Episode 137: Acute Mastoiditis
What is mastoiditis?
- Inflammatory, suppurative infection involving the mastoid air cells complicating otitis media (Bridwell, Pang, Cassano, Kynion).
- Categorized based on time course, involved regions, and bony septae destruction.
- Acute: symptoms < 1 month.
- Acute mastoiditis with periostitis: purulent material in the mastoid cavities with no bony septae destruction.
- Coalescent mastoiditis includes destruction of the bony septae.
- Subacute: persistent infection with destruction of the bony septae; most commonly occurs in otitis media with an effusion or recurrent otitis media without antibiotics (Kynion, Holt).
- Chronic: ongoing infection present for months to years.
How often does this happen?
- Prior to development of antibiotics, mastoiditis developed in 20% of otitis media cases.
- Less common now: incidence ranges between 2-12 per 100,000 population (Bridwell, Thompson, Marom, King, Thorne, Anthonsen).
- Most common age affected ranges between 2-7 years, but can affect any age.
- Prognosis is favorable if there are no extracranial or intracranial complications (Pang, Kynion, Glynn).
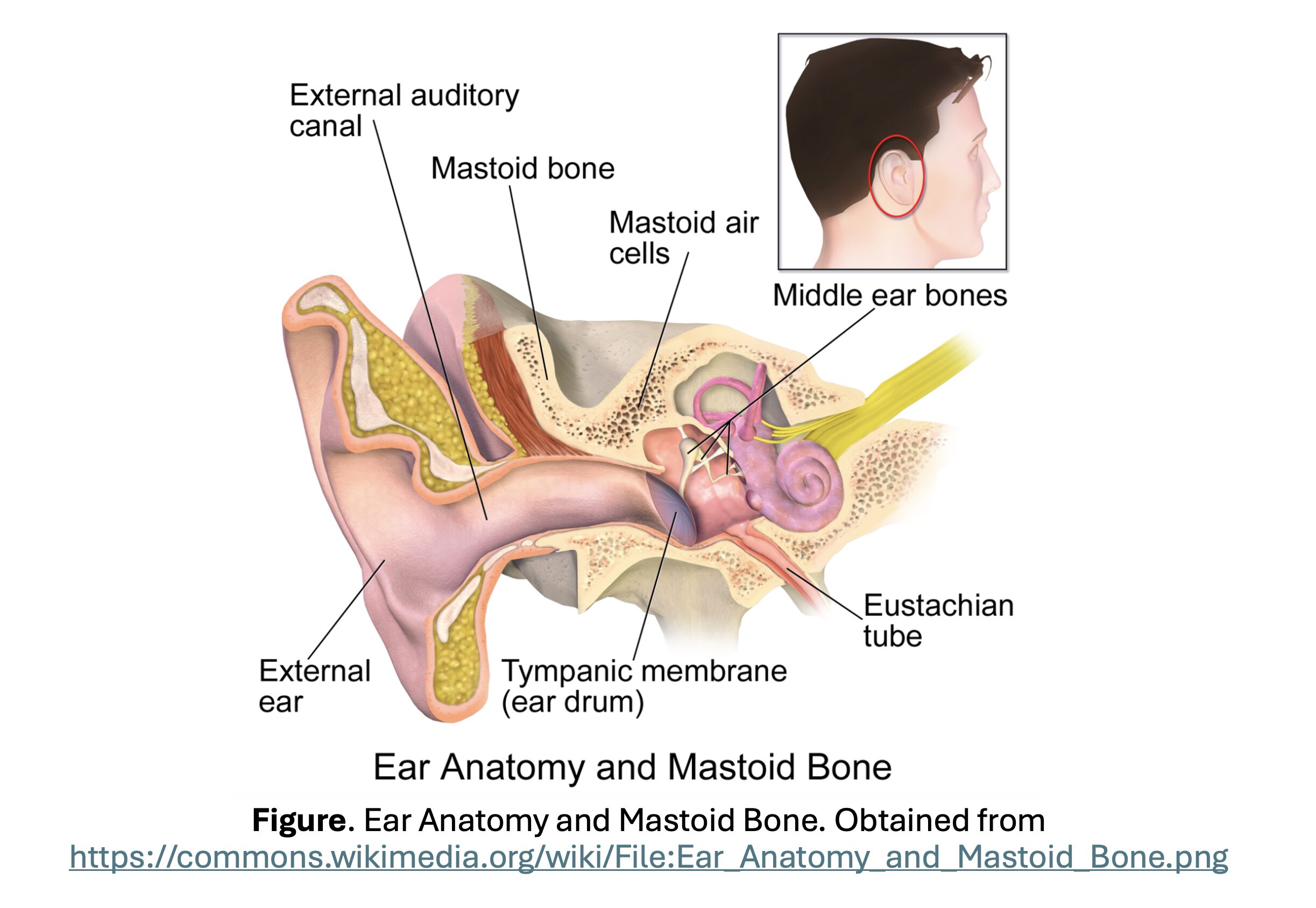
How does mastoiditis develop?
