
Author: Landon M Hatfield, MD (LSUHSC Baton Rouge Emergency Medicine Residency Program, Our Lady of the Lake Regional Medical Center) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF)
The young, the apprehensive, and the altered patient pose a difficulty to the ED physician with regard to complicated facial laceration closure. Local anesthesia may suffice for simple wounds in cooperative patients, but unlikely to be sufficient in the less cooperative. Topical anesthetics and or local anesthesia can be used for simple lacerations less than 4 cm as long as they do not penetrate deep into the dermis or subcutaneous layers; however infiltrations distort tissue planes and wound margins making re-approximation and closure less precise. Alternatively regional facial nerve blocks offer another means by which local anesthesia can be attained, especially in wounds greater than 4 cm and in those requiring significant cosmesis. This is a skill often overlooked but one quite useful. There are five regions of interest and we will review anatomy and technique of each.
A few tidbits before we begin… Skin and mucosal membranes must first be cleansed and sterile field prepared prior to nerve blockade. Topical 2% viscous lidocaine should be used prior to nerve blockade for both intraoral and superficial procedures. Buffered lidocaine with epinephrine provides not only anesthesia but also is vasoconstrictive and is to be used with caution on facial tissues and flaps as the constrictive properties can compromise tissue viability. The total dose of 1% lidocaine with epinephrine should not exceed 7 mg/kg (0.7mL/kg) and 4mg/kg without epinephrine. In older children and adults, paresthesias are a sign that needle tip is contacting desired superficial nerve terminus. For most blocks, a small needle 25 or 27 gauge is used, and 2-3 mL of buffered lidocaine 1% with epinephrine will be used, however more or less may be required depending on patient and region to be anesthetized. Roughly 2-3 minutes after infiltration, one can expect sufficient anesthesia with lidocaine and 10-20 minutes if using a longer acting analog such as bupivacaine. Irrigation is of great importance and a good rule of thumb is at least 20 to 25 mL of normal saline per 1 cm of wound length. Some studies have shown tap water in developed countries to be nearly as efficacious