
Author: Sean O’Hara, MD (EM Attending Physician, San Antonio, TX) and Rachel Bridwell, MD (EM Resident, San Antonio, TX) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 31-year-old female presents with headache. She has a history of migraines, but states that this headache is different from her normal headache. The headache came on over the past two days, but she has been having intermittent double vision when she changes positions, which is new for her. She has no other medical problems.
Initial VS include T 36.0, HR 75, BP 120/65, RR 18, SpO2 97% RA.
Exam reveals an obese female in no acute distress. Visual acuity is normal, but she has mild left sixth nerve palsy. Fundoscopic exam reveals bilateral papilledema. The rest of her neurologic exam is unremarkable.
What do you think is going on with this patient? What are the next steps in management?
Answer: Idiopathic Intracranial Hypertension (IIH)
- Background: Also known as pseudotumor cerebri, IIH is a disorder characterized by signs of increased intracranial pressure (headaches, vision loss, and papilledema) with no other cause detected on neuroimaging or other evaluations.
- Primarily affects obese women of childbearing age (women affected at 20 times the rate of men) but can occur in all patient groups. More severe in non-classic patients because of diagnostic delay. Pre-adolescent children less likely to be obese, with equal gender distribution.
- Approximately 2 per 100,000 people are affected per year.
- Deficits usually occur over months to years, but certain patients can have rapidly progressive IIH over weeks. Typically, the more severe deficits are at presentation, the higher chance of permanent disability.
- Typically idiopathic due to impaired CSF absorption. Associated with oral contraceptives, vitamin A, tetracyclines, lithium, thyroid disorders.
- Permanent visual loss is the primary morbidity, affecting 10-25% of patients with IIH.
- Evaluation: History and exam are often benign, but it is vital to consider the disease.
- History: Most common complaint headache, most often similar to primary headache disorders, but can be absent. Transient visual disturbances (bilateral or unilateral), pulsatile tinnitus, diplopia, nausea, vomiting are other signs of increased ICP. Important to determine if recent head/neck surgeries, if patient on medications associated with IIH (isoretinoin, tetracyclines, lithium, steroids, etc.), allergies, or other systemic disorders.
- Exam: Look for signs of secondary causes of increased ICP (mass, ICH, meningitis, malignant hypertension, etc.). Neurologic exam often normal. Hallmark physical exam findings are papilledema or cranial nerve palsy (VI). Visual acuity often normal, but common to have visual field deficits (inferior nasal field deficit most common). Possible to have IIH without signs of papilledema, CN palsy, or visual field deficits – often in non-typical patient groups like children or men. Fundoscopy is important, but is often difficult. Ultrasound can assist (see below).
- Obtain:
- Labs – CBC, BMP, LFTs, HCG for females.
- Neuroimaging –MRI with MRV preferred imaging, but suitable to obtain CT in patients not able to tolerate MRI. MRV is important in the evaluation for cerebral venous thrombosis. MRI able to evaluate for other causes of increased ICP more specifically, but often difficult to obtain. Some findings on MRI that suggest IIH include narrowing of transverse venous sinus, empty sella, and flattening of posterior sclera, but none are diagnostic.
- Ultrasound – Not diagnostic, but can confirm elevated ICP (still need to exclude other sources of increased ICP). Optic nerve sheath diameter >5-6 mm is typically associated with ICP pressure >20cm H20 (> 6 mm is reliable for increased ICP, while < 5 mm suggests no elevation in ICP).
- LP – Need to obtain in lateral decubitus position with legs extended in order to measure opening pressure. Opening pressure considered elevated if >25 cm H2O, normal if <20cm H2O, and equivocal if between 20 and 25. MRI can help differentiate equivocal cases. CSF studies (cell count, gram stain, culture, protein, glucose) are normal in IIH.
- Differential Diagnosis: Intracranial tumors, abscesses, venous sinus thrombosis, hydrocephalus, jugular vein thrombosis, malignant hypertension, meningitis, subarachnoid hemorrhage, steroid withdrawal, severe iron deficiency anemia.
- Official Diagnosis (modified Dandy criteria): symptoms of increased ICP, no localizing signs with exception of 6thnerve palsy, patient is awake/alert, normal central imaging findings with no evidence of thrombosis, LP opening pressure > 25 cm but otherwise normal CSF, no other explanation for increased ICP.
- Management:
- Weight loss if obese: Associated with decreased papilledema, quicker improvement of visual symptoms. Weight gain is risk factor for recurrence of IIH.
- Medical Therapy: Carbonic anhydrase inhibitors are mainstay of medical management, thought to decrease CSF production.
- Acetazolamide is first line treatment for IIH. For adults, start at 500mg BID, advance dose as tolerated (max dose 2-4g per day). For children, start at 25mg/kg per day (max dose 2g per day). Side effects typically limit max dose and include paresthesias, fatigue, nausea, vomiting, and electrolyte changes. Acetazolamide may be used in patients with minor sulfa allergy (not suitable to use in patients with history of anaphylaxis or SJS, for example).
- Furosemide can be used in addition to acetazolamide. Typical dosages are 20-40mg daily for adults, and 1-2mg/kg daily for children.
- Topiramate has also been utilized as treatment for IIH but hasn’t been adopted as a first line treatment.
- Steroids are no longer recommended for routine use.
- Surgical Therapy: Only considered in rapidly progressing IIH or for patients on maximal medical therapy with progression of symptoms. Serial lumbar punctures have fallen out of favor and are only used in extreme cases (i.e. vision loss) while awaiting more definitive surgical management. Two options for surgical management include optic nerve sheath fenestration (ONSF) or CSF shunting.
- ONSF: Used to improve visual symptoms but is typically not associated with headache improvement. Stabilizes vision in approximately 90% of patients. Can fail, requiring repeat ONSF.
- CSF Shunting: Completed through either ventriculoperitoneal or lumboperitoneal shunts. Almost complete headache relief initially, with variable improvement in visual symptoms. Typically headaches recur within several years. Higher rate of complications than ONSF.
- Disposition:
- Referral to Neuro-Ophthalmologist – Evaluate if necessary to have emergent ONSF.
- Referral to Neurologist —For initiation of medical management, potential referral to neurosurgery for CSF shunting procedures.
- Admit patients with significant vision changes, focal findings (consider another pathology), and severe pain.

