Author: Erica Simon, DO, MHA (EM Chief Resident at SAUSHEC, USAF) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Stephen Alerhand, MD (@SAlerhand)
It has been a long night in the department. After ordering supplies for your patient with an auricular laceration, you sit down at your desk to review the landmarks for an auricular block. Within minutes, “trauma team to the trauma room” is paged overhead. As you don your PPE, an intoxicated 32 year-old male wheels by, profusely bleeding from his scalp. The patient is post-assault with a beer bottle. Initial VS: BP 81/56, HR 120.
If either of these scenarios make you wish that you had consulted Roberts & Hedges recently, have no fear – we will take a minute to review the basics and offer tips for success in addressing a number of commonly encountered HEENT procedures.
Head
Repair of Facial Wounds
Patients with facial lacerations commonly present to the ED for treatment. As with all encounters, care begins with an assessment of the ABCs and intervention as appropriate. Physical exam of a wound requires an evaluation of location, length, depth, and width; a search for contaminants, and an exploration of deep structures (tendons, muscles, bones) for neurovascular injury.1-3 Goals for patient wound care include: obtaining hemostasis, attaining functional closure, decreasing the risk of infection, and minimizing scar formation.1-3
Anesthetics
Cleaning, irrigating, and exploring a wound is often times painful. Topical, local, and regional anesthesia should be chosen based upon ED availability, desired duration of anesthesia, and anatomic location of the injury (keeping in mind the potential requirement for the preservation of wound margins for repair). The American Academy of Pediatrics currently recommends the use of topical anesthetics for simple lacerations of the head, neck, and extremities, or trunk <5 cm in length.4 Time of onset for topical agents may vary from 10-30 minutes.3
Lidocaine, bupivacaine, and procaine are commonly used for local and regional anesthesia. The ED physician should be aware of maximum toxic doses prior to application:
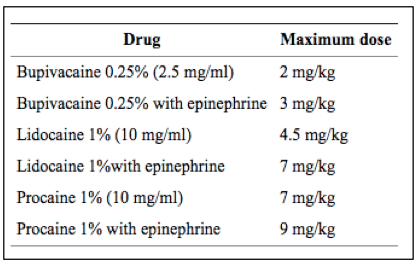
Dose Limitations of Locally Injected Anesthestics3
Wound Irrigation & Closure
While study data varies considerably, it is advised that irrigation volumes of 50 to 100 ml per cm of laceration length be utilized to clear wounds of contaminants.3 Experts recommend primary closure for clean wounds localized to the extremities for up to ten hours post injury.1-3 Given the vascular nature of the face and scalp, wounds to these areas may be closed for up to twelve hours post injury.3 Significantly contaminated lacerations and abrasions should be considered for delayed primary closure. In employing delayed primary closure, a provider should irrigate the wound to clear it of as many contaminants as possible, and refer a patient for re-evaluation 3-5 days post injury. If upon re-evaluation the site is without signs or symptoms of infection, margins may be debrided and the tissue closed.1-3 Grossly contaminated wounds should be irrigated and allowed to heal by secondary intention.1-3
Semer provides an excellent summary of optimal wound closure materials in his Practical Plastic Surgery for Non-Surgeons.5,6
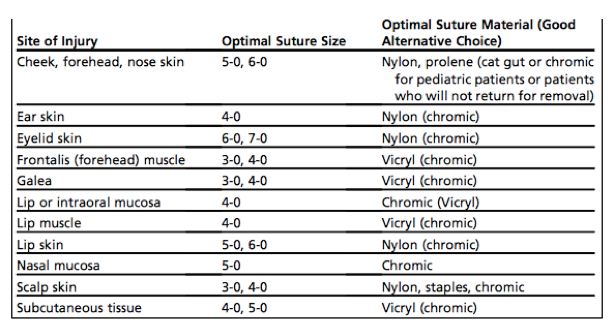 *Semer notes that Prolene may be substituted where nylon is recommended.5,6
*Semer notes that Prolene may be substituted where nylon is recommended.5,6
Tetanus and Antibiotics
For all patients with wounds, history taking should include questioning regarding tetanus vaccination status. Current CDC guidelines for tetanus administration in the setting of an injury are detailed below:
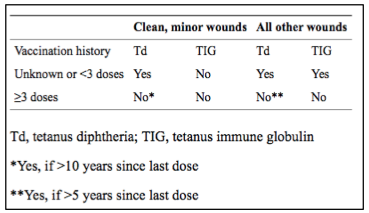
CDC Tetanus Vaccination Recommendations3