- Mastoid is part of the temporal bone, surrounded by the posterior and middle cranial fossa, facial nerve canal, sigmoid and lateral sinuses, and temporal bone petrous tip (Bridwell, Pang, Kynion, Glynn).
- At birth mastoid is a single cell (antrum) connected by a narrow channel to the middle ear.
- As the child grows older, interconnected air cells develop with pneumatization of the mastoid bone. The mastoid air spaces are continuous with the middle ear cavity.
- Acute otitis media causes inflammation of the mucosa lining the middle ear and often the mastoid.
- In most, inflammation resolves with resolution of otitis media. If inflammation does not improve, purulent material accumulates in the mastoid cavities, leading to acute mastoiditis with periostitis and bony necrosis.
- If the pressure continues to increase, bony septae between mastoid air cells are destroyed; causes coalescent mastoiditis.
- Abscess may develop, with infection spreading to other areas. Mastoid is anatomically near several important structures: semicircular canals, jugular vein, internal carotid artery, facial nerve, sigmoid sinus, brain, and meninges.
- Leads to other complications: subperiosteal abscess, Bezold abscess (deep neck abscess), petrositis, osteomyelitis of the calvaria, suppurative labyrinthitis, meningitis, venous sinus thrombosis, or intracerebral abscess may occur.
What are the most common bacteria?
- pneumoniae and Strep. pyogenes are most common causes.
- Others: Staphylococcus aureus, Fusobacterium necrophorum, Haemophilus influenzae, Moraxella catarrhalis, and Pseudomonas aeruginosa (Kaplan 2000, Gorphe, Brook).
- Multidrug resistant pneumoniae becoming a more frequent cause.
- Methicillin-resistant aureus has also remerged as a causative microbe; accounts for 20% of cases in one study (Brook, Kaplan 2015, Amir).
- Pseudomonas more common in diabetics, recent antibiotic use or recurrent otitis media, and perforation of tympanic membrane (Chien).
- Fusobacterium necrophorum more common in patients who fail oral antibiotics for otitis media and those with significantly elevated inflammatory markers (Ulanovski).
What are high-yield risk factors for mastoiditis?
- Greatest risk factor for mastoiditis is age; disease primarily affects the pediatric age group due to anatomical and immunological factors (Pang, Bridwell, Kynion).
- Tends to occur in those < 6 years (particularly 2-3 years). Immune system is more immature. Peds patients can develop rapid disease progression and more complications.
- Pediatric mastoid bone and air cells have thin trabeculae with increased pneumatization and a smaller passage connecting the mastoid antrum to the middle ear; increases risk of infection of both the fluid within the airspace and the bone.
- Proximal infections are risk factor in mastoiditis.
- Patients often have multiple incidents of otitis media prior to mastoiditis (up to 48%) (Spremo, Spratley).
What history and examination findings suggest the disease?
- Spectrum of signs/symptoms: ranges from few symptoms to life-threatening complications.
- Most common signs/symptoms: ear pain; protrusion of the auricle; and postauricular/mastoid tenderness with palpation, redness, fluctuance, or swelling.
- Systemic symptoms (fever, irritability, poor feeding, and malaise) are common (Bridwell, Pang).
- Red, inflamed, bulging tympanic membrane with a middle ear effusion, otorrhea may be present (van den Aardweg).
- Subacute mastoiditis: ear pain, cough, and fever over days to weeks. More commonly presents with complication (extracranial or intracranial) without evidence of acute otitis media as compared acute mastoiditis (Bridwell).
What does the literature say for findings? How reliable is mastoid tenderness and swelling?
- Several studies available evaluating history and exam.
- 2008 meta-analysis (65 studies; over 2100 patients) (van den Aardweg):
- 40% of patients had prior history of otitis media (2-8 weeks prior to diagnosis); 50% received dose of antibiotics prior to development of mastoiditis.
- Most common clinical finding in pediatric patients: lethargy or malaise (96%); then abnormal TM (82%), postauricular erythema or tenderness and/or pinna protrusion (80%), fever (76%), external auditory canal narrowing (71%), otalgia (67%), and otorrhea (50%). Hearing loss may also occur.
- Exam most commonly revealed TM abnormalities; 80% had otitis media with mastoiditis at the time of presentation. 79-85% of patients with mastoiditis had postauricular findings, displacement of the auricle, and acute otitis media.
- 2023 retrospective study found otalgia (OR 5.01, 95% CI 1.52-16.51), auricle protrusion (OR 8.42, 95% CI 1.37-51.64), and mastoid hyperemia (OR 4.07, 95% CI 1.09-15.23) were associated (Bertolaso).
- 2008 meta-analysis (65 studies; over 2100 patients) (van den Aardweg):
- Protrusion of the auricle is down and out in < 2 years and up and out in > 2 years.
- Postauricular lymphadenopathy may cause swelling in the postauricular area.
- Subperiosteal abscess will obliterate the postauricular skin crease and displace the auricle laterally (van den Aardweg).
- Persistent fever despite treatment with antibiotics for otitis media is suggestive of mastoiditis (van den Aardweg).
- Perform neuro exam: complications can involve the cranial nerves (VI, VII, ophthalmic branch of the trigeminal branch).
