller DE, Beach TP, Garvin JP, Birck HG, Frank JE. Assessment of intubation in croup and epiglottitis. Ann Otol Rhinol Laryngol. 1982;91(4 Pt 1):403-406. doi:10.1177/000348948209100417
- Cheung CSK, Man SY, Graham CA, et al. Adult epiglottitis: 6 years experience in a university teaching hospital in Hong Kong. Eur J Emerg Med. 2009;16(4):221-226. doi:10.1097/MEJ.0B013E328320AD2F
- Hanna J, Brauer PR, Berson E, Mehra S. Adult epiglottitis: Trends and predictors of mortality in over 30 thousand cases from 2007 to 2014. Laryngoscope. 2019;129(5):1107-1112. doi:10.1002/LARY.27741
- Rafei K, Lichenstein R. Airway infectious disease emergencies. Pediatr Clin North Am. 2006;53(2):215-242. doi:10.1016/J.PCL.2005.10.001
- Sobol SE, Zapata S. Epiglottitis and croup. Otolaryngol Clin North Am. 2008;41(3):551-566. doi:10.1016/J.OTC.2008.01.012
- Andreassen U, Baer S, Nielsen T, Dahm S, Arndal H. Acute epiglottitis–25 years experience with nasotracheal intubation, current management policy and future trends. J Laryngol Otol. 1992;106(12):1072-1075. doi:10.1017/S0022215100121784
- Maisel A. B-type natriuretic peptide levels: Diagnostic and prognostic in congestive heart failure: What’s next? Circulation. 2002;105(20):2328-2331. doi:10.1161/01.CIR.0000019121.91548.C2
- Mandal A, Kabra SK, Lodha R. Upper Airway Obstruction in Children. Indian J Pediatr 2015 828. 2015;82(8):737-744. doi:10.1007/S12098-015-1811-6
- Kissoon N, Mitchell I. Adverse effects of racemic epinephrine in epiglottitis. Pediatr Emerg Care. 1985;1(3):143-144. doi:10.1097/00006565-198509000-00008
- Richards AM. Pediatric Respiratory Emergencies. Emerg Med Clin North Am. 2016;34(1):77-96. doi:10.1016/J.EMC.2015.08.006