as normal saline, however we will not get into this discussion in this post. Betadine and hydrogen peroxide should be avoided as they are irritants and potentially toxic to exposed wound tissue ,and chlorhexidine, which can stain teeth, is not to be used intraorally. Lastly, procedural sedation can be used when physician or patient safety could be compromised, larger wounds requiring significant revision, and lacerations requiring aggressive cleansing and decontamination.
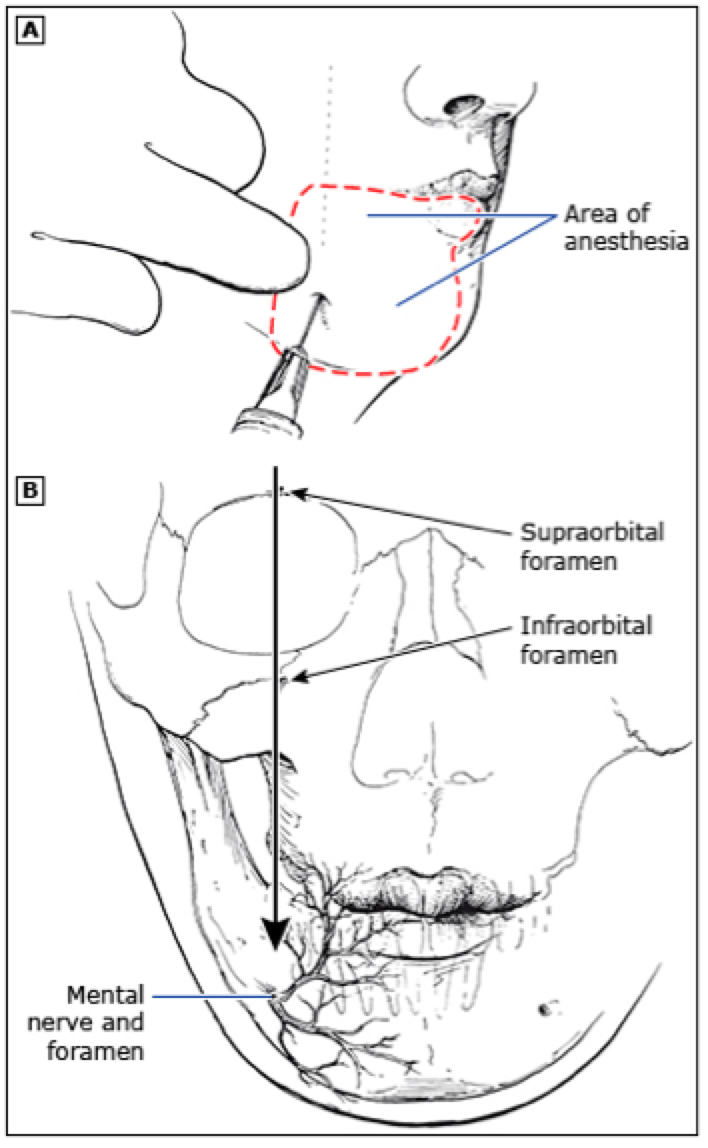
Figure 1. Superficial approach to mental nerve blockade. A vertical line connects the supraorbital notch, infraorbital foramen, and mental foramen that all give rise to the terminal sensory branches of the trigeminal nerve
The mental nerve block anesthetizes the inner oral mucosa, gingiva, and lower lip and exits its foramen just below the canines of the mandible and first premolars. The mental nerve foramen is located in line with the infraorbital and supraorbital foramen and may be palpated through the skin, but is not possible in all patients. For the superficial approach, a needle is inserted perpendicularly through the skin at a 45°-90° angle relative to foramen (Figure 1). The intraoral approach is better tolerated and is completed after 2% viscous lidocaine is applied topically to the buccal mucosa. 5-10 minutes later, the mucosa is dried and lip is everted. A small gauge needle is inserted at the gingival line, directed 1 cm inferiorly and 3-5 mL of buffered lidocaine is injected (Figure 2).

Figure 2. Intraoral approach to mental nerve block
Used with permission from Gregori M. Kurtzman, DDS
The infraorbital nerve block anesthetizes the lower eyelid, medial cheek, and the ipsilateral side of the nose and upper lip. The infraorbital nerve exits its foramen 1 cm below the midpoint of the lower orbital rim just above the canine teeth of the maxilla. The block is accomplished in one of two approaches. The intraoral approach is better tolerated than is the superficial, subcutaneous method. Topical 2% viscous lidocaine is applied using a q-tip to the gum line above the maxillary canine. 