
Authors: Brittany Kirch, DO (EM Resident, CRDAMC); Alec Pawlukiewicz, MD (EM Attending, CRDAMC) // Reviewed By: Sophia Görgens, MD (EM Physician, Yale University, CT), Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 58-year-old male with no significant past medical history, presents to the ED for 1 day of severe vertigo associated with nausea and vomiting, tinnitus, and sudden-onset hearing loss. He reports several days of left-sided ear pain and discharge from his left ear. He has had no neck pain, headache, weakness, numbness, or vision changes. Vital signs include T 38.9C, HR 120, BP 138/96, RR 18, SpO2 99% on room air.
On exam, he is ill-appearing with an HEENT exam notable for an inflamed left external auditory canal with purulent drainage and an erythematous tympanic membrane with evidence of perforation. He has left-sided hearing loss, left-beating horizontal nystagmus, and a mildly unsteady gait. His cranial nerve exam is otherwise within normal limits, his sensation is intact to light touch, he has no focal motor weakness, and his coordination/cerebellar testing is intact.
The initial laboratory evaluation is notable for leukocytosis with bandemia. CT head shows no acute intra-cranial process.
Question: What is the most likely diagnosis?
Answer: Suppurative Labyrinthitis1-31
Etiology
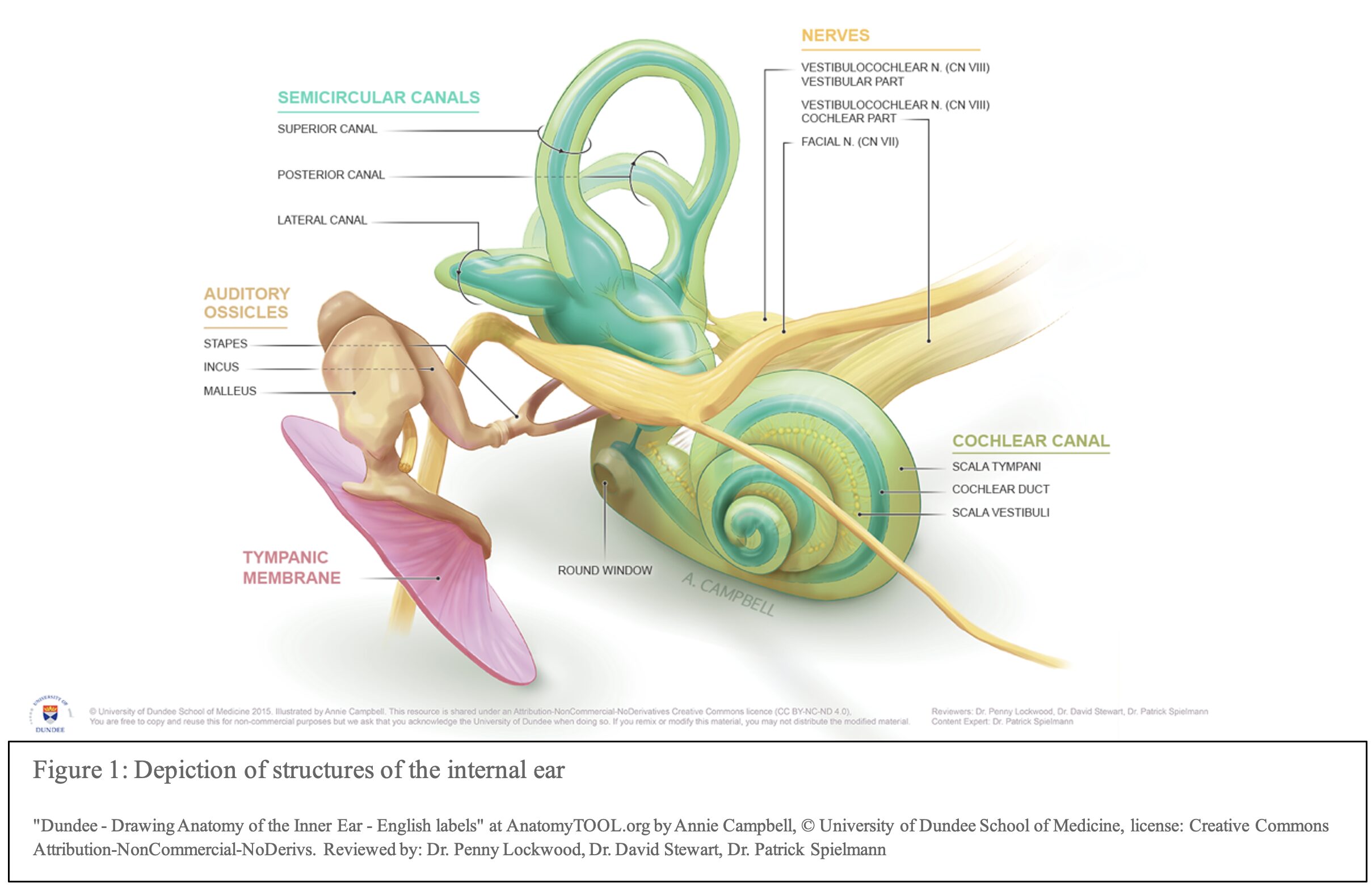
- Labyrinthitis, also known as otitis interna, is an inflammatory disorder affecting the labyrinth1
- The labyrinth is divided into two parts: the bony and membranous labyrinth2,3
- The bony labyrinth is found within the temporal bone and contains the vestibule, the cochlea, and the ampullae of the semicircular canals
- The membranous labyrinth is found within the bony labyrinth and contains the saccule, utricle, semicircular and cochlear ducts
- This organ is a part of the vestibular-auditory systems affecting both hearing and balance
- The labyrinth is divided into two parts: the bony and membranous labyrinth2,3
- Labyrinthitis is typically caused by a viral, bacterial, fungal, medication toxicity, or an autoimmune process 2–4
- May also be secondary to congenital infections such as HIV, Rubella, CMV and Syphilis3–5
- Viral Labyrinthitis can be caused by direct viral process or the post-viral inflammatory phase1,2,5
- Associated with congential infections such as Rubella, Mumps, HSV, and CMV
- Common cause of SNHL in children, especially in countries with low vaccinations rate2
- Most common cause of labyrinthitis and typically follows an upper respiratory infection1
- It is often confused with vestibular neuritis; however vestibular neuritis has no associated SNHL5
- Associated with congential infections such as Rubella, Mumps, HSV, and CMV
- Bacterial labyrinthitis can be divided into two separate subtypes 1,6
- Serous: Secondary to inflammatory mediators or endotoxins produced by a bacterial infection
- Considered a precursor to a suppurative infection1,6
- Suppurative: direct invasion of bacteria resulting in end organ damage1,3,6
- Common causative agents include Streptococcus pneumoniae and Haemophilus influenzae1
- Identification of causative agent can be difficult due to challenges in obtaining sample tissue2
- Serous: Secondary to inflammatory mediators or endotoxins produced by a bacterial infection