Antibiotics should be considered for all patients who are immunocompromised, those who presents with grossly contaminated wounds or deep puncture injuries, those suffering from animal or human bites, and those who presents late in the course of their injury with signs of infection.1-3
Disposition
In general, individuals suffering from hypovolemia secondary to hemorrhage and those experiencing wounds involving > 10% BSA (loss of excess extracellular fluid) often require inpatient management post stabilization.3 Deep wounds to the hands or feet, lacerations involving nerves, arteries, bones, or joints, severe crush injuries, and wounds leading to significant concern regarding cosmetic outcome require consultation with a specialist.7 When appropriate, patients should be referred for aftercare (to include non-absorbable suture or staple removal):
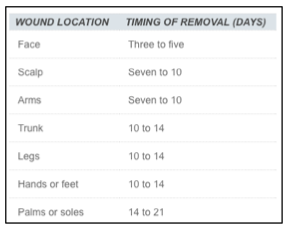
Timing of Suture or Staple Removal7
Note: This post is my no means all encompassing in its discussion of facial wound management. Scalp laceration repair is discussed below given its common occurrence in the ED population. (See Roberts & Hedges for an in-depth review of the management of eyebrow lacerations, lip lacerations involving the vermillion border, and nasal bridge lacerations).
Special Topics
Scalp Laceration Repair – As the scalp is highly vascular, with an arterial supply originating from three branches of the external carotid artery and two branches of the internal carotid artery, patients with scalp wounds often times present with hypotension secondary to blood loss.1,5 If hemostasis is not achieved with the application of direct pressure, several options are available:
- Raney scalp clips
- Figure-of-eight suture (pictured below)
- Hemostats applied to the edge of the wound to control hemorrhage (complication of devitalized tissue)
- Injection of local anesthetic with epinephrine1,2

The subgaleal layer of scalp connective tissue contains veins which drain through vessels of the skull into the venous sinuses of the cranial hemispheres.1 Therefore, scalp wounds must be explored in a hemostatic field as these unaddressed injuries may pre-dispose individuals to infection resulting in osteomyelitis, meningitis, or brain abscesses.1
Quick Review: The scalp consists of five layers:
S – skin
C – connective tissue (superficial fascia)
A – aponeurosis (galea)
L – loose connective tissue (areolar tissue)
P – periosteum
- Lacs penetrating to the galea: repair with 4-0 non-absorbable nylon or polypropylene sutures; interrupted or horizontal mattress.
- Lacs penetrating the muscle layer: repair with 4-0 absorbable sutures; simple interrupted (skin and muscle can be repaired with a single suture through both layers is there is no gaping defect in the muscle layer).
- Skin: close with surgical staples or sutures.1,5
If discharged, patients with a large or deep scalp wound should have a pressure dressing placed so as to avoid hematoma formation.5
Hair Apposition Technique (HAT)
If you have not tried the HAT or modified HAT (modified = Kelly clamps used for hair <1 cm) introduced by Hock, et al. in 2002, it is something worth considering, especially in your next pediatric scalp laceration. Advantages of the HAT include decreased total procedure time as compared to suturing, decreased pain with application, and decreased cosmetic complications (infection risk is comparable to sutures).8-10
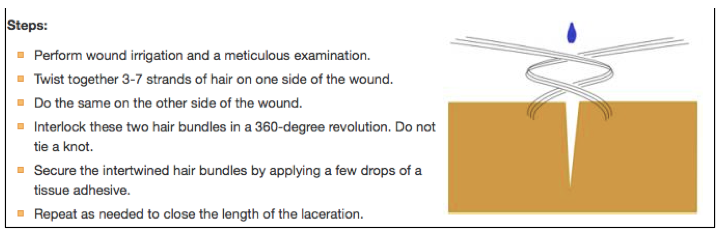 Hair Apposition Technique
Hair Apposition Technique
Contraindications to performing the HAT include:
- Grossly contaminated wounds
- Wounds under tension
- Wounds with poor hemostasis despite hair apposition/pressure
- Scalp lacerations > 10 cm (risk of dehiscence/infection)8
Dogma: “No local epinephrine for the ears, nose, fingers, toes, and penis.”