- Involvement of cranial nerve VI -> abducens nerve palsy; involvement of cranial nerve VII -> facial palsy; involvement of the ophthalmic branch of the trigeminal pain -> severe pain (Pang, Bridwell, Kynion).
- Neuro exam is challenging in kids: observe them interact with parents, watch them smile and use facial muscles, speak to them while the parent/guardian alternates covering their ears, watch them ambulate/crawl and move their extremities, and have them track someone across the room.
Is laboratory testing helpful?
- Labs cannot exclude the diagnosis. WBC and inflammatory markers are often elevated but not specific.
- Blood cultures positive in less than 6% of patients, but obtain in patients who are toxic-appearing (Kynion).
- Highest yield laboratory testing: specimen from the middle ear obtained by tympanocentesis or myringotomy (obtained by ENT; not in the ED) (Garcia, Nussinovitch).
- Sample should not be obtained from the external ear (often contaminated with aeruginosa, S. aureus).
- Sent for Gram stain, bacterial cultures, antimicrobial susceptibility testing.
When should we get imaging, and what is the test we should get?
- Imaging not absolutely necessary if history and exam consistent with the diagnosis and there is no evidence of complications.
- However, imaging can confirm the diagnosis and determine stage of infection.
- Obtain imaging in toxic-appearing patients, acute otitis media that fails to respond to therapy, and evidence of extracranial or intracranial complications (Pang, Kynion, Bridwell).
- Findings suggestive of extracranial complications: postauricular mass, cranial nerve deficits, neck mass, hearing loss, vertigo, tinnitus, retroorbital pain.
- Findings suggestive of intracranial complications: focal neurologic deficits, altered mental status, meningismus (Pang, Kynion, Bridwell).
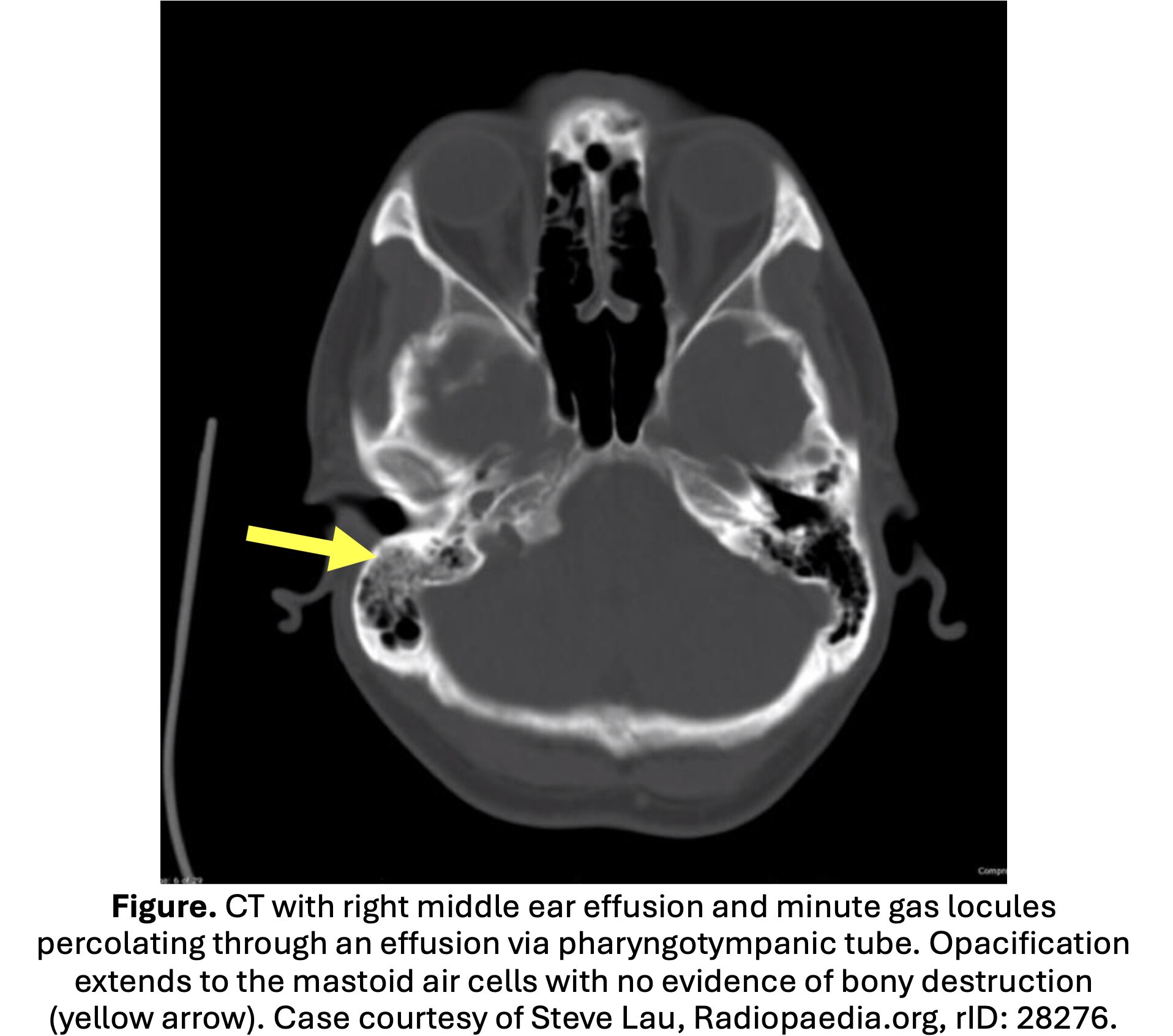
- CT temporal bones with IV contrast modality of choice; sensitivity 87-100% (Antonelli, Bridwell, Vazquez).