- Suppurative Labyrinthitis (SL) arises from 3 sources2,6,7
- Tympanogenic/ Otogenic: infection arises from the middle ear2
- Can occur from an acute or chronic otitis media (OM) 3,8
- Spreads to inner ear via the round and oval window9,10
- Tends to present with unilateral symptoms4
- Tympanogenic/ Otogenic: infection arises from the middle ear2
- Meningogenic: infection spreads from the meninges in patients with meningitis 3,4,6,9
- Spreads by direct communication between the central nervous system (CNS) and the inner ear via the cochlear aqueduct, modiolus of the cochlea, and internal auditory canal
- Typically, audio-vestibular symptoms will appear later in presentation and can be bilateral4
- Hematogenic: results from a bloodborne infection, however this mechanism is not well established9
Epidemiology
- Incidence of suppurative labyrinthitis is not well defined, and typically does not occur as an isolated infection3
- It is considered one of the more common intratemporal complications of OM, with generally low overall occurrence11–14
- One prospective cohort study found a 0.17% annual incidence of labyrinthitis as a complication of OM15
- Thought to have a decreasing prevalence due to more easily accessible antibiotic treatment and vaccinations2–4,6,10,11,13
- Higher incidence might be seen in countries with limited resources due to lack of access to antibiotic treatment and vaccinations11
- Can occur at any age, however broadly considered to have a bimodal disruption affecting primarily younger children before age of 5 and adults from 30-60 years old3,16,17
- Suppurative labyrinthitis is thought to be the cause of hearing loss in children under the age of 2 who survive bacterial meningitis3
Clinical Presentation
- Signs and symptoms can overlap with acute otitis media, chronic otitis media, and meningitis depending on the source of SL17
- Hallmark symptoms associated with SL:
- Acute Vertigo: described as severe and incapacitating3,4,12,16,18–20
- Sensorineural Hearing Loss (SNHL): Rapidly progressive, often profound. The hearing loss is the considered the most disabling aspect of SL3,4,16,18–21
- Consider Weber and Rinne testing using a tuning fork to differentiate from conductive hearing loss typically associated with OM16
- Tinnitus3,12,16,18–21
- Nystagmus: may be horizontal, vertical, or rotary3,16,20
- Nausea and vomiting typically, secondary to severe vertigo3,4,16
- If tympanogenic:
- Ear pain17
- Fever17
- Bulging, erythematous TM, or retracted TM with limited mobility17
- Otorrhea16
- Unilateral symptoms4,10,20,22
- If meningogenic:
- Meningeal signs such as nuchal rigidity, Kernig’s or Brudzinski’s sign2,17,19
- Photophobia, headache, fever 2,17
- Bilateral audio-vestibular symptoms4
- A thorough HEENT and neurologic exam should be completed as part of the physical exam
- Neurological deficits such as focal weakness, numbness, gaze palsy or visual field deficits are typically not associated with SL and are concerning for CVA as an alternate diagnosis3,16,17
- Distinguishing SL from vestibular neuritis, viral labyrinthitis, serous labyrinthitis, and idiopathic labyrinthitis1,2,17
- Vestibular neuritis is typically associated with recent and/ or concurrent viral upper respiratory infection1,5