While current literature continues to advise caution in the application of epinephrine to areas of limited vascular supply, to date, studies utilizing anesthetics with epinephrine have not demonstrated the feared complications of tissue ischemia and necrosis (Largest study: Dutch retrospective review of patient charts, n=10,201 surgical patients, inclusion criteria: application of local anesthetic with epinephrine to the fingers, nose penis, outer ear, and tip of the nose).11,12 Proper injection and infiltrative technique continues to be vital in local anesthetic application.
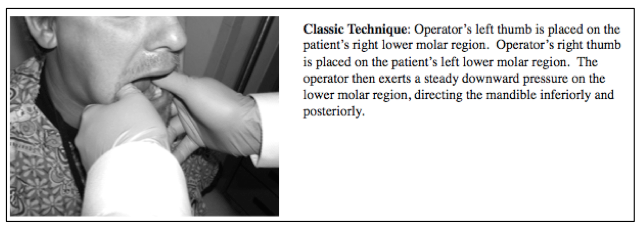
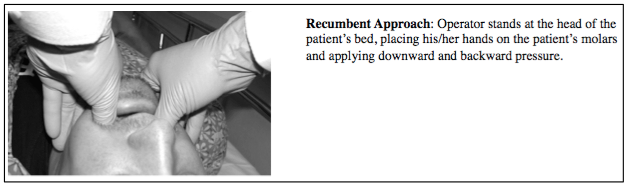
Mandibular Dislocations
Mandibular dislocations may occur in up to 5% of the population during their lifetime.13 The majority of dislocations occur secondary to extremes of mouth opening including yawning, laughing, or eating, but may also occur in the setting of trauma or dystonic reactions to medications.1 Patients often present with acute jaw pain, jaw malocclusion, or inability to open or close the mouth.1,13 Dislocation of the mandible at the TMJ occurs when the condylar head is displaced from the glenoid fossa. While dislocations come in varying flavors, far and wide the most common are bilateral and anterior.1,13 For the sake of keeping this a quick review, we will talk about re-locating the anteriorly dislocated mandible.
Sedation and anesthesia – this is a must. A number of texts cite successful reduction with the use of local anesthetics injected directly into the TMJ space or the lateral pterygoid muscle (for more information on these techniques please see references 14 and 15 below), however procedural sedation may be required.
Care should be taken to avoid self-harm in performing the procedure as sudden masseter spasm and involuntary patient biting may cause digit/hand trauma; gauze and other protective devices including plastic finger splints may be used.13
The following figures are adapted from Chan, et al.

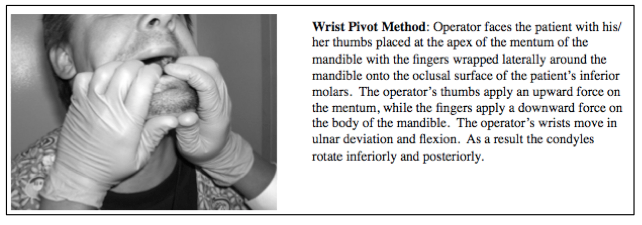
Complications – Patient injuries include spontaneous dislocation after reduction (more common in patients with chronically recurring dislocation), mandibular fracture, joint/cartilage injuries, and dental injuries.1,13
Disposition – After reduction patients should be advised to maintain a soft diet and apply cool compresses intermittently to the TMJs for 48 hours.
Ears
Auricular Lacerations
The ear consists of the EAC, the auricle, and the earlobe. Blood supply to the ear is from the superficial temporal and posterior auricular arteries, and the nerve supply originates from branches of the great auricular nerve (see below).5 Anesthesia for wound exploration and repair is provided through the use an auricular ring block.
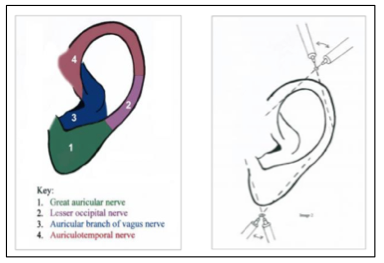 Nerve Supply and Anesthesia of the Ear16
Nerve Supply and Anesthesia of the Ear16
The more you know: Ultrasound is now being utilized in the ED to target the branches of the auricular nerve for improved pain control. Flores and Harring describe their technique in a recent Journal of Emergency Medicine, Ultrasound in Emergency Medicine publication detailed below.
