Authors: Michael Purcell (EM Resident Physician, OSU Wexner Medical Center) and Mark J. Conroy, MD (Assistant Professor of EM, OSU Wexner Medical Center) // Edited by: Alex Koyfman, MD (EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital, @EMHighAK) & Justin Bright, MD (@JBright2021)
Case
A 42 year-old woman is referred to the emergency department for treatment of suspected fungal meningitis. She underwent lumbar puncture 12 days earlier in which an undifferentiated fungus grew. Her history is notable for sinus surgery approximately 2.5 months ago and progressively worsening headaches and visual changes since 10 days after the procedure. She reports no increase in drainage from her eyes. She denies pain in her eyes or pain with eye movements. She has not noticed any floaters, but has had increasing photosensitivity during this time. She has no other pertinent medical history, including immunosuppressive medications or comorbidities.
Background
Endophthalmitis is a rare, but clinically significant infection. It is often misdiagnosed due to the multitude of other ocular diseases that share similar presenting symptoms. It results from an infectious or non-infectious inflammatory process of the vitreous and aqueous humors. Missed or late diagnoses can have severe consequences, including permanent vision loss. The natural history of the disease thus necessitates a high degree of clinical suspicion in all patients, especially those at increased risk.
Endophthalmitis can be further classified as either exogenous or endogenous depending on the source of infection. Exogenous endophthalmitis results from direct inoculation via surgery, trauma, or peri-ocular infections. Surgery, in particular cataract surgery, is the leading cause of endophthalmitis in adults, although it can occur in up to 10% of cases of ruptured globe or penetrating eye injury. Endogenous cases result from hematogenous seeding of the eye. Common risk factors include immunodeficiency, diabetes, malignancy, intravenous drug use, organ transplant, endocarditis, or chronic steroid use.
Diagnosis/Management
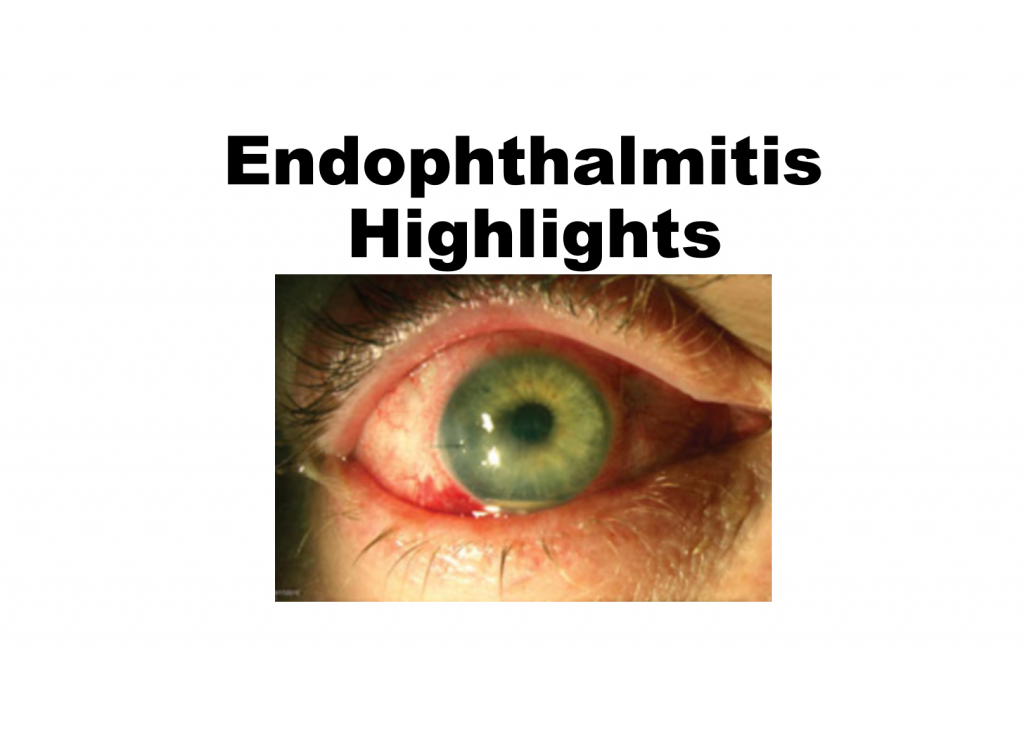
The diagnosis of endophthalmitis is made through history, clinical examination, and positive vitreous or aqueous cultures. Presenting complaints vary widely and include: blurred vision, increased IOP, swollen eyelids, chemosis, conjunctival injection, hypopyon, decreased red reflex, cell and flare, proptosis, and decreased ocular mobility. Given the variable presentations, emergency department management focuses on investigating at risk patients. In addition, emergency department physicians should perform an eye exam on septic patients with ocular complaints or altered mental status in order to avoid missing hematogenous seeding of the eye.