- Symptoms typically include mild tinnitus, vertigo, and nystagmus
- Will not have any associated hearing loss
- Viral labyrinthitis and serous labyrinthitis are often described as a mild presentation of tinnitus, vertigo, nystagmus, and SNHL1,17
- Can be difficult to distinguish from SL
- Viral labyrinthitis can result in permanent SNHL, however this is more commonly seen in congenital infections1,2
- Hearing loss in serous labyrinthitis is self-limited17
- SNHL with tinnitus, nystagmus, and vertigo without any evidence of an infectious process is classified as labyrinthitis2
- Idiopathic process without a clear mechanism
- Vestibular neuritis is typically associated with recent and/ or concurrent viral upper respiratory infection1,5
Evaluation
- Laboratory testing should be tailored to the patient’s clinical presentation3,17
- There is no lab or imaging study that will definitively diagnosis SL16,17
- If patient presentation is concerning for sepsis, recommend proceeding with appropriate sepsis labs and work up
- If patients have signs and symptoms concerning meningitis, recommend preceding with Lumbar Puncture (LP)3,16
- If otorrhea is present, cultures should be obtained16
- CT head will often not show findings consistent with acute phase of suppurative labyrinthitis infection1,3,14,16,20
- May be obtained to evaluate for mastoiditis or alternative acute intracranial pathologies such as intracranial abscess or sinus thrombosis
- Sequalae of suppurative labyrinthitis might be seen if repeat CT imaging is done which can include:
- Labyrinthitis ossificans 1,2,9
- Labyrinthine aplasia 1
- Fistula12
- MR with contrast, while not always readily available in the ER, should be considered early in the work up for patients with presentation concerning for SL.
- T1 weighted image can show enhancement of the labyrinth and may help to identify labyrinthitis early in its course 1–4,10,16,17,19
Diagnosis
- Suppurative labyrinthitis is a clinical diagnosis with no definitive test available for diagnosis16,17
- Have a high index of suspicion in ill-appearing patients with:
- Vertigo with hearing loss
- Meningeal signs with hearing loss or vertigo
- Acute or chronic OM with hearing loss consistent with SNHL.
- Have a high index of suspicion in ill-appearing patients with:
Treatment
- These patients should be admitted for continued monitoring of symptoms and started on IV antibiotics1,3,13,17,22
- Recommend using antibiotics that have good CNS penetrance2,17
- Ceftriaxone: 50mg/kg (maximum 2g per dose) every 12 hours23
- Vancomycin: 20-35 mg/kg intravenous loading dose, followed by 15-20 mg/kg intravenous every 8 to 12 hours (maximum 3,000 mg per dose)24
- Vestibular suppression can be used for symptom management3,13,17
- Medications should not be used longer than 72 hours due to inhibition of vestibular compensation3
- Diazepam25
- IV, Oral
- 1 to 5 mg every 12 hours as needed for up to 48 to 72 hours
- Meclizine26
- Oral
- Initial dosing: 12.5 to 25 mg every 6 to 12 hours as needed
- May increase to 50 mg per dose as needed based on response and tolerability; maximum dose: 100 mg/day, use for MAX of 3 days
- Scopolamine27
- Apply 1 transdermal patch (1 mg/3 days) behind the ear for use up to 72 hours
- If needed for >72 hours, remove the old patch and place new one behind the other ear.
