Today on the emDOCs cast with Brit Long, MD (@long_brit) and Tim Montrief, MD (@EMinMiami), we cover ovarian hyperstimulation syndrome (OHSS).

Background:
– Ovarian hyperstimulation syndrome (OHSS) is associated with hyperstimulation of the ovaries due to fertility therapy and assisted reproductive technology (ART). It may also occur due to a mutation in the FSH receptor.
– ART includes any procedure with fertility medications, artificial insemination, surrogacy, and in vitro fertilization.
– Pregnancies with ART have higher rates of complications.
– Most patients are under the age of 35 years.
– Rates of ART have doubled in the past decade and now account for up to 2% of all pregnancies.
-IVF Cycle: 1) Controlled ovarian hyperstimulation with exogenous gonadotropins, 2) Follicle aspiration (i.e., oocyte retrieval), 3) Fertilization/insemination of the retrieved oocyte with spermatozoa, and 4) Embryo transfer. Most complications occur in the first step.
-OHSS affects up to 30% of all stimulation cycles. The mild form is most common. Moderate and severe account for up to 10% of cases.
Pathophysiology
– OHSS leads to capillary leakage and third spacing of fluid.
– Release of vasoactive factors like VEGF and cytokines. Leads to uterine/ovarian enlargement, increased vascular permeability, vasodilation.
– Edema, third spacing, and dehydration.
– Increased risk of thrombosis, infection.

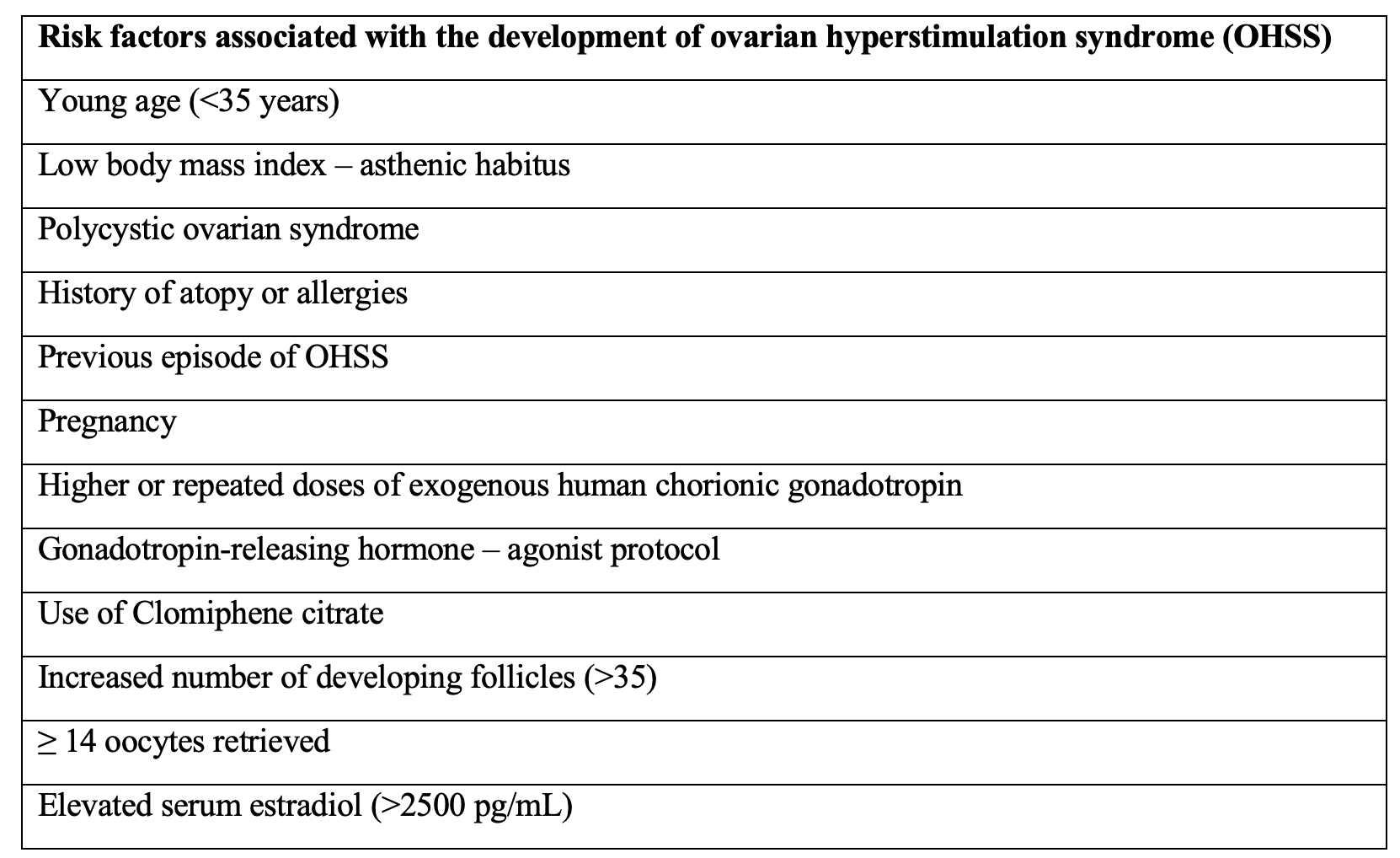
Risk factors:
– Prior OHSS, polycystic ovarian syndrome (OR 6.8), increased number of oocytes received.
History and Examination
– Early OHSS occurs 4-7 days after exogenous hCG administration and is mild to moderate. Late occurs after this period with more severe presentation.
– Ask about history of PCOS, the date of initial ART therapy, medication used for trigger (hCG or GnRH agonist), number of follicles on final monitoring scan, current therapy day, number of eggs collected, whether or not embryos were replaced and if so, how many.
– Carefully scrutinize vital signs. Fever occurs in over 80% and tachypnea in close to 100% of those with severe OHSS. Ask about current weight, changes, and abdominal girth.
– Evaluate for third spacing and edema (pulmonary, pleural effusion, ascites, peripheral).
– In patients with severe OHSS, 99% present with ascites, 54% with gastrointestinal symptoms, 30% with oliguria, 13% with peripheral edema, and 6% with peritonitis.
– Severe edema and intravascular dehydration may result in end organ injury.
– Defer pelvic exam in those with moderate/severe OHSS (high risk of cyst rupture).
– Mild, moderate, severe, critical based on clinical features and laboratory findings.

