
Authors: Ryan Mason, MD and Alex St. John, MD (University of Washington, Division of Emergency Medicine) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Chief Resident at SAUSHEC, USAF)
Hand injuries can inflict a high degree of morbidity in the form of pain and loss of the ability to work or perform activities of daily living. Due to the hand’s highly specialized and complicated anatomic structure, many of these injuries can be subtle. Indeed, an entire sub-specialty of surgery exists to care for the hand. Our job as emergency physicians is to identify these elusive injuries for further specialist management in order to avoid their devastating consequences.
This article will summarize some of the more subtle and risky pathologic hand injuries through a review of the current literature.
1. “Sausage Digit”: Pyogenic Flexor Tenosynovitis (PFT)
Adapted from Draeger et al, 2012 Review of Flexor Tendon Sheath Infections of Hand1
Anatomy
- Flexor tendons of the digits are enclosed within sheathes that extend to the palmar surface of the hand.
- Suppurative infection can damage these sheathes leading to stiffness, tendon disruption, and even the need for amputation.
Presentation
- Most often caused by penetration injury 2-5 days prior to presentation, possibly longer in immunocompromised patients.
- Clinical diagnosis, but radiographs should be used to rule out foreign bodies or bony injury.
- Most commonly Staph & Strep species, but GNR are also very common.
The Exam
Kanavel’s Signs: Used as clinical diagnosis criteria since 1933. While no studies exist validating sensitivity or specificity, one 2007 study characterized the frequency of each sign in a retrospective cohort of 75 patients with PFT:2
- Fusiform digit swelling: 97%
- Pain with passive extension (earlier finding): 72%
- Semi-flexed digital posture: 69%
- Tenderness along flexor tendon sheath: 64%
- Other studies found that only 50% of patients with PFT have all four signs.
- Tenderness along the flexor tendon sheath can be used to distinguish PFT from other finger infections such as: Herpetic Whitlow, Felon, and Septic Arthritis.
Management
- PFT requires prompt antibiotics and surgical intervention.
- IV antibiotics should be initiated to cover Staph aureus, Streptococcus, and Gram-negative organisms. The article suggests Vancomycin and Piperacillin-Tazobactam.
- Expeditious hand surgery consultation.
Bottom Line:
- Suspect PFT with penetrating injuries to palmar surface of hand.
- Clinical exam can be helpful in raising suspicion, but cannot rule out
- This is a hand emergency. If suspicious, initiate broad antibiotic therapy and consult a hand surgeon.
2. Compartment Syndrome of Hand
Compartment syndrome of the hand is a rare, but devastating injury if not identified and treated in a timely fashion. Most information on the entity is drawn from case reports and series, with many inferences made from other extremities.3 That being said, we will review what is currently known on the topic.
Anatomy
The hand contains multiple compartments divided by fascia. When a compartment’s pressure increases, blood supply can become compromised leading to tissue injury and eventual loss of function.
One review article lists six* compartments of the hand:4
- Thenar
- Hypothenar
- Adductor
- Interosseous
- Digital
- Carpal Canal/Central Palmar
*Note that depending on the source, the number of hand compartments can vary between 5 and 10. Regardless of their quantity and name, know that there are multiple, distinct areas within the hand at risk for compartment syndrome.