- Often demonstrates mastoid opacification or clouding; fluid and mastoid thickening in the mastoid and middle ear is nonspecific and common in pediatric otitis media.
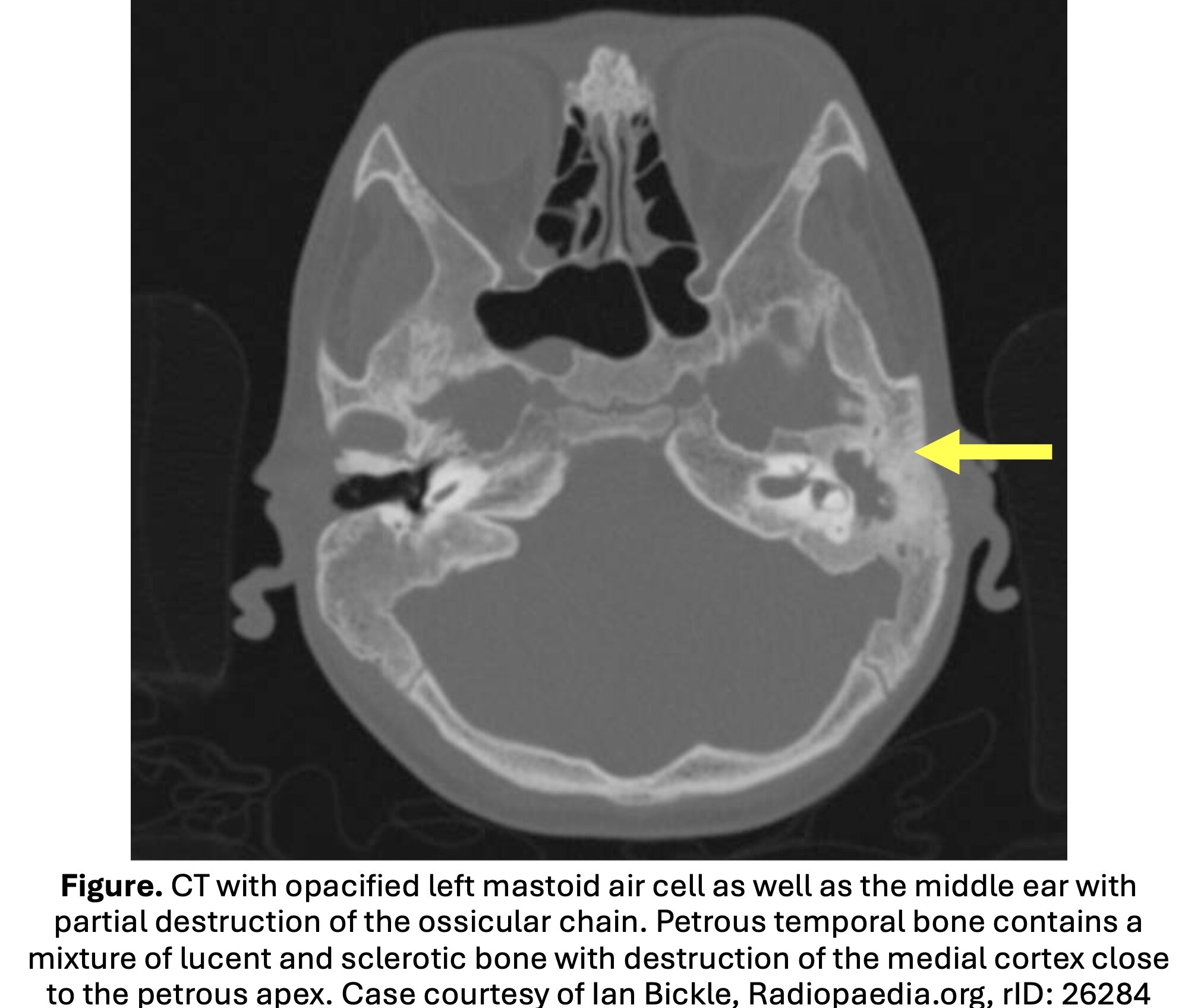
- Diagnostic findings: destruction of the mastoid cortex, periosteal thickening or disruption, and subperiosteal abscess.
- Coalescent mastoiditis: loss of definition in the bony septae defining the mastoid air cells.
- Concern for complication: CT head/temporal warranted in those with complications.