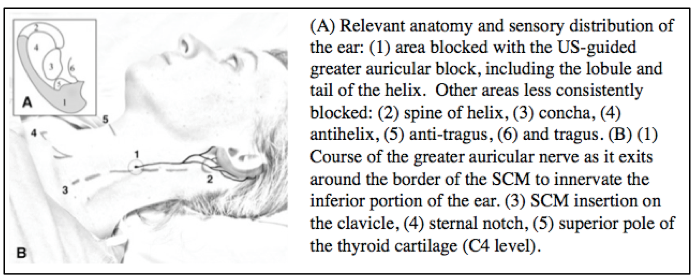 US Guided Auricular Nerve Block17
US Guided Auricular Nerve Block17
The goal of managing an auricular laceration is to cover exposed cartilage and limit hematoma formation.
In addressing an ear lac:
- Trim away jagged skin/cartilage (if the skin cannot be stretched over the exposed cartilage, depending on the location, up to 5mm of cartilage can be removed without causing deformity).1
- Approximate cartilage with 4-0 or 5-0 absorbable sutures (the anterior and posterior perichondrium must be included as sutures tear through cartilage).1,5
If the wound is through-and-through: approximate the posterior surface with 5-0 non-absorbable sutures, then repair the anterior aspect of the wound with 5-0 or 6-0 non-absorbable sutures.
Contaminated Wounds
Cover cartilage by loose skin approximation and prescribe oral antibiotics.1 Tetanus administration is as per CDC recommendations above.
Disposition
All ear lacerations should be enclosed in a compressive dressing to prevent hematoma formation (sequelae = “cauliflower” deformity). The contours of the anti-helix are packed with xeroform and sutures are placed through-and-through to hold the packing in place. The area behind the ear is then supported with gauze and the head wrapped with an ace bandage for compression.18
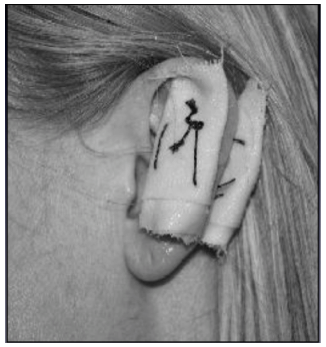
Compressive Auricular Dressing18
Auricular Hematomas
Auricular hematomas may occur as a result of blunt trauma to the external ear, or as a complication of an auricular laceration repair. Two techniques are commonly utilized to drain auricular hematomas: needle aspiration (a 20G needle is placed at the point of maximal hematoma fluctuance, blood is aspirated, and the ear is “milked” to express additional blood), or an open technique employing a scalpel and irrigation. Both drainage procedures require compressive auricular dressings so as to avoid hematoma re-accumulation and again the cauliflower deformity. Similar to auricular laceration repairs, topical or regional anesthesia should be utilized.1,5
In his blog, Closing the Gap – Wound Closure for the Emergency Practitioner, Brian Lin, MD provides an excellent photographic depiction:
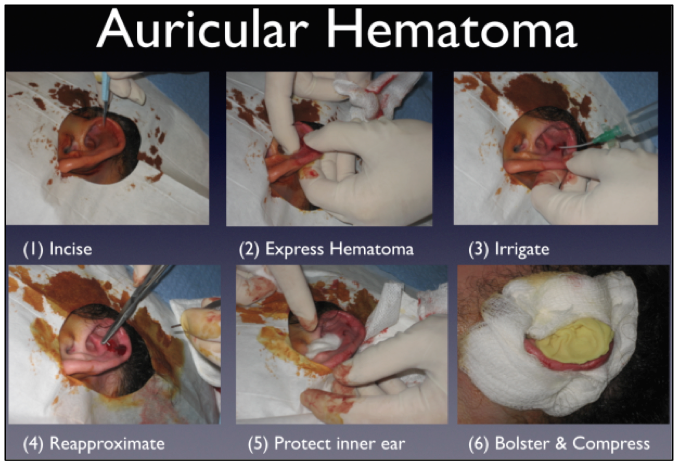
Addressing an Auricular Hematoma18
In “bolstering and compressing,” Roberts & Hedges recommend: utilizing vaseline gauze or saline-soaked packing gauze/cotton to support the ear, placing layers of gauze behind the ear as a posterior pack, covering the ear with multiple layers of gauze, and securing the gauze to the head with kerlix or an elastic wrap.1
Disposition
Experts recommend that anti-Staphylococcal antibiotics be given, and that patients with auricular hematomas be re-evaluated in 24 hours to search for blood re-accumulation. All patients with hematomas lasting >7 days should be referred to a specialist for debridement and repair.1
Auricular Foreign Bodies (FBs)
Cockroaches are the most common auricular FBs in adults. By contrast, children are likely to shove anything from cheese to rocks in their ears without telling an adult. Patients with an auricular FB may present with symptoms of ear pain and fullness to tinnitus and vertigo (suggesting associated TM rupture).