- If symptoms are not adequately controlled with use of 1 patch, may consider using 2 patches.
- Early ENT consult and involvement
- Some patients will require surgical intervention which can include myringotomy and/or mastoidectomy3,10,21
- Potential for steroid administration to preserve hearing, especially if no improvement despite adequate antibiotic treatment
- No clear guideline on the use of steroids in suppurative labyrinthitis 1,2,10,19,20,28
- Systemic dexamethasone was found to be protective against hearing loss in pediatric patients with bacterial meningitis19,29
- Dexamethasone30
- 0.15 mg/kg/dose IV up to 10 mg every 6 hours for first 2 to 4 days of antibiotic treatment
- No clear guideline on the use of steroids in suppurative labyrinthitis 1,2,10,19,20,28
Prognosis
- Typically, SNHL from suppurative labyrinthitis is permanent
- Secondary to destruction of the labyrinth or due to the development of labyrinthitis ossificans3,10,19,31
- It is unknown how frequently meningitis causes SL or SL from a tympanogenic source causes meningitis2,17
- Tinnitus can also persist after resolution of infection3
Clinical Pearls
- Consider suppurative labyrinthitis in patients with fever, acute hearing loss, and vertigo, especially if evidence of acute or chronic OM is present
- Generally, tympanogenic source of suppurative labyrinthitis will cause unilateral symptoms, and bilateralsymptoms are associated with a meningogenic source
- Focal neurologic deficits and/or findings, outside of nystagmus, vertigo, and SNHL, should raise concern for other potential acute intracranial process, such as stroke, abscess, or hemorrhage
Disclaimer: The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Carl R. Darnall Army Medical Center, Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Army, the Department of the Air Force and Department of Defense or the U.S. Government.

A 6-year-old boy presents to the emergency department with his parent for an earache and fever. A week ago, he began reporting ear pain, and he has had no relief with acetaminophen and ibuprofen. This morning, the patient began to describe room-spinning episodes and difficulty hearing out of his right ear. His vital signs include temperature 38.4°C, heart rate 126 bpm, blood pressure 100/60 mm Hg, respiratory rate 26/min, and oxygen saturation 98% on room air. The physical exam is notable for a bulging, erythematous right tympanic membrane. Neurological testing elicits near complete hearing loss in his right ear but is otherwise normal. What complication is this patient most at risk for, given the most likely diagnosis?
A) Brain abscess
B) Herpes zoster oticus
C) Ipsilateral facial paresis
D) Meningitis
Correct answer: D
This patient’s presentation is most consistent with bacterial labyrinthitis, with meningitis as its most common disease sequelae. Risk factors and clinical presentations differ between the three types of labyrinthitis. Each most commonly presents with some form of vertigo, tinnitus, orhearing loss, or a combination of these. Serous labyrinthitis is most commonly due to a preceding viral upper respiratory infection. The presenting symptoms are the mildest of the three types. Toxic labyrinthitis is due to an offending medication causing direct damage to the labyrinth. Offending medications can include aminoglycosides, salicylates, and loop diuretics. The associated symptoms are more severe than serous labyrinthitis. Treatment for serous labyrinthitis is based on the patient’s symptoms. The mainstay of treatment for toxic labyrinthitis is to remove all offending medications and provide close follow-up, though a full resolution is not assured.
In this case, the patient’s bacterial labyrinthitis is due to his acute otitis media, as noted by his bulging, erythematous right tympanic membrane and fever. Bacterial labyrinthitis has the most severe symptoms of the three types, with patients appearing the most toxic. This infection can spread via a contiguous route into the meninges. Thus, antibiotics should be started, and an otolaryngology consult called. These patients should be admitted for continued monitoring and possible surgical drainage.
Brain abscesses (A) are not as commonly associated with bacterial labyrinthitis as meningitis. While they can form due to the direct contiguous spread of an acute otitis media, this patient’s presentation is most consistent with bacterial labyrinthitis. Thus, he is most at risk for meningitis.