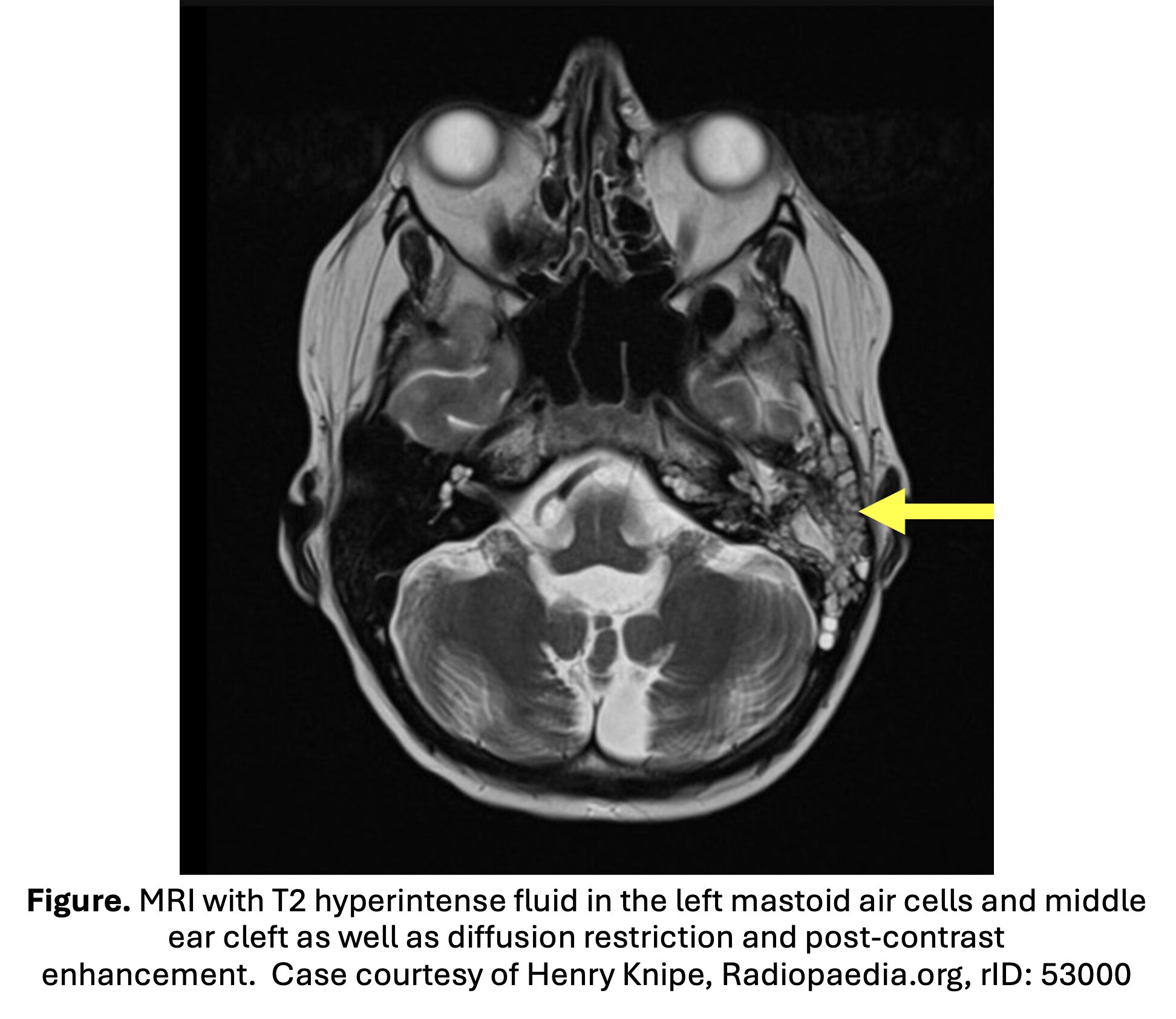
- Second line imaging modality: MRI with gadolinium contrast.
- Higher sensitivity for extra-axial fluid collections compared to CT; can evaluate intracranial structures and vascular complications (Vazquez).
- MRI may be pursued if concern for intracranial or vascular complication, IV contrast allergy, or in pediatric patients to avoid radiation exposure if MRI available.
What should be considered for management?
- Based on stage of the disease and complications.
- Consult ENT for confirmed mastoiditis for drainage of mastoid/middle ear (Loh, Psaraommatis, Kaufmann, Bridwell). May require transfer to a center with ENT for evaluation and surgical treatment.