In evaluating an auricular FB, visual inspection of the ear is the most important aspect of the patient encounter. The following require ENT consultation:
- Button batteries (can cause significant tissue damage in a matter of hours secondary to anode/cathode discharge = liquefactive necrosis).19
- Objects that are deep in the ear and appear embedded.1
- Silly putty1
- Sharp objects1
Analgesia/Anesthesia
Auricular rings blocks provide poor anesthesia to the EAC.1,17 As mentioned above, adequate visualization is key. In the majority of cases, young children may require procedural sedation for the removal of auricular FBs.
Methods for FB Removal
Irrigation: Ideal for small objects adjacent to the TM. A 16-18G flexible IV catheter can be attached to a 10 cc syringe or a 1-2 inch section of butterfly needle tubing from which the needle has been removed. NS may then be used to flush the FB from the EAC. This procedure is contraindicated in patient’s with evidence of TM rupture, and should not be used if the FB is composed of organic material given the possibility of FB swelling upon exposure to NS.20
Suction-Tip Catheters: Work well with round FBs. While these are commercially available in a number of sizes, 100-140 mm Hg of negative pressure must be generated for the catheter to adequately be used as an extraction tool.1
Manual Instrumentation: Should be used only when the patient is cooperative, and the object is directly visualized. Instruments range from alligator forceps to cerumen curettes.
Superglue: Most effective for smooth, round objects that are difficult to remove with manual instrumentation.1 Glue is placed on the tip of a straightened paperclip or wooden cotton-tip applicator, allowed to become tacky, and then advanced into the EAC. If the tip dries against the canal wall, iatrogenic trauma may occur.
Katz Extractors/Fogarty Catheters: Both of these devices allow for mechanical removal of auricular FBs. Fogarty catheters were designed for biliary (No. 6) or vascular (No. 4 or 5) procedures, while Katz extractors were created specifically for auricular/nasal FB removal. Both devices function similarly: the catheter is advanced beyond the FB, the balloon gradually inflated with a 3cc syringe, and the FB pulled from the nose, advanced by the inflated balloon.1
 Katz Extractor and Fogarty Catheter21
Katz Extractor and Fogarty Catheter21
Bug Extraction
Insects are often removed by manual extraction. If the insect is still alive, mineral oil or viscous lidocaine may be placed into the EAC prior to removal (kills the bug, effectively eliminating the difficulty of a moving target, and reducing pain associated with insect movement).
In the patient with a FB, do not forget to examine other orifices for a second FB. This is especially true in children.
Complications
Complications of the above methods of FB removal include TM rupture and EAC trauma.
Disposition
Patients with concomitant TM rupture (or iatrogenic TM rupture), EAC infection or trauma, or those post a failed ED extraction should be referred to ENT. It is important to note that failure to ensure appropriate patient follow-up has resulted in documented cases of mastoiditis and meningitis.22
Special Topics
Embedded Earrings – Although rare in the ED (the largest study: a retrospective review of medical records from Cincinnati Children’s Hospital Medical Center from 2000-2005 identified 100 patients with embedded earrings), this complication can be associated with infection and local cellulitis at the time of presentation. Management is facilitated by local anesthesia and incision for removal.23 Antibiotics should be prescribed as appropriate.