5-10 minutes after topical anesthesia, the mucosa is dried and using non-injecting hand, the upper lip is retracted using the thumb while the index and middle fingers are placed over the inferior optic rim. A small gauge needle is then inserted at the gingival line, directed superiorly halfway between entry site and orbital rim and 3-5 mL of buffered lidocaine is injected (Figure 3). In some patients it may be possible to palpate the infraorbital foramen through the skin but more likely through the intraoral approach. If the patient is capable of responding, paresthesias in appropriate distribution are indicative of proper location as well. The superficial approach is accomplished by inserting the needle perpendicular to or at 45° angle to the foramen.
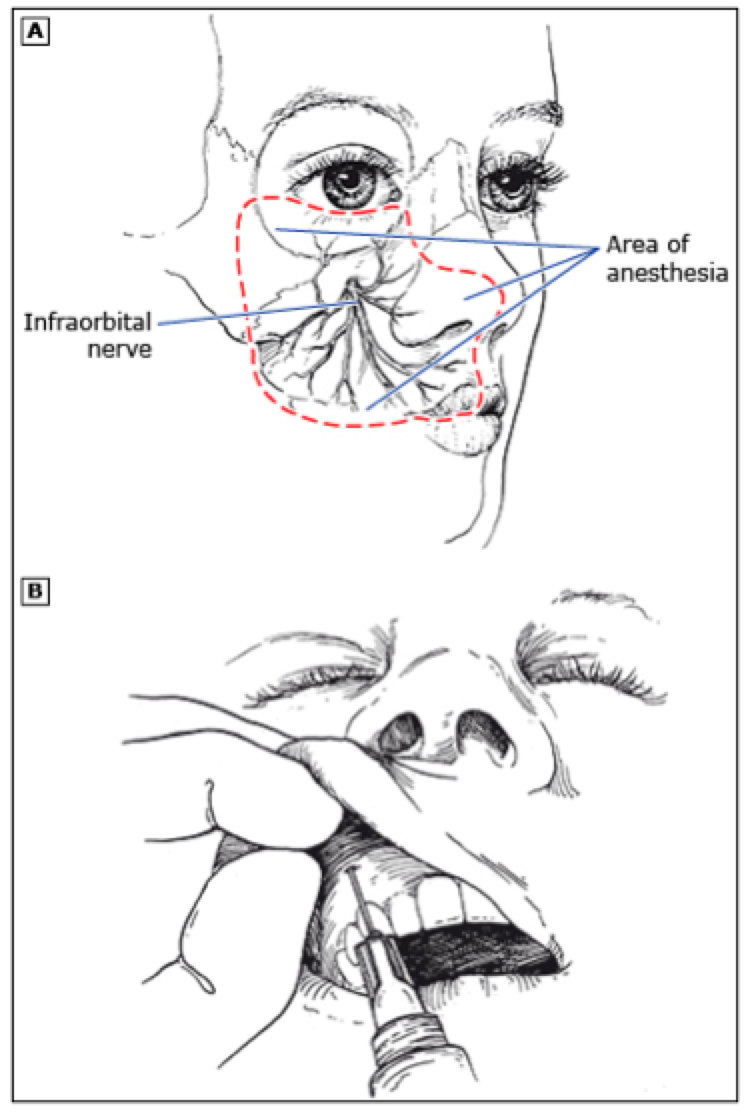
Figure 3. Intraoral approach to Infraorbital nerve blockade
The supraorbital and supratrochlear nerve blocks provide anesthesia from the vertex of the scalp to the bridge of the nose. The supraorbital nerve exits the supraorbital foramen just above the supraorbital ridge. The supratrochlear nerve exits roughly 1cm medial to the supraorbital foramen. The supraorbital nerve is responsible for the majority of the forehead and the supratrochlear nerve the nose. After preparation of a sterile site, a wheal is raised and then 2-3 mL of buffered lidocaine infiltrated with a small needle above the eyebrow and in line with the pupil. Needle is then directed medially and 3-5 mL is then infiltrated in a horizontal line that contacts the most medial portion of eyebrow (Figure 4).
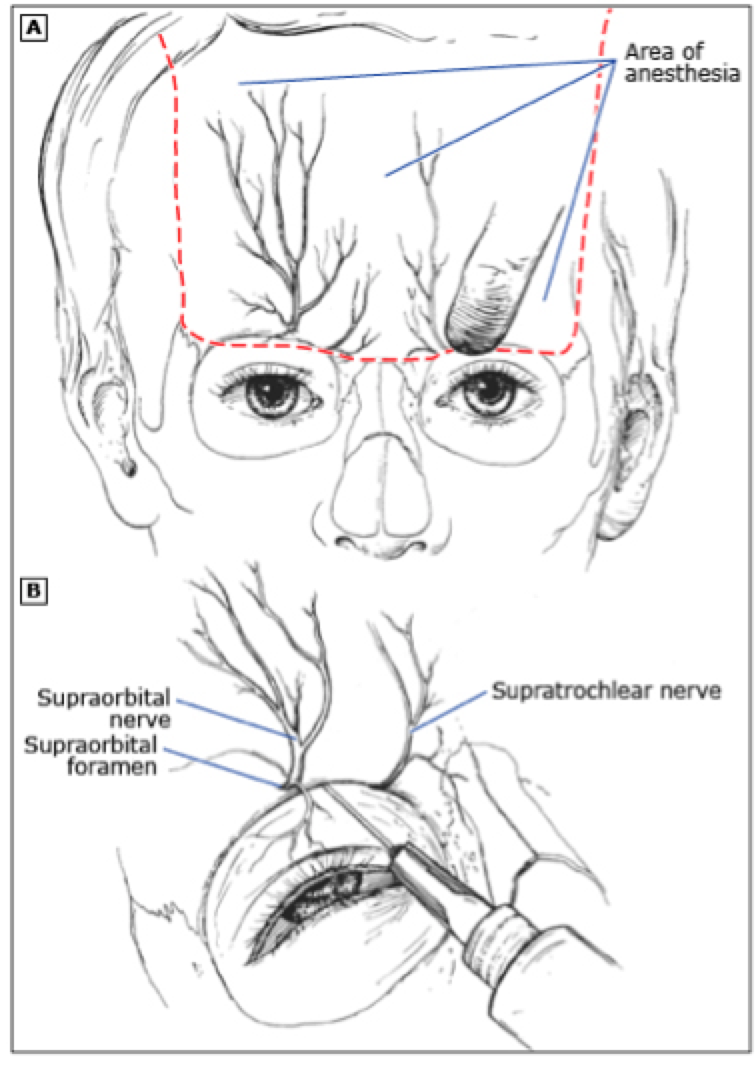
Figure 4. Supraorbital and Supratrochlear nerve blockade
The regional auricular block anesthetizes the entire ear except the concha and meatus that are innervated by the vagus nerve. The auricle is innervated by the auriculotemporal nerve superiorly and medially and the greater auricular nerve and lesser occipital nerve laterally and inferiorly. After a sterile field is prepared at the base and superior portions of auricle, a small needle is used to enter skin just below ear and a small wheal is raised. The needle is then directed posteriorly towards the mastoid and 2-3 mL of lidocaine is injected along the needle tract as the needle is withdrawn. A second tract of 2-3 mL is then made without completely removing needle directed anteriorly. The same method is used superior to the auricle by entering the skin just above and forming a second v-shaped tract (Figure 5). Epinephrine is to be avoided, as the vascular supply of the cartilage is poor.
