Episode 107: Eclampsia
Definition:
- Severe hypertensive disease of pregnancy (HDP) with new onset tonic-clonic, focal, or multifocal seizures or unexplained altered mental status in a patient who is pregnant or postpartum and there’s no other causative etiologies.
- Eclampsia can occur during or after the 20th week of pregnancy and up to 6 weeks postpartum.
- 60% of cases occur during the antepartum period, 20% intrapartum, and another 20% in the postpartum period. Most postpartum cases occur within the first week.
- Eclampsia may occur in patients less than 20 weeks of gestation in patients with renal disease, molar pregnancy, or multiple gestations.

- The classic understanding of HDP is this linear progression from gestational hypertension to preeclampsia to preeclampsia with severe features to eclampsia if there’s no intervention.
- This is not borne out in the literature. One study found 38% of patients who developed acute-onset eclampsia had no signs or symptoms of preeclampsia before seizures. Other studies have shown that only 1.9% and 3.2% of patients with preeclampsia and preeclampsia with severe features develop eclampsia in the absence of intervention.
Epidemiology:
- HDP account for close to 20% of maternal deaths worldwide. Preeclampsia and eclampsia are the most severe manifestations of HDP and they account for the largest proportion of deaths.
- Eclampsia occurs in around 0.3% of live births. The incidence is 1.5 to 10 cases per 10,000 deliveries.
Risk Factors:
- High-risk: Previous preeclampsia/eclampsia, multifetal gestation, renal disease, autoimmune disorder, type 1 or type 2 diabetes mellitus, chronic hypertension
- Moderate-risk: First pregnancy, maternal age >35 years, family history of preeclampsia, body mass index >30
Challenges/Issues:
- Can be a challenging diagnosis. One study found a misdiagnosis rate of 31% for OBGYN clinicians.
- Maternal mortality rate is 5-14%; condition associated with ischemic and hemorrhagic stroke, coma, heart failure, venous thrombosis, renal failure or liver damage, disseminated intravascular coagulation, and fetal demise.
- Up to 25% of mothers develop long term problems.
- Neonates can have long term issues: small for gestational age, hypoxic-ischemic brain injury, and neonatal respiratory distress syndrome.
Presentation:
- Seizures or a change in mental status are the defining symptoms; seizure are typically generalized, tonic clonic, < 1 minute. Patients are often postictal for 10-20 minutes.
- Approximately one third have no findings of preeclampsia before the seizure.
- 80% have prodromal symptom before the seizure: headache (66-82%), visual disturbances (27-44%), and upper abdominal pain (25%).
- Exam varies: 25% have normal BP, 20% have mild hypertension. Edema, clonus, and hyperreflexia may be present. The patient could be altered if they already seized or have a complication due to eclampsia.
- Key: Consider eclampsia in any pregnant and postpartum woman presenting to the ED, especially in patients with symptoms such as headache, confusion/altered mental status, vision changes, and hypertension.
ED Evaluation:
- Assessment focuses on looking for complications and mimics. Consider trauma, infection, neurologic emergency (ICH/SAH/PRES), CV and pulmonary issues, and toxic ingestion.
- Begin management while investigations underway
- POC glucose, CBC, electrolytes, RFP, LFTs, coag panel, fibrinogen, LDH, uric acid, urinalysis.
- May find thrombocytopenia, elevated creatinine, elevated aminotransferases, elevated LDH and uric acid, and proteinuria.
- Proteinuria is 55% sensitive and 84% specific for > 300mg/ 24-hour urine protein.
- Obtain ECG for dysrhythmia.
- If that patient has a new-onset seizure, focal deficit, or altered, obtain a noncontrast head CT.
- Up to 90% of patients will have findings of PRES on neuroimaging.
- If there are cardiopulmonary signs or symptoms, obtain chest x-ray.
ED management:
- Major components are preventing maternal hypoxia, stopping the seizure and preventing more seizures, treating severe hypertension if it’s present, and consulting OBGYN. If the patient is pregnant, they need emergent delivery.
- If they are pregnant, put them in the left lateral decubitus position.
- Obtain IV access and place on supplemental oxygen to prevent patient and fetal hypoxia. Be prepared for a challenging airway (edema, friable mucosa, hemodynamics).
- For seizures, the treatment of choice is magnesium. Reduces maternal mortality and decreases the risk of seizure recurrence.
- If the patient is actively seizing, give IV magnesium sulfate at a loading dose of 4-6 grams over 15 minutes, followed by maintenance infusion of 1-3 g/hr. Goal serum magnesium is 2-3.5 mmol/L (4-5 mEq/L). If no IV access, give 10 g IM magnesium (5 g in each buttock).
- Absolute contraindications for magnesium: myasthenia gravis, severe hypocalcemia, complete heart block, and myocarditis.
- Up to 10% of patients have recurrent seizure activity after the initial bolus of magnesium. If that occurs, give a second bolus of 2 g magnesium over 3-5 minutes. Next administer benzodiazepines and prepare to intubate.
- Magnesium is mostly safe, maternal toxicity is rare with monitoring. Patients do require monitoring on the magnesium infusion.