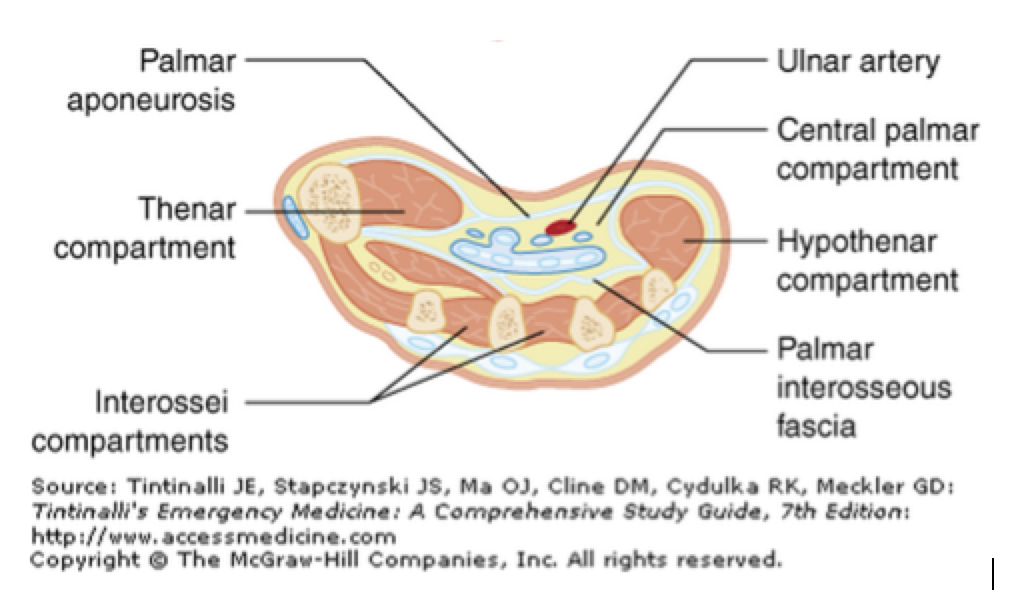
Figure 1. One (of many) schema depicting the various compartments of the hand.
Presentation
Compartment syndrome of the hand can result from a myriad of causes which increase intra-compartmental pressure. Many review articles cite risk factors and etiologies of compartment syndrome regardless of location. The best attempt at studying etiologies is cited below:
Kalyani et. al. 2011: Review of compartment syndrome etiologies
- Included ENTIRE upper extremity
- 80 patient cohort
- Most common causes included:
- Fracture (30%)
- Penetrating Injury (15%)
- Arterial Injury (11%)
Other cited etiologies of hand compartment syndrome include: soft tissue injury, crush injury, envenomation, and iatrogenic causes such as infiltrated IVs and restrictive splints/casts.3–5
The Exam
Much has been written on the signs and symptoms of compartment syndrome and the difficulties in its clinical diagnosis.7 Compartment syndrome of the hand is no different. The following exam findings are noted in some literature to be specific for compartment syndrome of the hand:
- Pain with passive motion at MCP joint.8
- Tense, swollen hand in an intrinsic minus position.9 (Figure 2)
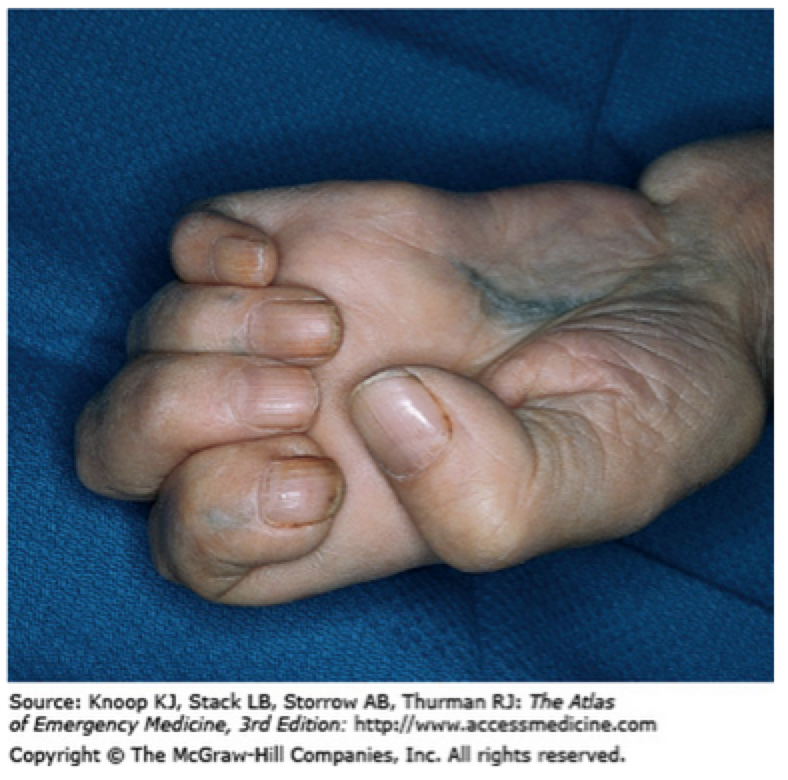
Figure 2. Intrinsic Minus or “Claw Hand”
Unfortunately, the sensitivity, specificity and predictive values of these findings have either never been tested or been found to be low with large inter-observer variability.3,4 Thus, physical exam should raise suspicion for compartment syndrome in the hand, but by no means be used to rule it out.