Herpes zoster oticus (B), or Ramsay Hunt syndrome, is a type of vestibular ganglionitis caused by the reactivation of a previously dormant varicella zoster infection. It presents as grouped vesicles on erythematous bases within the auditory canal with subsequent vertigo, deafness, and ipsilateral partial or complete facial nerve palsy. Known risk factors include previous varicella infection, immunosuppression, extremes of age, and pregnancy. Although herpes zoster can lead to symptoms of labyrinthitis, it would not be a complication of this patient’s current bacterial illness.
Ipsilateral facial paresis (C) can be a complication of many disease processes that cause vertigo, ranging from herpes zoster oticus, vestibular ganglionitis, strokes, and trauma to brain abscesses and tumors. Labyrinthitis is not associated with an increased risk of facial paresis.
Additional Reading
Further FOAMed:
- Review of mastoiditis: https://www.emdocs.net/acute-mastoiditis-pearls-and-pitfalls/
- Review of vertigo: https://www.emdocs.net/em-beats-by-doge-vertigo-central-or-peripheral/
References:
- Small JE., Noujaim DL., Ginat DThomas, Kelly HR., Schaefer PW., Brunch PM. Neuroradiology : spectrum and evolution of disease. In: Neuroradiology: Spectrum and Evolution of Disease. Elsevier; 2019:396.
- Flint PW., Goddard JC, Slattery WH. Infections of the Labyrinth. In: Cummings Otolaryngology: Head and Neck Surgery. 7th ed. Elsevier; 2021:2356-2364.
- Barkwill D, Winters R, Arora Affiliations R. Labyrinthitis Continuing Education Activity. https://www.ncbi.nlm.nih.gov/books/NBK560506/?report=printable
- Bertholon P, Karkas A. Otologic disorders causing dizziness, including surgery for vestibular disorders. In: Handbook of Clinical Neurology. Vol 137. Elsevier B.V.; 2016:279-293. doi:10.1016/B978-0-444-63437-5.00020-0
- Furman JM. Vestibular neuritis and labyrinthitis. UptoDate. October 2025. Accessed November 15, 2025. https://www.uptodate.com/contents/vestibular-neuritis-and-labyrinthitis?search=vestibular%20neuritis&source=search_result&selectedTitle=1~36&usage_type=default&display_rank=1
- Paparella MM. XLIV THE PATHOLOGY OF SUPPURATIVE LABYRINTHITIS.
- Flint PW., Arts HA, Adams ME. Sensorineural Hearing Loss in Adults. In: Cummings Otolaryngology: Heard and Neck Surgery. 7th ed. Elsevier; 2021:2311-2327.
- Khairkar M, Deshmukh P, Maity H, Deotale V. Chronic Suppurative Otitis Media: A Comprehensive Review of Epidemiology, Pathogenesis, Microbiology, and Complications. Cureus. Published online August 19, 2023. doi:10.7759/cureus.43729
- Taxak P, Ram C. Labyrinthitis and labyrinthitis ossificans-a case report and review of the literature. J Radiol Case Rep.EduRad. 2020;14(5):1-6. doi:10.3941/jrcr.v14i5.3706
- Jang CH, Park SY, Wang PC. A Case of Tympanogenic Labyrinthitis Complicated by Acute Otitis Media. Yonsei Med J. 2005;46(1):161. doi:10.3349/ymj.2005.46.1.161
- Maranhão A, Andrade J, Godofredo V, Matos R, Penido N. Epidemiology of Intratemporal Complications of Otitis Media. Int Arch Otorhinolaryngol. 2014;18(02):178-183. doi:10.1055/s-0033-1364172
- Xiao Q, Zhang Y, Lv J, Yang J, Zhang Q. Case Report: Suppurative Labyrinthitis Induced by Chronic Suppurative Otitis Media. Front Neurol. 2022;13. doi:10.3389/fneur.2022.892045
- Sharma N, Jaiswal AA, Banerjee PK, Garg AK. Complications of Chronic Suppurative Otitis Media and Their Management: A Single Institution 12 Years Experience. Indian Journal of Otolaryngology and Head and Neck Surgery. 2015;67(4):353-360. doi:10.1007/s12070-015-0836-5
- Wu JF, Jin Z, Yang JM, Liu YH, Duan ML. Extracranial and intracranial complications of otitis media: 22-year clinical experience and analysis. Acta Otolaryngol. 2012;132(3):261-265. doi:10.3109/00016489.2011.643239
- de Albuquerque Maranhão AS, de Andrade JSC, Godofredo VR, Matos RC, de Oliveira Penido N. Intratemporal complications of otitis media. Braz J Otorhinolaryngol. 2013;79(2):141-149. doi:10.5935/1808-8694.20130026
- Flint PW., Budenza CL, El-Kashlan HK. Complications of Temporal Bone Infections. In: Cummings Otolaryngology: Head and Neck Surgery. 7th ed. Elsevier; 2021:2135-2154.