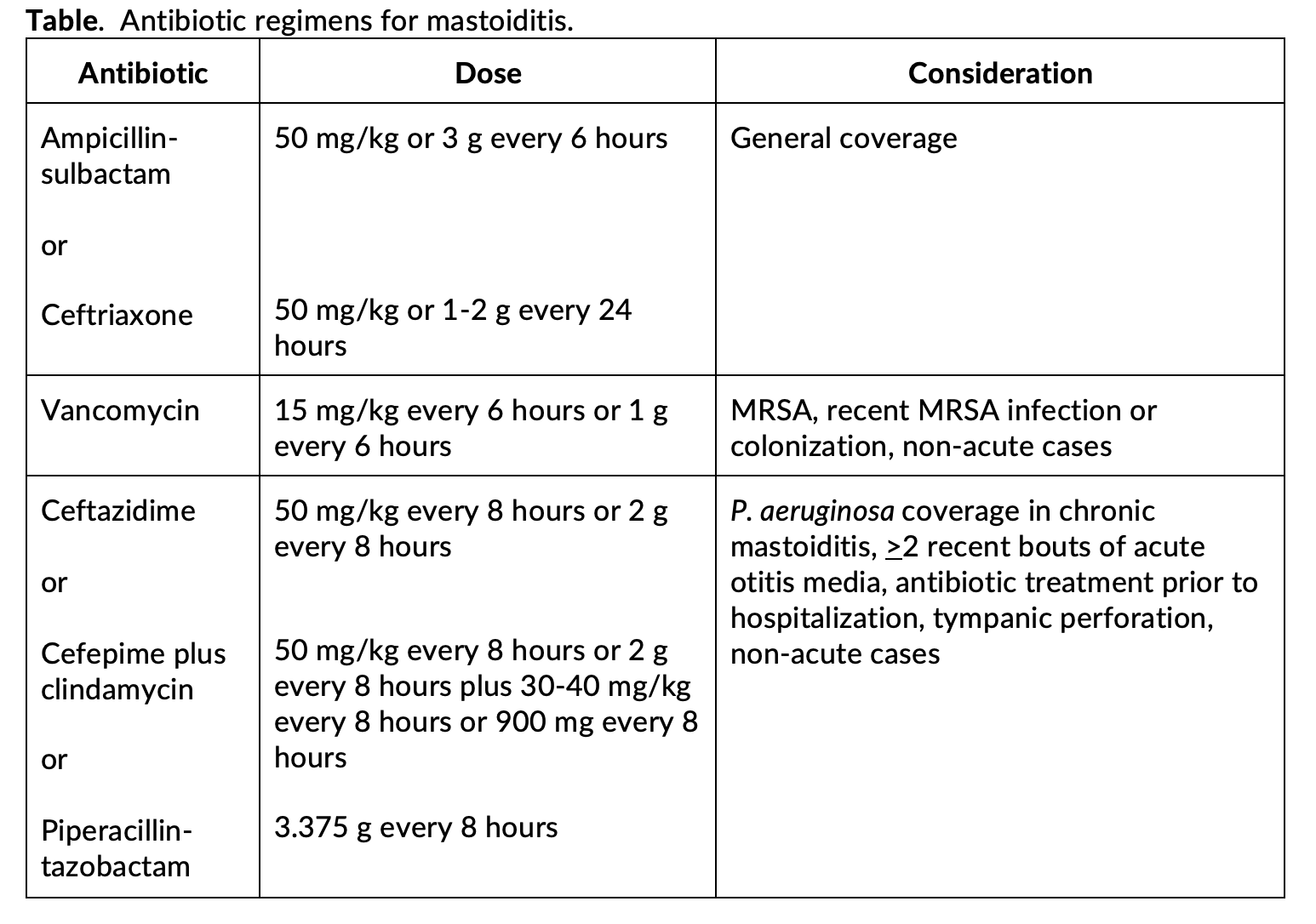
- ED management: IV antibiotics; first line options ampicillin-sulbactam or ceftriaxone.
- P. aeruginosa coverage recommended for recurrent otitis media, tympanic perforation, subacute presentation, or antibiotic administration prior to ED presentation. May include piperacillin-tazobactam, cefepime, or ceftazidime for P. aeruginosa coverage with considerations of vancomycin for MRSA coverage (Brook, Amir, Chien, Luntz, Ho).
- Admit uncomplicated mastoiditis for IV antibiotics and myringotomy for middle ear drainage.
- If patients do not improve within 48 hours, ENT may perform mastoidectomy (Bridwell, Kynion, Loh, Psarommatis, Kaufmann).
- Surgical management required in over half of patients; may be associated with improved cure rates but also higher complication rates. Much of this is decided by ENT specialist.
- In pediatric cohort of 2170 patients, 1248 (57.5%) required surgical management (Friesen). Over half received a myringotomy with or without tube insertion, 15.5% received a mastoidectomy, and 6.9% underwent a periosteal abscess drainage.
- Coalescing mastoiditis typically receive a mastoidectomy; non-coalescing mastoiditis IV antibiotic therapy first; if failed treatment then myringotomy ventilation tube (Spremo).
- 2019 systematic review found cure rate of 72% for medical treatment, while myringotomy with or without tube ventilation resulted in higher cure rates as high as 99.7% (Anne).
- 2022 Cochrane review found that mastoiditis managed surgically had decreased rates of complications compared to those managed with antibiotics alone, but surgical patients incurred higher rates of intra and extracranial abscesses (Kaufmann).
- Suppurative complications (subperiosteal abscess, Bezold abscess, osteomyelitis of other skull parts, meningitis, intracranial abscess, suppurative labyrinthitis) or coalescent mastoiditis treated with mastoidectomy along with other measures (depending on the specific complications) (Bridwell, Kynion, Loh, Psarommatis, Kaufmann).
- Subperiosteal abscess requires incision and drainage in addition to myringotomy (Anne).
- Intracranial complications require neurosurgical specialist consultation.
What complications can occur?