Due to the difficulties of clinical exam, direct measurement of the compartment using a commercial device is the preferred method of confirming the diagnosis. The most current review article recommends fascial release when a compartment pressure of the hand is within 30mmHg of the patient’s diastolic blood pressure.3
Management
- Prompt surgical consult with Hand specialist.
- Fasciotomy.
Bottom Line
- Suspect hand compartment syndrome with similar etiologies of compartment syndrome elsewhere.
- Physical exam findings should raise your suspicion, but cannot rule out compartment syndrome. Confirm with compartment pressure testing.
- If compartment pressure of the hand is within 30mm Hg of the patient’s diastolic blood pressure, consult a hand surgeon for fasciotomy.
3. A Skiing Gamekeeper’s Menace: Ulnar Collateral Ligament Disruption
Adapted from Madan, et al. UCL Injury 2014 Review Article10
Anatomy
The Ulnar Collateral Ligament (UCL) extends over the ulnar aspect of the thumb MCP joint providing strength and stability to the thumb. Injury at this site can cause lack of stability and cause disability by limiting pincer strength.
Presentation
- Acute: Forceful radial movement of the thumb, such as a falling with a ski pole or sudden stop on a bicycle.
- Chronic: Repetitive ulnar movement against resistance, such as manual trades or breaking fowl necks.
The Exam
While ultrasound and MRI can confirm a UCL injury, the diagnosis remains primarily clinical. To identify an UCL injury, ligamentous laxity must be tested. If exam will be limited by pain, consider regional nerve blocks (see diagram below). Holding the thumb in 30° flexion at the MCP, stabilize first metacarpal and apply radial stress to thumb until reaching a firm end-point (testing the proper UCL). Repeat with thumb in 30° extension (testing the accessory UCL). Deviation of 35° on the affected side or a difference of 15° between the affected and opposite sides in flexion indicates a UCL tear. (Figure 3)
Additionally, examine thumb for presence of a Stener Lesion, which manifests as tender swelling at the base of thumb on the ulnar side and represents a proximally displaced UCL lying superficial to the overlying adductor aponeurosis. Stener Lesions are important information for our orthopedic colleagues, as they may indicate the need for surgical repair.
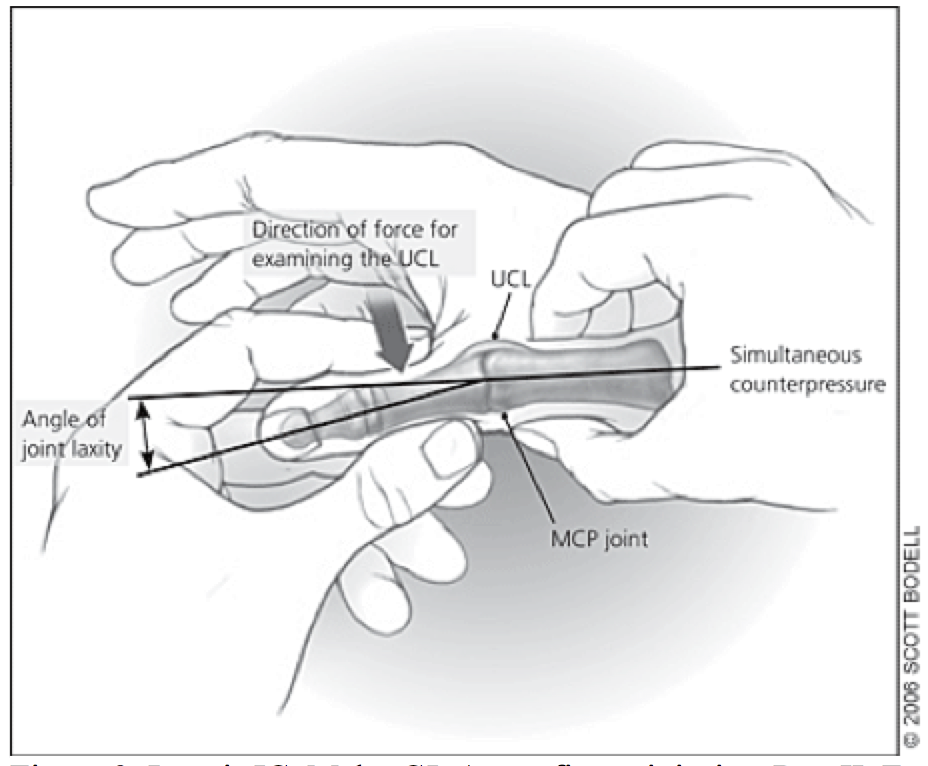
Figure 3. Leggit JC, Meko CJ. Acute finger injuries: Part II. Fractures, dislocations, and thumb injuries. Am Fam Physician. 2006;73(5):827-834
Management
While not used to confirm diagnosis, any suspected UCL injury should have radiographs. Associated bony avulsion fractures are seen in 20%–30% of UCL ruptures.