- Jain MD R, Chu MD MSE. Suppurative Labyrinthitis. Sibel DO MJ, Bontempo MD L, Swadron MD S, Patrick Nordt MD PS, Mattu MD A, Johnson MD MSW, eds. Preprint posted online October 2024. https://www.emrap.org/corependium/chapter/recAwzDw3joQxcDbZ/Suppurative-Labyrinthitis
- Kaya S, Schachern PA, Tsuprun V, Paparella MM, Cureoglu S. Deterioration of Vestibular Cells in Labyrinthitis. Annals of Otology, Rhinology and Laryngology. 2017;126(2):89-95. doi:10.1177/0003489416675356
- Kopelovich JC, Germiller JA, Laury AM, Shah SS, Pollock AN. Early prediction of postmeningitic hearing loss in children using magnetic resonance imaging. Archives of Otolaryngology – Head and Neck Surgery. 2011;137(5):441-447. doi:10.1001/archoto.2011.13
- Maranhão AS de A, de Andrade JSC, Godofredo VR, Matos RC, Penido N de O. Intratemporal complications of otitis media. Braz J Otorhinolaryngol. 2013;79(2):141-149. doi:10.5935/1808-8694.20130026
- Leskinen K&, Jero J. Acute Complications of Otitis Media in Adults.
- Fooanant S, Ruckphaopunt K, Niramon N, Teotrakul S, Kanesanarak J. Extracranial and intracranial complications of suppurative otitis media. report of 102 cases. J Laryngol Otol. 1993;107(11):999-1004. doi:10.1017/S0022215100125095
- UpToDate Lexidrug. Ceftriaxone: Drug Information. Preprint posted online 2025. https://www.uptodate.com/contents/ceftriaxone-drug-information?source=auto_suggest&selectedTitle=1~4—1~4—ceft&search=ceftriaxone
- UpToDate Lexidrug. Vancomycin: Drug Information. Preprint posted online 2025. https://www.uptodate.com/contents/vancomycin-drug-information?source=auto_suggest&selectedTitle=1~1—1~4—vanco&search=vancomycin
- UpToDate Lexidrug. Diazepam: Drug Information. Preprint posted online 2025. https://www.uptodate.com/contents/diazepam-drug-information?search=dizepam&source=panel_search_result&selectedTitle=1~150&usage_type=panel&kp_tab=drug_general&display_rank=1
- UpToDate Lexidrug. Meclizine: Drug Information. Preprint posted online 2025. https://www.uptodate.com/contents/meclizine-drug-information?source=auto_suggest&selectedTitle=1~2—1~2—mecl&search=meclizine
- UpToDate Lexidrug. Scopolamine (hyoscine): Drug Information. Preprint posted online 2025. https://www.uptodate.com/contents/scopolamine-hyoscine-drug-information?search=o%09Scopolamine%20&source=panel_search_result&selectedTitle=1~69&usage_type=panel&kp_tab=drug_general&display_rank=1
- Maranhão AS de A, Godofredo VR, Penido N de O. Suppurative labyrinthitis associated with otitis media: 26 years’ experience. Braz J Otorhinolaryngol. 2016;82(1):82-87. doi:10.1016/j.bjorl.2014.12.012
- Mclntyre PB, Berkey CS, King SM, et al. Dexamethasone as Adjunctive Therapy in Bacterial Meningitis A Meta-Analysis of Randomized Clinical Trials Since 1988.
- UptoDate Lexidrug. Dexamethasone (systemic): Drug information. UpToDate.
- Kaya S, Tsuprun V, Hizli Ö, Paparella MM, Cureoglu S. Quantitative assessment of cochlear histopathologic findings in patients with suppurative labyrinthitis. In: JAMA Otolaryngology – Head and Neck Surgery. Vol 142. American Medical Association; 2016:364-369. doi:10.1001/jamaoto.2015.3803





