
Author: Rachel Bridwell, MD (@rebridwell, EM Resident Physician, SAUSHEC / San Antonio, TX) // Edited by: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 43-year-old female is brought to the ED by her husband for altered mental status, with recent worsening confusion. Review of systems is remarkable for a recent weight gain, constipation, fatigue, and skin changes. Vital signs include BP 92/60, HR 48, T 93.2 rectal, RR 13, SpO2 96% on room air. She is alert and oriented x 1, and her neck reveals a well-healed midline anterior neck scar. She is bradycardic, and her abdomen is soft but distended. Her extremities are cool, and her skin exam reveals a doughy-like sensation with palpation over her tibias.
What’s the likely diagnosis, and what are the next steps in your evaluation and treatment?
Answer: Myxedema Coma1-14
Epidemiology:
- Typically affects middle age and older women (> 60 years) with history of hypothyroidism1
- Incidence of 0.22 per million per year1
- Patients with TSH > 10 mIU/L or untreated hypothyroidism are at increased risk for HFrEF, HFpEF, bradycardia2
- Consider precipitating etiologies: Bradycardia, hypothermia, burns, CHF, CVA, GI bleed, metabolic abnormality, medications (CNS/cardiac depressants), PE, sepsis, trauma, Sheehan’s syndrome1
- Drugs to consider: amiodarone, lithium, phenytoin, Synthroid non-compliance3
- Rare induction of myxedema coma by large amounts of raw bok chow consumption4
- Two types: Primary (more common) and secondary
- Primary: Inherent thyroid problem, hypothalamus sending TSH to thyroid5
- Secondary: Failure of hypothalamus (TSH and T3 normal, elevated TRH)
- Euthyroid Sick Syndrome: Failure of peripheral conversion of T3 to T46
- Mortality between 20-60%, but if untreated, mortality reaches 100%7
Clinical Presentation:
- All systems slowed: bradycardia, hypothermia, bradypnea, hypotension, constipation, fatigue, skin and hair changes, loss of 1/3 of lateral eyebrow
- May be severely hypothermic despite infection1
- Neuro: Patients may present with hypoactive delirium
- Assess ABCs
- Hypotension—Consider D5NS in the setting of hyponatremia, though gentle balance required for fluid overload state
- Consider use of 3% saline if severely hyponatremic and fluid overloaded to correct 3-4 mEq/L8
- Bradycardia
- Hypothermia
- Bradypnea—Anatomic changes of myxedema of larynx and macroglossia may result in a challenging intubation1
- Mechanical ventilation may be required within 36-48 hours1
- Perform a complete physical examination to evaluate for underlying etiology7
- CV: Bradycardia, decreased cardiac output
- Dermatology: Pretibial myxedema, loss of lateral 1/3 of eyebrow, coarse skin, muscle hypertrophy
- Altered vascular permeability generates effusions and anasarca secondary to decreased GFR and excess ADH9
- Neuro: Hypoactive delirium, psychosis, lethargy, psychomotor retardation, “hung up” reflexes (delayed relaxation phase of reflexes)
- Myxedema madness
- Status epilepticus with 25% patients experiencing seizures secondary to hypoxia, hypoglycemia, hyponatremia1
- Myxedema madness
Laboratory and Imaging:
- CBC, CMP, TSH, T4, blood cultures, UA/UCx, CK, ECG, VBG to assess respiratory status
- Elevated TSH (usually greater than 10)
- Though severe systemic illness or treatment with inotropes or steroids can reduce TSH1
- Normal TSH seen if primary issue is pituitary e.g. Sheehan’s syndrome
- Hyponatremia and hypoglycemia common11
- Elevated CK, Cr, transaminases
- Bradycardia, AV blocks, low voltages, prolonged QT7
- Respiratory acidosis secondary to hypercapnic bradypnea7
- Hypercapnic hypoventilation generates shunting even after intubation6
- Normocytic, normochromic anemia12
- May not mount leukocytosis even in setting of infection2
- Elevated TSH (usually greater than 10)
- Consider investigating underlying etiologies precipitating event: GI bleed, MI, infection, infarction, medication non-compliance3
- Obtain chest x-ray
- Other testing may be required dependent on history and exam, including head and/or abdominal CT.
Treatment:
- ABCs—Rewarm the patient, NS repletion to target hyponatremia, consider advanced airway management
- Treat underlying etiology. Administer broad-spectrum antibiotics.
- Repletion: Give stress dose prior repletion of thyroid hormones to prevent precipitation of adrenal crisis7
- Hydrocortisone: 100mg IV q8hours3
- Levothyroxine (T4): 100-500 mcg IV T4 load, then 50 mcg qd3
- Consider lower dose in patients with CHF13
- Liothyronine (T3): 10-25 mcg IV/NGT q 8-12 hours3
- Difficult absorption if NGT in underlying gastric complications of myxedema to include ileus, constipation, gastric atony12
- T3 vs T4 administration controversial
- T4 administration increases cardiac output and can precipitate heart failure or MI, while T3 is associated with increased dysrhythmia2
- In known coronary insufficiency, improve oxygen supply prior to T4 supplementation, which increases myocardial demand14
- Consult endocrine evaluation
- Admit to MICU
- T4 administration increases cardiac output and can precipitate heart failure or MI, while T3 is associated with increased dysrhythmia2
Pearls:
- Consider and treat precipitating factors that cause myxedema
- Give stress dose steroids prior to thyroid repletion to prevent causing adrenal crisis
- Give lower dose of T4 in setting of underlying CHF or known coronary artery disease

An 87-year-old woman with a long-standing history of hypothyroidism presents to the ED with confusion and lethargy. On physical exam, you note diffuse nonpitting edema. Vital signs are BP 100/60 mm Hg, HR 44 beats per minute, RR 10 breaths per minute, and T 94.0°F. Which of the following laboratory abnormalities is often associated with this diagnosis?