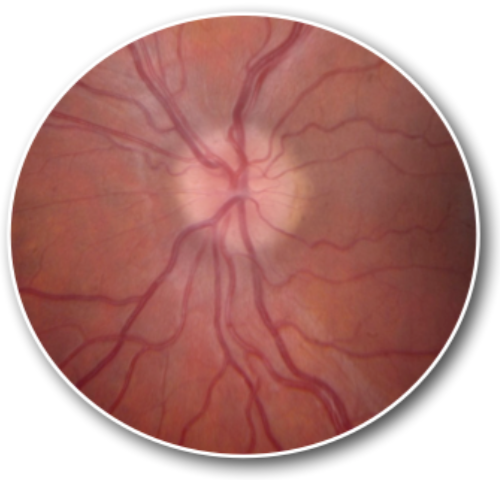
A 14-year-old obese girl presents with a headache. She states that the headache has been on and off for weeks and has a moderate intensity. She also states that she has had intermittent loss of vision for seconds at a time for the last two to three days. Physical examination reveals the above image. A noncontrast head CT scan is normal. What is the next best step in management?
A) Acetazolamide
C) Lumbar puncture with opening pressure
D) Symptomatic management and follow up
Answer: C
This patient presents with symptoms and signs consistent with idiopathic intracranial hypertension (IIH) and should have a lumbar puncture with an opening pressure performed to make the diagnosis. The pathophysiology of IIH is not completely understood but is thought to be due to an imbalance of CSF production and reabsorption. Patients typically present with a generalized headache of gradual onset. The headache is worsened by Valsalva maneuver or bending over. Patients may also present with visual complaints that are transient or continuous. Patients may have visual field defects or frank vision loss. The hallmark physical exam finding is papilledema, as seen in the patient above. It is typically bilateral and symmetric. Sixth cranial nerve (abducens) palsy may also be present. The diagnosis of IIH is made by a lumbar puncture with an increased opening pressure. Making the diagnosis is critical as it affects management and appropriate management can avoid the most common complication which is vision loss.

Acetazolamide (A) and corticosteroids (B) are treatments for IIH but should not be started until a definitive diagnosis is made. Symptomatic management and follow up (D) should not be used as diagnosis is critical.
Further Reading:
- FOAMed:
- References:
- Jones JS et al (October 1999). “Emergency department presentation of idiopathic intracranial hypertension”. AJEM. 17(6): 517-521.
- Agarwal MR, Yoo JH (November 2007). “Optic nerve sheath fenestration for vision preservation in idiopathic intracranial hypertension”. Journal of Neurosurgery. 23(5): E7.
- Mcgirt MJ et Al (October 2004). “Cerebrospinal fluid shunt placement for pseudotumor cerebri—associated intractable headache: predictors of treatment response and an analysis of long-term outcomes.” Journal of Neurosurgery. 101(4): 627-632.
- Digre KB, Corbett JJ (2001). “Idiopathic intracranial hypertension (pseudotumor cerebri): A reappraisal”. Neurologist. 7: 2–67.
- Wall, M (February 2017).”Update on Idiopathic Intracranial Hypertension”. Neurologic Clinics. 35 (1): 45–57.





1 thought on “EM@3AM: Idiopathic Intracranial Hypertension”
Pingback: Idiopathic Intracranial Hypertension: a rapid review - First10EM