
Author: Lloyd Tannenbaum, MD (EM Attending Physician, APD, Geisinger Wyoming Valley, PA) // Reviewer: Brit Long, MD (@long_brit)
Hello and welcome back to ECG Pointers, a series designed to make you more confident in your ECG interpretations. This week, we feature a post from Dr. Tannenbaum’s ECG Teaching Cases, a free ECG resource. Please check it out. Without further ado, let’s look at some ECGs!
“Mom you’re being so dramatic. I can’t believe we’re here right now.”
“Quiet! You passed out! You know our family history. You need to get checked out. It could be a sign of something really bad!”
“Mom. Come on. I’m a 23-year-old man. I’m in great shape, I work out all the time, I just got dehydrated or something. I can’t believe you made me come to the ER. This is so embarrassing.”
You pull back the curtain to room 29, interrupting the conversation. “Hello there! I’m your ER doctor, what seems to be going on?” you ask.
“Doctor, thank goodness you’re here. My son passed out today. He’s in visiting from college, he’s about to graduate, summa cum laude, just by the way. First in the family to go to college. We’re so proud. Anyway, we were sitting at the breakfast table and then all of a sudden, boom! He just went out. Lasted about a minute. I called 9-1-1, but he had recovered by the time the medics arrived. They checked him out, said his vitals looked fine and then my son refused to go to the hospital with the paramedics. Told them he was fine. It took me 90 minutes of begging to convince him to get checked out by you.”
“Wow, ok! Sounds like quite the exciting morning!” you tell her. “How about you, sir, what do you remember?” you ask the patient.
“I’m sorry, doctor, we’re totally wasting your time. I just got a little dehydrated and passed out. It happens sometimes. I’ve done it before, I’m always fine. Last time really freaked out my girlfriend, but I was fine then, and I’m fine now.”
“Do you remember what happened either of those times?” you ask the patient.
“Well, I’m not really comfortable describing the first time I passed out in front of my mother, but let’s just say that we were, uh, exercising together and half way through, I passed out,” he tells you as he and his mom turn a deep shade of red.
“And today?” you ask, trying to avoid an awkward conversation.
“Today was strange. I woke up, felt fine, came downstairs for breakfast, and then mid-sentence, I went out. Not like last time at all.”
“And, Ma’am, I heard you mention something about your family history before I walked in, what were you referring to?”
“We have a strong history of heart problems. Several of my sisters have required a valve repair or a bypass. One even had a cardiac arrest from her heart going into a bad rhythm and had a defibrillator placed!”
“Does your son have a history of heart problems?”
“I don’t know. We live in a very rural town without easy access to a pediatric cardiologist. The closest one was a 3-hour drive away and we didn’t have the money to make that kind of a trip. The town doctor said that his ECG was mostly-normal so we never looked into it more. He said something about some T waves being flipped or something but it was so long ago, I don’t remember. But now that he’s passing out, I know that something is wrong”
You look over at the patient and notice that he doesn’t look good.
“Sir! Sir! Are you ok?” you ask him.
“I don’t feel very well” he tells you and then slumps over. His mom screams. You look up at the cardiac monitor and this is what you see:
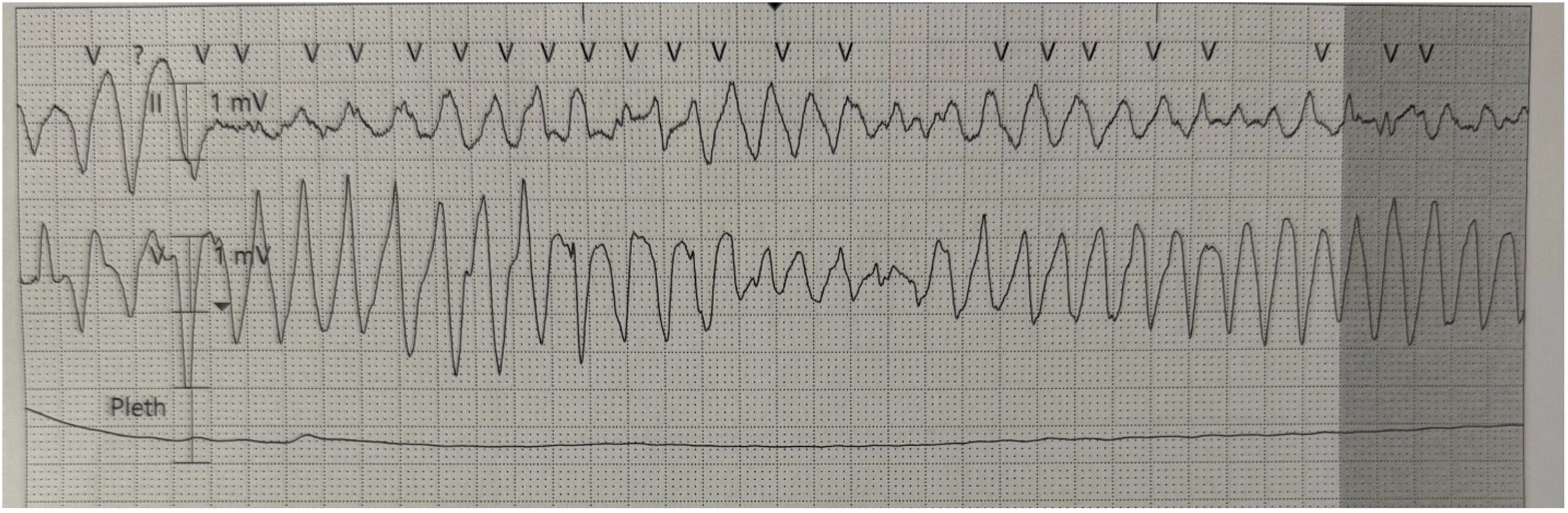
This is polymorphic ventricular tachycardia. Not a good rhythm. But what could be going on here? What “mitral valve problems” could this patient’s mom be referring to?