- Mastoiditis associated with serious complications due to location of infection; complications more common in patients < 2 years. aureus also increases risk of complications.
- Extracranial complications: subperiosteal abscess (most common complication), Bezold abscess (deep neck abscess), mastoid bony wall destruction, venous sinus thrombosis, labyrinthitis, petrous apicitis, cranial nerve palsies.
- Intracranial complications (4-16%): epidural and subdural abscesses, meningitis, encephalitis (Go, Spiegel).
Summary:
- Mastoiditis is a suppurative infection of the mastoid air cells, usually associated with acute otitis media in pediatric patients.
- Most common bacteria causing mastoiditis include pneumoniae and S. pyogenes; MRSA and P. aeruginosa have increased in incidence.
- Around half have a preceding episode of otitis media.
- History and exam: tympanic membrane erythema, pinna protrusion, postauricular/mastoid erythema and tenderness, external canal swelling, and otorrhea in addition to systemic symptoms such as fatigue and malaise.
- Labs not specific; CT with IV contrast for complications, toxic-appearing, failed abx therpay.
- Treatment includes ENT consultation and IV antibiotics.
- Complications include subperiosteal and intracranial abscess, facial nerve palsy, meningitis, venous sinus thrombosis, Bezold abscess, and seizures.
References:
- Bridwell RE, Koyfman A, Long B. High risk and low prevalence diseases: Acute mastoiditis. Am J Emerg Med. 2024 May;79:63-69. doi: 10.1016/j.ajem.2024.02.009. Epub 2024 Feb 7. PMID: 38368849.
- Pang LHY, Barakate MS, Havas TE. Mastoiditis in a paediatric population: a review of 11 years experience in management. Int J Pediatr Otorhinolaryngol. 2009;73(11):1520-1524. doi:10.1016/J.IJPORL.2009.07.003
- Cassano P, Ciprandi G, Passali D. Acute mastoiditis in children. Acta Biomed. 2020;91(1-S):54-59. doi:10.23750/ABM.V91I1-S.9259
- Kynion R. Mastoiditis. Pediatr Rev. 2018;39(5):267-269.
- Holt GR, Gates GA. Masked mastoiditis. Laryngoscope. 1983;93(8):1034-1037. doi:10.1288/00005537-198308000-00011
- Thompson PL, Gilbert RE, Long PF, Saxena S, Sharland M, Wong ICK. Effect of antibiotics for otitis media on mastoiditis in children: a retrospective cohort study using the United kingdom general practice research database. Pediatrics. 2009;123(2):424-430. doi:10.1542/PEDS.2007-3349
- Marom T, Tan A, Wilkinson GS, Pierson KS, Freeman JL, Chonmaitree T. Trends in otitis media-related health care use in the United States, 2001-2011. JAMA Pediatr. 2014;168(1):68-75. doi:10.1001/JAMAPEDIATRICS.2013.3924
- King LM, Bartoces M, Hersh AL, Hicks LA, Fleming-Dutra KE. National incidence of pediatric mastoiditis in the United States, 2000-2012: creating a baseline for public health surveillance. Pediatr Infect Dis J. 2019;38(1):e14. doi:10.1097/INF.0000000000002049
- Thorne MC, Chewaproug L, Elden LM. Suppurative complications of acute otitis media: changes in frequency over time. Arch Otolaryngol Head Neck Surg. 2009;135(7):638-641. doi:10.1001/ARCHOTO.2009.75
- Anthonsen K, Hostmark K, Hansen S, et al. Acute mastoiditis in children: a 10-year retrospective and validated multicenter study. Pediatr Infect Dis J. 2013;32(5):436-440. doi:10.1097/INF.0B013E31828ABD13
- Glynn F, Osman L, Colreavy M, Rowley H, Dwyer TPO, Blayney A. Acute mastoiditis in children: presentation and long term consequences. J Laryngol Otol. 2008;122(3):233-237. doi:10.1017/S0022215107009929
- Kaplan SL, Mason EO, Wald ER, et al. Pneumococcal mastoiditis in children. Pediatrics. 2000;106(4):695-699. doi:10.1542/PEDS.106.4.695
- Gorphe P, De Barros A, Choussy O, Dehesdin D, Marie JP. Acute mastoiditis in children: 10 years experience in a French tertiary university referral center. Eur Arch Otorhinolaryngol. 2012;269(2):455-460. doi:10.1007/S00405-011-1667-Y
- Brook I. Role of methicillin-resistant Staphylococcus aureus in head and neck infections. J Laryngol Otol. 2009;123(12):1301-1307. doi:10.1017/S0022215109990624
- Kaplan SL, Center KJ, Barson WJ, et al. Multicenter surveillance of Streptococcus pneumoniae isolates from middle ear and mastoid cultures in the 13-valent pneumococcal conjugate vaccine era. Clin Infect Dis. 2015;60(9):1339-1345. doi:10.1093/CID/CIV067
- Amir AZ, Pomp R, Amir J. Changes in acute mastoiditis in a single pediatric tertiary medical center: our experience during 2008-2009 compared with data for 1983-2007. Scand J Infect Dis. 2014;46(1):9-13. doi:10.3109/00365548.2013.849814
- Chien JH, Chen YS, Hung IF, Hsieh KS, Wu KS, Cheng MF. Mastoiditis diagnosed by clinical symptoms and imaging studies in children: disease spectrum and evolving diagnostic challenges. J Microbiol Immunol Infect. 2012;45(5):377-381. doi:10.1016/J.JMII.2011.12.008
- Ulanovski D, Shavit SS, Scheuerman O, Sokolov M, Hilly O, Raveh E. Medical and surgical characteristics of fusobacterium necrophorum mastoiditis in children. Int J Pediatr Otorhinolaryngol. 2020;138. doi:10.1016/J.IJPORL.2020.110324
- Spremo S, Udovcić B. Acute mastoiditis in children: susceptibility factors and management. Bosn J basic Med Sci. 2007;7(2):127-131. doi:10.17305/BJBMS.2007.3066
- Spratley J, Silveira H, Alvarez I, Pais-Clemente M. Acute mastoiditis in children: review of the current status. Int J Pediatr Otorhinolaryngol. 2000;56(1):33-40. doi:10.1016/S0165-5876(00)00406-7
- van den Aardweg MT, Rovers MM, de Ru JA, Albers FW, Schilder AG. A systematic review of diagnostic criteria for acute mastoiditis in children. Otol Neurotol. 2008 Sep;29(6):751-7. doi: 10.1097/MAO.0b013e31817f736b. PMID: 18617870.