Eyes
Exploration of any eye injury should include an assessment of EOMs, visual fields, visual acuity, and globe integrity. Fluorescein stain should be performed for identification of corneal trauma, foreign bodies, and globe trauma (Seidel’s sign – intraocular humor washing away the fluorescein, indicating globe injury). IOP should be assessed if concern for orbital compartment syndrome arises (contraindicated in the setting of globe rupture).1
Eyelid Laceration Repair
In addressing eyelid lacerations, it is important to recognize what is and is not appropriate for ED repair. The following lacerations should be referred to a specialist:
- Lacerations traversing the lid margin (require appropriate repair to avoid en/ectropion).
- Injuries penetrating the tarsal plate (ensure no obvious globe trauma prior to consultation).
- An injury to the upper lid dividing the levator palpebrae and causing ptosis.
- An injury in close proximity to the medial canthus for which there is concern for lacrimal duct involvement.
- Lid avulsions.
- Loss of extensive lid tissue/complex lacerations.
- Any periorbital laceration with adipose tissue exposure (concern for deep tissue injury or concomitant globe rupture if through the upper eyelid).1,5
Superficial lacerations to the eyelid may be repaired with 6-0 or 7-0 non-absorbable nylon or polypropylene simple interrupted sutures.
Complications/Disposition
Complications of laceration repair include iatrogenic injury secondary to local anesthesia injection/suture needle. All patients with should be referred to a specialist for aftercare.5
Lateral Canthotomy and Cantholysis
Trauma-induced hemorrhage is the most common precipitating factor for orbital compartment syndrome in patients presenting to the ED,24 however, several conditions may lead to the development of orbital compartment syndrome. Iserson, et al. provide an excellent chart in their Wilderness and Environmental Medicine publication:
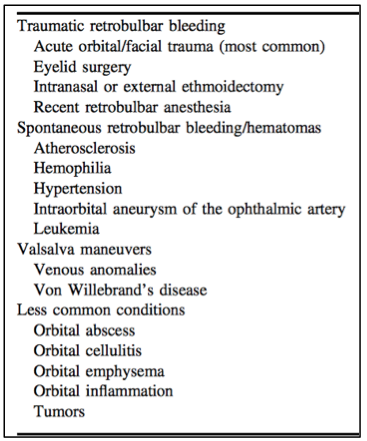
Causes of Orbital Compartment Syndrome24
In the setting of orbital compartment syndrome, the optic nerve and central retinal artery are compressed, resulting in ischemia and vision loss.1,24 Indications for lateral canthotomy and cantholysis include:
- Decreased visual acuity
- Ocular pressure >40 mm Hg
- Proptosis
- Afferent pupillary defect (Marcus Gunn pupil)
- Cherry-red macula
- Opthalmoplegia, optic nerve pallor
- Severe eye pain1,24
Roberts & Hedges provide a great procedural schematic depicted below. As the authors note, many practitioners will elect to perform a re-assessment of IOP after release of the inferior crus. If vision returns and the IOP is within normal limits, release of the superior crus is not required.1