Interestingly, I accidentally stumbled into the controversies of mitral valve prolapse (MVP). Apparently, in the cardiology world, there is a decent sized camp of physicians who believe that MVP is arrhythmogenic and increases a patient’s (especially young patient’s) risk of sudden cardiac death. On the flip side is an equally large group of cardiologist who think that MVP is an incidental finding and poses no more of a risk of sudden cardiac death than the average population.
Since I’m neither a cardiologist, nor someone who likes to take sides in a debate like this, instead, today we’re going to look over a fascinating article from Dr. Michael Ackerman and his team from the Mayo Clinic about a malignant subtype of MVP.
This team looked at records for 1200 patients who had sudden cardiac death and identified 24 who had an “unexplained” out of hospital cardiac arrest, meaning that no cause of the arrest was found. The patients were worked up extensively and no evidence of prolonged QTc was found, normal stress tests, normal EF on Echo, etc. Believe me when I say that an extensive chart review was done and, according to the textbook, they were in perfect health, except they had and survived sudden, unexplained cardiac death.
Interestingly, of those 24 “healthy” people, 10 of them (42%) had bileaflet mitral valve prolapse identified on their post-arrest echocardiogram. 9 of those 10 (90%) patients were female! All 10 of them had some degree of mitral regurgitation due to the MVP.
Then they took a look at the ECGs of these 24 patients. The most common abnormality was age-inappropriate ST-T changes, specifically inverted or biphasic T waves in the inferior leads (II, III, and aVF). In those patients with the bileaflet MVP, 7 out of 9 of them (78%) had these T wave changes. (Note: one of the patients with bileaflet MVP was excluded from ECG analysis as that patient had a paced rhythm).
Finally, they reviewed Holter data on these patients and found that those with bileaflet MVP had a significantly higher rate of PVCs, ventricular bigeminy, and Vtach than those survivors without bileaflet MVP. Interestingly, 7 of the 10 bileaflet MVP patients, there were multiple morphologies of PVCs found. They came from the outflow tracks, papillary muscles, or fascicles. Some even came from both the left and right outflow tracks.
So, what happened next? Dr. Ackerman and the team concluded that they may have identified a potentially “malignant” MVP-ventricular arrhythmia phenotype. It’s characterized by (quoted from their paper’s conclusion): “young women with bileaflet MVP, biphasic or inverted T waves in the inferior leads, and frequent complex ventricular ectopic activity with documented ventricular bigeminy or VT as well as PVC configurations of outflow tract alternating with papillary muscle or fascicular origin.”
This paper helped to set the stage for further work on and the identification of “Arrhythmogenic Mitral Valve Prolapse Syndrome” which had a much larger study run in 2025. It included 148 patients and many of the characteristics identified today are still the same as Dr. Ackerman’s initial paper. The study can be found here. Take a look at their conclusions:
“In this international descriptive registry of patients with arrhythmogenic mitral valve prolapse syndrome and SCA, patients were young, women, and had bileaflet mitral valve prolapse, mitral annular disjunction, inferolateral T-wave inversions, and nonsustained VT. A history of syncope and anterolateral T-wave inversions was relatively common in patients who survived SCA or sustained VT/ventricular fibrillation.”
Case Wrap Up: You turn to check on the patient after noticing his concerning rhythm change. He has no pulse and you active your team while starting CPR. One of the nurses quickly brings in a defibrillator and you shock the patient, restoring sinus rhythm. He’s very confused, but talking to you and curious why everyone is standing over him yelling. You rapidly admit the patient for an extensive cardiac work up with EP following him closely.
Recap:
- There is a subset of mitral valve prolapse (MVP) that puts patients at high risk for arrhythmias and sudden cardiac death. This is now called Arrhythmogenic Mitral Valve Prolapse Syndrome.
- These patients will often have a triad of:
- Bileaflet MVP
- Inferior lead T wave inversions
- Multiple sites causing PVCs
- These patients are often young and female
- Ackerman’s initial study showed a 90% female predominance; the most recent paper I could find with 148 patients showed a 68% female predominance.
- This condition is unlikely to be diagnosed in the ED but is still worth knowing about.