Management typically consists of immobilization for 4 weeks in a thumb spica splint. Orthopedic follow up should be arranged.
Bottom Line:
- Thumb UCL injury often from forceful radial deviation of thumb.
- Untreated, can result in weakness of pincer grasp.
- Test for laxity at MCP when stressed radially.
- Assess for Stener lesions.
- Treat with thumb spica immobilization.
References / Further Reading
- Draeger RW, Bynum DK. Flexor Tendon Sheath Infections of the Hand Abstract. J Am Acad Orthop Surg. 2012;20(6):373-382.
- Tenosynovitis PF, Pang BH, Teoh L, et al. Factors Affecting the Prognosis of Pyogenic Flexor Tenosynovitis. 2007:1742-1748. doi:10.2106/JBJS.F.01356.
- Codding JL, Vosbikian MM, Ilyas AM. Acute Compartment Syndrome of the Hand. J Hand Surg Am. 2015;40(6):1213-1216. doi:10.1016/j.jhsa.2015.01.034.
- Leversedge FJ, Moore TJ, Peterson BC, Seiler JG. Compartment syndrome of the upper extremity. J Hand Surg Am. 2011;36(3):544-559; quiz 560. doi:10.1016/j.jhsa.2010.12.008.
- Seiler JG, Olvey SP. Compartment syndromes of the hand and forearm. J Am Soc Surg Hand. 2003;3(4):184-198. doi:10.1016/S1531-0914(03)00072-X.
- McQueen MM, Gaston P, Court-Brown CM. Acute compartment syndrome. Who is at risk? J Bone Joint Surg Br. 2000;82(2):200-203.
- Kam JL, Hu M, Peiler LL, Yamamoto LG. Acute compartment syndrome signs and symptoms described in medical textbooks. Hawaii Med J. 2003;62(7):142-144.
- Halpern AA, Greene R, Nichols T, Burton DS. Compartment syndrome of the interosseous muscles: early recognition and treatment. Clin Orthop Relat Res. 1979;(140):23-25.
- Ouellette EA, Kelly R. Compartment syndromes of the hand. J Bone Joint Surg Am. 1996;78(10):1515-1522.
- Madan SS, Pai DR, Kaur A, Dixit R. Injury to Ulnar Collateral Ligament of Thumb. Orthop Surg. 2014;6(1):1-7. doi:10.1111/os.12084.
- http://www.ncbi.nlm.nih.gov/pubmed/?term=%22flexor+tenosynovitis%22+%22emergency+medicine%22
- http://www.ncbi.nlm.nih.gov/pubmed/26035497
- http://www.ncbi.nlm.nih.gov/pubmed/24686026
- http://www.ncbi.nlm.nih.gov/pubmed/23340119





2 thoughts on “Handy Knowledge: subtle and high-risk hand injuries”
Pingback: Global Intensive Care | AIR Series: Orthopedics Upper Extremity Module (2016)