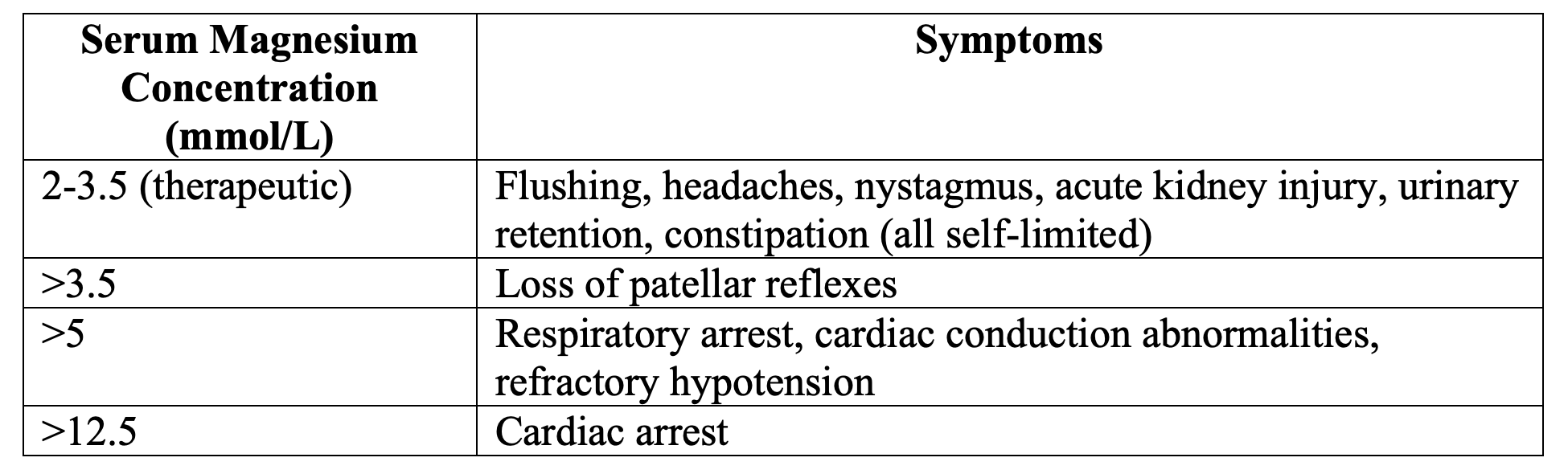
-
- The first physical exam finding of magnesium toxicity is loss of deep tendon reflexes.
- Urine output should be 100 mL/4 hours. Urinary retention and decreased production can be due to magnesium toxicity or decreased renal function (90% of magnesium is eliminated through the urine).
- If they have known renal disease, administer bolus but no infusion.
- Other than the urine output and DTS, monitor their RR, HR, BP every 30 minutes.
- If evidence of toxicity present, stop the infusion and give calcium if the patient has cardiopulmonary symptoms. Administer fluids and diuretics to enhance renal clearance. If the patient has severe renal dysfunction, hemodialysis may be necessary.
- BP management: Target is systolic blood pressure (SBP) 130-150 mm Hg and diastolic blood pressure (DBP) 80-100 mm Hg.
- Options: labetalol, nicardipine, hydralazine, and nifedipine.
- Systematic review found no difference in efficacy or safety between hydralazine and labetalol or hydralazine and calcium channel blockers. Avoid ACE inhibitors and ARBs in pregnant patients – renal issues in the fetus.

What do I do if the patient does not respond to management?
- Reconsider the diagnosis and consult neurology.
- Majority of patients will improve with the magnesium and blood pressure control, but if the patient does not improve within 10-20 minutes, consider NCSE, CNS infection, PRES, SAH/ICH.
- If still seizing despite the first and second bolus of magnesium, give benzodiazepines and antiepileptics like levetiracetam and consider ketamine/propofol for intubation.
Summary:
- Eclampsia is a severe manifestation of HDP and is defined by new onset tonic-clonic, focal, or multifocal seizures or unexplained altered mental status in a pregnant or postpartum patient in the absence of other causative etiologies.
- Eclampsia should be considered in pregnant and postpartum patients presenting to the ED, even in the absence of the classic symptoms of preeclampsia. Symptoms of preeclampsia and prodromes of eclampsia are often subtle and non-specific.
- Laboratory testing can assist, but it should not delay diagnosis and management of eclampsia.
- Treatment focuses on preventing maternal hypoxia, stopping the seizure and preventing more seizures with magnesium, treating severe hypertension if it’s present, and consulting OBGYN.
- Monitor patients on magnesium drip closely to identify early signs and symptoms of toxicity. Reduce magnesium dose in patients with renal dysfunction.
- Consider maternal medical history when selecting a blood pressure agent, as some may exacerbate underlying conditions. Do not use ACE-I or ARB medications in pregnant patients. Labetalol, hydralazine, nicardipine, and nifedipine may be used.
- For patients who do not improve with seizure control and blood pressure management and display continued altered mental status or seizure, non-convulsive status epilepticus, central nervous infection, PRES, and other intracranial pathologies should be considered. In these patients, neurologic consultation and neuroimaging are recommended.
References:
- Boushra M, Natesan SM, Koyfman A, Long B. High risk and low prevalence diseases: Eclampsia. Am J Emerg Med. 2022 Aug;58:223-228.
- Fishel Bartal M, Sibai BM. Eclampsia in the 21st century. American journal of obstetrics and gynecology. 2022;226(2S):S1237-S1253.
- Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222. Obstetrics and gynecology. 2020;135(6):e237-e260.
- Wilkerson RG, Ogunbodede AC. Hypertensive Disorders of Pregnancy. Emergency medicine clinics of North America. 2019;37(2):301-316.
- Shimkhada R, Solon O, Tamondong-Lachica D, Peabody JW. Misdiagnosis of obstetrical cases and the clinical and cost consequences to patients: a cross-sectional study of urban providers in the Philippines. Global Health Action. 2016;9(1).
- Brewer J, Owens MY, Wallace K, et al. Posterior reversible encephalopathy syndrome in 46 of 47 patients with eclampsia. American journal of obstetrics and gynecology. 2013;208(6):468.e1-468.e6.
- Duley L, Meher S, Jones L. Drugs for treatment of very high blood pressure during pregnancy. The Cochrane database of systematic reviews. 2013;2013(7).