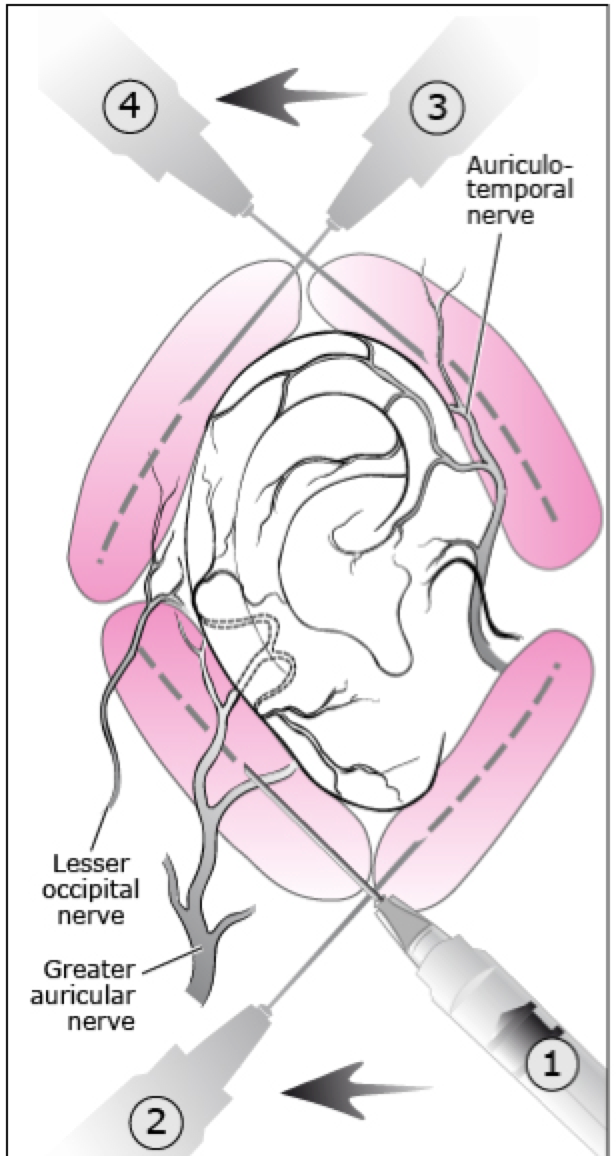
Figure 5. Auricular innervation and regional blockade.
Effective anesthesia allows for optimization of many procedures, including complex laceration repair. Distortion of tissues at or around the site of local anesthetic injection may complicate laceration closure, in which case a regional block improves outcomes. The key to regional anesthesia is familiarity with anatomy of the nerve and associated landmarks. Paresthesias may help to localize the nerve, but should be minimized to reduce the risk of residual neuropathy. Minimization of sedation and increased safety make regional anesthesia very useful especially when large amounts of local anesthesia would be required. Regional nerve blocks represent another tool to be employed in the right context, and familiarity with anatomy and technique can aid the Emergency Physician in complex laceration closure.
References / Further Reading
-Cimpello LB, Deutsch RJ, Dixon C, et al. Illustrated techniques of pediatric emergency procedures. In: Textbook of Pediatric Emergency Medicine, 6th ed.
-Hollander JE, Camacho M. Assessment and management of facial lacerations. In: UpToDate, Wiley JF (Ed), UpToDate, Waltham, MA. (Accessed on November 15, 2015.)
-Malloy KM, Hollander JE. Assessment and management of auricle (ear) lacerations. In: UpToDate, Wiley JF (Ed), UpToDate, Waltham, MA. (Accessed on November 15, 2015.)
-Tintinalli, Judith E, and J S. Stapczynski. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. New York: McGraw-Hill, 2011.
-Cimpello LB, Deutsch RJ, Dixon C, et al. Illustrated techniques of pediatric emergency procedures. In: Textbook of Pediatric Emergency Medicine, 6th ed, Fleisher GR, Ludwig S (Eds), Lippincott, Williams & Wilkins,





1 thought on “Facial Nerve Blocks”
Pingback: visual aid: facial nerve blocks | DAILYEM