A) Hyperglycemia
B) Hyperkalemia
C) Hypomagnesemia
D) Hyponatremia
Answer: D
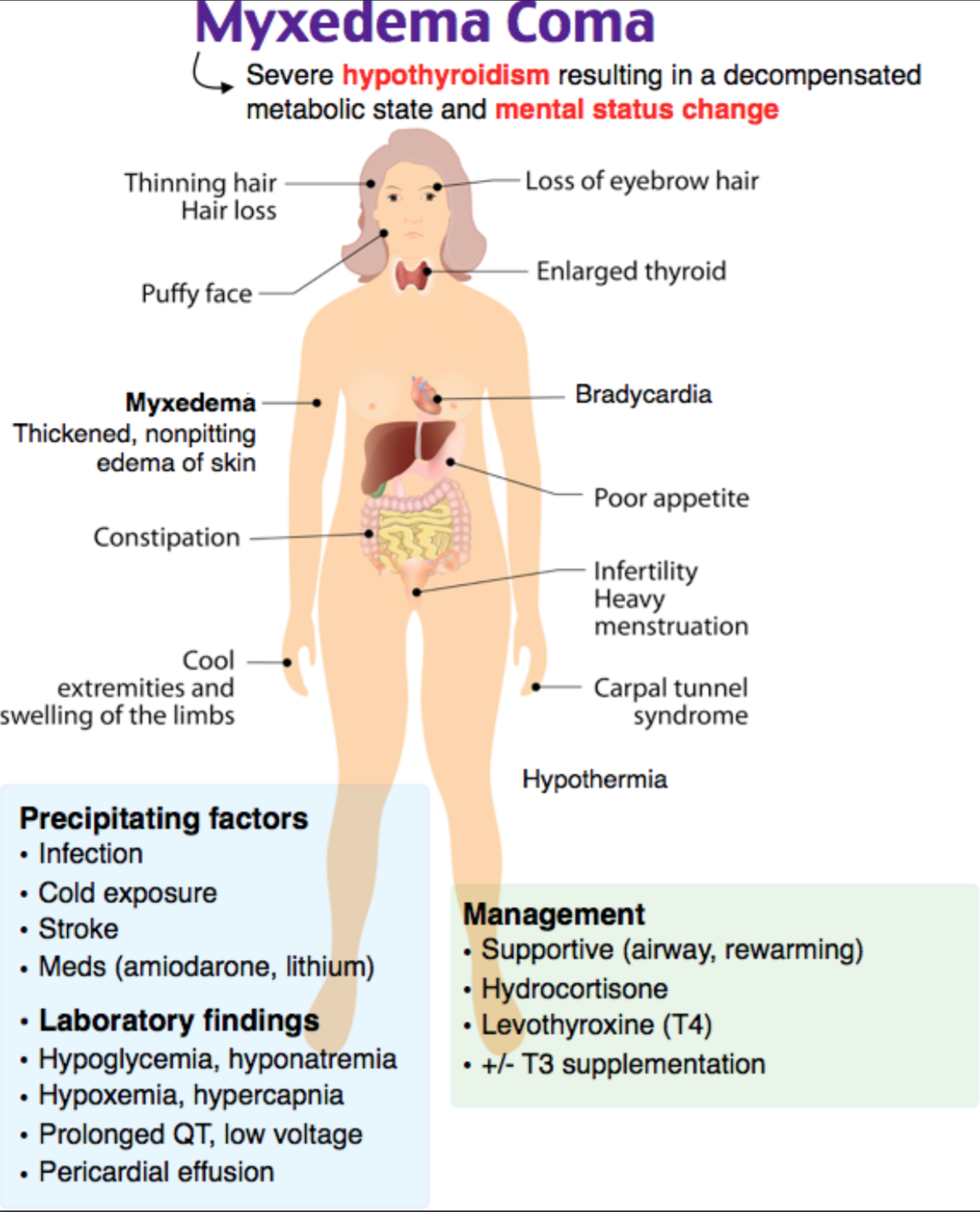
This patient is exhibiting signs and symptoms consistent with myxedema coma. Myxedema coma is defined as severe hypothyroidism resulting in a decompensated metabolic state and mental status change. It is classically characterized by thickened, nonpitting edema of the skin diffusely associated with severe chronic hypothyroidism. The diagnosis of myxedema coma is a clinical diagnosis based upon history and physical examination findings and exclusion of other causes of coma. As with other causes of hypothyroidism, the TSH is typically high while T4 and T3 are low. Other laboratory findings include hypoglycemia, hyponatremia (seen in over 50% of patients with this diagnosis), hypoxemia, and hypercapnia. ECG findings often include prolonged QT interval, low voltage, and flattened T waves. If a pericardial effusion is present, the chest radiograph may show an enlarged cardiac silhouette. Precipitating factors of myxedema coma include infection, cold exposure, stroke, or medications such as amiodarone and lithium. Mortality in myxedema coma is proportional to the severity of the patient’s hypothermia. Other signs and symptoms of myxedema coma include hypoventilation, bradycardia, poor cardiac contractility, decreased cardiac output, pericardial effusion, and altered mental status. Definitive therapy for patients with myxedema coma is with the administration of intravenous thyroxine.
Hypoglycemia, not hyperglycemia (A), is associated with myxedema coma. Neither hyperkalemia (B) nor hypomagnesemia (C) are definitively associated with myxedema coma.
Further Reading:
emDocs EM Primer





2 thoughts on “EM@3AM: Decompensated Hypothyroidism”
Pingback: May FOAMed - FRCEM Success
Pingback: Quiz 35, May 17th 2019