Note: Physical assessment of proptosis and EOMs are much less reliable post-cantholysis, and do not indicated the resolution of the compartment syndrome.25
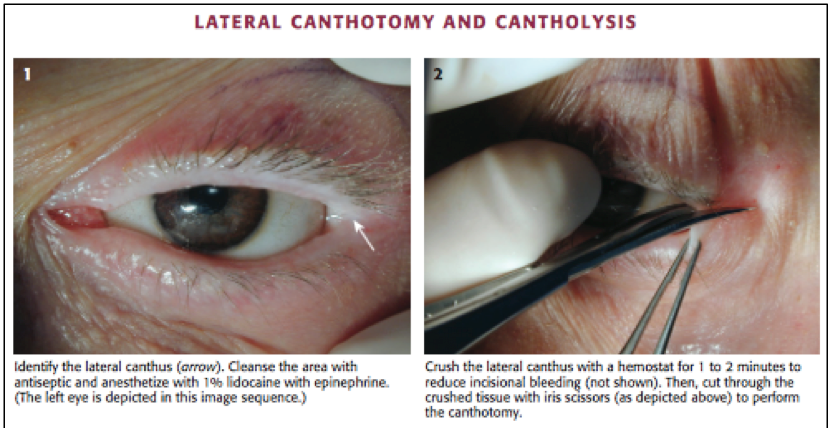
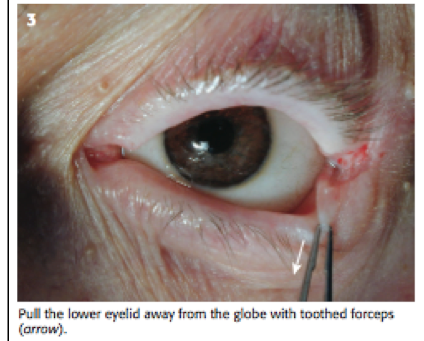
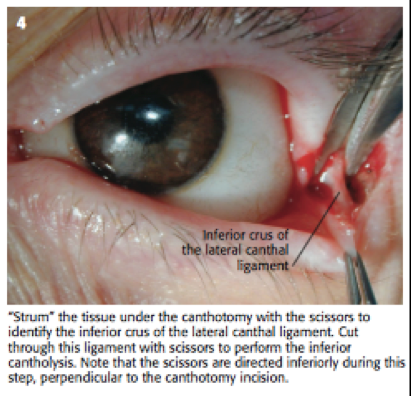
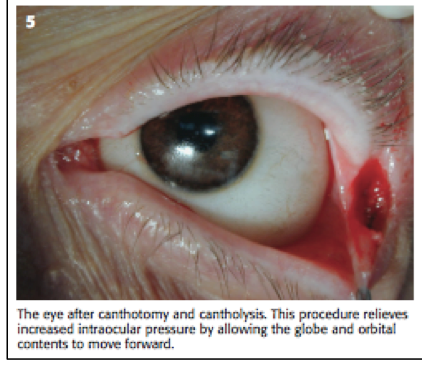
Performance of a Lateral Canthotomy and Cantholysis1
Complications
Instruments should be directed toward the orbital rim, tangential to the surface of the globe, to avoid iatrogenic EOM or globe injury.25
Disposition
All patients require emergent consultation with a specialist.1,25
Nose
Epistaxis Management
Information regarding the management of epistaxis can be found in a previous emDocs link:
http://www.emdocs.net/wp-content/uploads/2014/11/Epistaxis-Millsap-.pd
Keep your eyes open for the upcoming post: The Emergency Department Management of Posterior Epistaxis
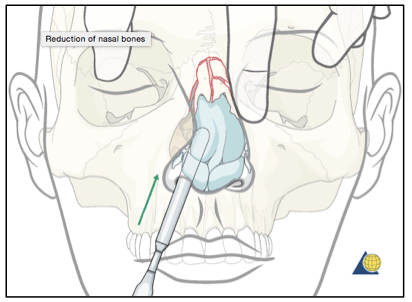
Nasal Bridge Fracture Reduction
This is generally not the emergency physician’s domain. The majority of fractures are not reduced until patient follow-up 3-7 days after initial injury to allow for swelling improvement.1 If imaging reveals complicated fractures or fractures involving the nasal septum, the patient should be referred to the appropriate specialist. If the patient has a simple nasal bridge fracture (unilateral fracture of the nasal pyramid), and has no concern about cosmetic outcome, despite discussion regarding poor outcome for impacted or greenstick fractures:
- Document and obtain written consent.
- Take a “before” photo for the medical record.
- Decide on a procedural sedation agent/sedate the patient.
- Elevate the depressed nasal bone using a scalpel handle.
- Use your opposite hand to manually displace the pyramid to midline.
- Take an “after” photo for the medical record.
Steps 4-6 are depicted in the figure below. An exterior splint should be applied to maintain the reduction.

Reduction of a Lateral Nasal Bridge Fracture26
Complications/Disposition
Complications include failed reduction, and nasal trauma secondary to the scalpel handle. All patients require follow-up for splint removal in 7-14 days. Antibiotics are not indicated.1
Nasal Septal Hematoma
Nasal septal hematomas occur due to trauma to the anterior portion of the nasal septum, and may be seen in the setting of nasal bridge fracture.1 Patients with septal hematomas present with pain, rhinorrhea, or difficulty breathing through the affected nares. Patients with subacute septal hematomas often present with fever and signs/symptoms consistent with infection (the retained blood serves as a medium for Staph and Strep species propagation).1 On visual inspection, septal hematomas may be detectable due to septal asymmetry.