- Bertolaso C, Cammisa I, Orsini N, et al. Diagnosing acute mastoiditis in a Pediatric Emergency Department: a retrospective review. Acta Biomed. 2023;94(2). doi:10.23750/ABM.V94I2.13839
- Garcia C, Salgueiro AB, Luís C, Correia P, Brito MJ. Acute mastoiditis in children: Middle ear cultures may help in reducing use of broad spectrum antibiotics. Int J Pediatr Otorhinolaryngol. 2017;92:32-37. doi:10.1016/J.IJPORL.2016.11.002
- Nussinovitch M, Yoeli R, Elishkevitz K, Varsano I. Acute mastoiditis in children: epidemiologic, clinical, microbiologic, and therapeutic aspects over past years. Clin Pediatr (Phila). 2004;43(3):261-267. doi:10.1177/000992280404300307
- Antonelli PJ, Dhanani N, Giannoni CM, Kubilis PS. Impact of resistant pneumococcus on rates of acute mastoiditis. Otolaryngol Head Neck Surg. 1999;121(3):190-194. doi:10.1016/S0194-5998(99)70170-1
- Vazquez E, Castellote A, Piqueras J, et al. Imaging of complications of acute mastoiditis in children. Radiographics. 2003;23(2):359-372. doi:10.1148/RG.232025076
- Loh R, Phua M, Shaw C-KL. Management of paediatric acute mastoiditis: systematic review. J Laryngol Otol. 2018;132(2):96-104. doi:10.1017/S0022215117001840
- Psarommatis IM, Voudouris C, Douros K, Giannakopoulos P, Bairamis T, Carabinos C. Algorithmic management of pediatric acute mastoiditis. Int J Pediatr Otorhinolaryngol. 2012;76(6):791-796. doi:10.1016/J.IJPORL.2012.02.042
- Kaufmann MR, Shetty K, Camilon PR, Shetty A, Levi JR, Devaiah AK. Management of Acute Complicated Mastoiditis: A Systematic Review and Meta-analysis. Pediatr Infect Dis J. 2022;41(4):297-301. doi:10.1097/INF.0000000000003452
- Luntz M, Brodsky A, Nusem S, et al. Acute mastoiditis — the antibiotic era: a multicenter study. Int J Pediatr Otorhinolaryngol. 2001;57(1):1-9. doi:10.1016/S0165-5876(00)00425-0
- Ho D, Rotenberg BW, Berkowitz RG. The relationship between acute mastoiditis and antibiotic use for acute otitis media in children. Arch Otolaryngol Head Neck Surg. 2008;134(1):45-48. doi:10.1001/ARCHOTOL.134.1.45
- Friesen TL, Hall M, Ramchandar N, Berry JG, Jiang W. Evolving Management of Acute Mastoiditis: Analysis of the Pediatric Health Information System Database. Otolaryngol Head Neck Surg. 2023;169(2):382-389. doi:10.1002/OHN.286
- Anne S, Schwartz S, Ishman SL, Cohen M, Hopkins B. Medical Versus Surgical Treatment of Pediatric Acute Mastoiditis: A Systematic Review. Laryngoscope. 2019;129(3):754-760. doi:10.1002/LARY.27462
- Go C, Bernstein JM, De Jong AL, Sulek M, Friedman EM. Intracranial complications of acute mastoiditis. Int J Pediatr Otorhinolaryngol. 2000;52(2):143-148. doi:10.1016/S0165-5876(00)00283-4
- Spiegel JH, Lustig LR, Lee KC, Murr AH, Schindler RA. Contemporary presentation and management of a spectrum of mastoid abscesses. Laryngoscope. 1998;108(6):822-828. doi:10.1097/00005537-199806000-00009