If endophthalmitis is strongly suspected or confirmed, blood cultures should be obtained prior to initiating systemic antibiotics. Endogenous endophthalmitis is often caused by coagulase negative staphylococcus, while exogenous cases are usually the result of staphylococcus or streptococcus. Antibiotic treatment should be aimed at these bacterial species. Definitive treatment, however, requires intra-vitreal antibiotic injections. For this reason, immediate ophthalmology involvement is needed after systemic antibiotics are started. Patients with severe vision loss may even need debridement and vitrectomy in the operating room. Interestingly, one large study showed that although systemic antibiotics comprise part of the standard of care, they may have no benefit in post-cataract surgery infections. This underscores the need for immediate involvement of ophthalmology for intravitreal antibiotics.
In cases of trauma or penetrating eye injury, emergency department management should focus on prophylaxis rather than treatment. The first step is to determine whether there is a retained foreign body via ultrasound or CT scan. Traumas with retained foreign bodies require prophylactic, intra-vitreal antibiotics. In other cases of ocular trauma, systemic prophylaxis with vancomycin and ciprofloxacin is sufficient. If patients develop post-traumatic endophthalmitis, then treatment with both systemic and intra-vitreal antibiotics is warranted.
Pearls
- Early recognition and a high index of suspicion in patients with risk factors or altered mental status are crucial given the sequelae of delayed treatment.
- Bilateral involvement occurs in 14-25% of cases, with right eye predominance due to blood flow.
- Early involvement of ophthalmology is a must, as patients will need intravitreal antibiotics and possibly vitrectomy.
- The most common causative organism in exogenous and endogenous cases are gram positive staph and strep organisms.
- Exogenous fungal inoculations can have a prolonged latency period up to seven weeks.
- Prevention with prophylactic antibiotics is key in post-traumatic cases, especially if there is a retained foreign body.
- Risk for development is increased with the presence of intraocular foreign body following trauma.
Pitfalls
- Failing to broaden evaluation once critically ill patients are stabilized.
- Failing to ask about visual changes in critically ill patients.
- Failing to involve ophthalmology, as definitive treatment with intravitreal antibiotics, culture, and vitrectomy cannot be performed in the emergency department.
- Misdiagnosis is common as symptoms may mimic glaucoma, conjunctivitis, iritis, scleritis, anterior uveitis, orbital cellulitis, mucormycosis, cavernous sinus thrombosis, and other ocular pathology.
References/Further Reading
- Andreoli CM, Andreoli MT, Kloek CE, Ahuero AE, Vavvas D, Durand ML. Low rate of endophthalmitis in a large series of open globe injuries. Am J Ophthalmol. 2009 Apr;147(4):601-608.
- Busbee BG. Advances in knowledge and treatment: an update on endophthalmitis. Curr Opin Ophthalmol 2004;15:232–37.
- Khan S, Athwal L, Zarbin M, Bhagat N. Pediatric infectious endophthalmitis: a review. J Pediatr Ophthalmol Strabismus. 2014 May-Jun;51:140-53.
- Safneck JR. Endophthalmitis: a review of recent trends. Saudi J Ophthalmol. 2012;26:181-189.
- Shrader SK, Band JD, Lauter CB, Murphy P. The clinical spectrum of endophthalmitis: incidence, predisposing factors, and features influencing outcome. J Infect Dis 1990;162:115-120.
- Soheilian M, Rafati N, Mohebbi MR, Yazdani S, Habibabadi HF, Feghhi M, Shahriary HA, Eslamipour J, Piri N, Peyman GA; Traumatic Endophthalmitis Trial Research Group. Prophylaxis of acute posttraumatic bacterial endophthalmitis: a multicenter, randomized clinical trial of intraocular antibiotic injection, report 2. Arch Ophthalmol. 2007 Apr;125(4):460-5.
- Results of the Endophthalmitis Vitrectomy Study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Endophthalmitis Vitrectomy Study Group. Arch Ophthalmol. 1995 Dec;113(12):1479-96.
- http://www.ncbi.nlm.nih.gov/pubmed/24768670