Evaluation:
– Obtain CBC, basic metabolic panel, liver enzymes, direct/indirect bilirubin, alkaline phosphatase, albumin, coagulation studies (including fibrinogen), venous blood gas, serum osmolality, pregnancy test/hCG level, type and screen, urinalysis, and lactate level.
– Indications for paracentesis include symptomatic complaints such as dyspnea, abdominal distention, and oliguria. Additional indications include evaluation for spontaneous bacterial peritonitis and the presence of intra-abdominal hypertension.
– Obtain imaging based on clinical assessment (ie, chest x-ray, CT for PE, CT head for altered mental status, etc.).
– Bedside ultrasound can evaluate ovarian size, presence of ascites, ovarian torsion, ectopic/heterotopic pregnancy, vascular thrombosis, interstitial pulmonary edema, pleural effusions, pericardial effusion, and any associated tamponade physiology.
Management:
– Dependent on severity and presence of comorbid conditions.
– Early consultation with the obstetrics and gynecology team, as well as any subspecialties, is recommended.
– The treatment of OHSS is primarily supportive. In most cases, OHSS is mild and follows a self-limited course.
– Mild and moderate OHSS may be treated on an outpatient basis with symptomatic relief, monitoring, strict return precautions, and close follow up in 2-3 days.
- Limit fluid intake to < 2 per day, monitor weight/abdominal girth, avoid nephrotoxic agents (NSAIDs).
- Consider thromboprophylaxis with LMWH.
– For severe, management targets maintaining circulatory hemodynamics, mobilizing fluid from the third space back into the vessels, correcting hemoconcentration, and respiratory support.
- Correct hypovolemia, hypotension, and decreased renal perfusion, accepting that fluid administration may contribute to the accumulation of ascites. NS or balanced crystalloid solution is the initial resuscitation fluid of choice. Albumin can be used for HCT > 45%, albumin < 3 g/dL, or significant ascites. Target urine output > 20-30 mL/hr.
- Vasopressors may be required. Norepinephrine vs. dopamine can be used. Dopaminergic agonists, including cabergoline, are effective therapies for the prevention of OHSS via blockage of VEGF expression.
- Correct electrolyte abnormalities. Current evidence suggests that hypertonic saline solutions, either alone or in combination with colloid solutions, result in significant reduction in intra-abdominal pressure while expanding intravascular volume and correcting hyponatremia present in OHSS.
- Pulmonary support may involve thoracentesis, oxygen supplementation, non-invasive ventilation (NIV), or mechanical ventilation.
- Abdominal compartment syndrome (ACS): Non-operative management of ACS should focus on the following: 1) evacuating intestinal contents via naso or oro-gastric tube placement, 2) evacuating any intra-abdominal space-occupying lesions (e.g. ascites), 3) improving abdominal wall compliance, 4) optimizing fluid resuscitation and 5) optimizing systemic and regional perfusion status.
- When infection is suspected, empiric antibiotic therapy should be initiated.
Disposition:
- Mild to moderate OHSS may be managed on an outpatient basis, while severe OHSS requires inpatient management.
References:
- Timmons D, Montrief T, Koyfman A, Long B. Ovarian hyperstimulation syndrome: A review for emergency clinicians. Am J Emerg Med. 2019 Aug;37(8):1577-1584. doi: 10.1016/j.ajem.2019.05.018. Epub 2019 May 7. PMID: 31097257.