In addressing a septal hematoma:
- Incise the mucosa horizontally over the mucosa after anesthesia is achieved (B).
- Excise a small amount of mucosa to avoid premature closure of the incision (C).
- Place a section of a sterile rubber band to act as a drain.
- Pack the nostril to re-approximate the perichondrium to the cartilage (D).1,27
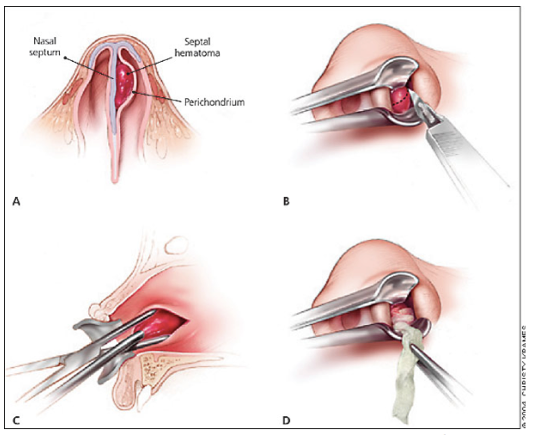
Drainage of a Nasal Septal Hematoma27
Complications/Disposition
Missed septal hematomas may result in infection (as above), septal perforation, or cartilage destruction resulting in a saddle-nose deformity.1,27 All patient should receive antibiotic therapy and should be referred for daily hematoma re-evaluation to ensure no additional blood accumulation. The affected nares should remain packed for 24 hours post hemostasis to ensure perichondrium attachment to the septal cartilage.1,27
Nasal Foreign Bodies
Approximately 0.1% of annual pediatric ED visits are for nasal FBs.28 While nasal FB are commonly encountered in the pediatric population, this diagnosis should also be considered in psychiatric and developmentally-delayed patients presenting with fever, nasal pain, purulent or bloody sinus drainage, or recurrent unilateral epistaxis.1 Imaging is generally not required in the setting of acute retained FB. Xrays or CT of the sinuses may be obtained in the evaluation of a chronically retained nasal FB.1
FBs may be removed using many of the same techniques mentioned under the auricular FB section: manual instrumentation and fogarty catheters/katz extractors. Posterior FBs often require positive pressure for removal. One such technique for the application of positive pressure is the “parent’s kiss” or “mother’s kiss” maneuver:

Parent’s Kiss Positive Pressure Technique29
- Mom tells the child that she is going to “give her a big kiss.”
- She quickly occludes the nostril opposite the FB.
- She makes a firm seal with her mouth over the child’s mouth and gives a short, sharp, puff of air into the child’s mouth, dislodging the object.1,29
Note: This technique may also be performed utilizing a BVM placed over the patient’s mouth, however, the sellick maneuver should performed during bag compression in order to avoid air entering the esophagus and subsequently the stomach.1
As with auricular FBs, sedation may be required to obtain patient cooperation. Oxymetazoline and topical lidocaine may also aid in FB removal – providing reduction of nasal turbinate edema and pain control.1
Complications/Disposition
Similar to auricular FBs, trauma to the nares and nasal mucosa may occur secondary to extraction attempts. All patients with retained nasal FBs require ENT referral.
Batteries require special attention; as previously mentioned, they quickly cause tissue damage. If unable to expediently remove a disc battery, ENT should be consulted immediately.1
Special Topics
Magnetic Nose Rings – be on the lookout for patients wearing bilateral magnetic nose rings. Magnets may become displaced with their polarization directed through the nasal septum, subsequently causing pressure necrosis of the nasal mucosa. Patients may present with nasal pain and purulent drainage which is mistaken for a simple sinusitis.1,30

Magnetic Nasal Ring31
Throat
Peri-Tonsillar Abscess (Quinsy) Needle Aspiration/Incision and Drainage
Peritonsillar abscesses (PTAs) are the most common deep space infections of the head and neck, and frequently occur in the second and third decades of life as sequelae of recurrent tonsillitis or inadequately treated tonsillitis.1,32 Spread of infection from the tonsil leads to a localized pus collection between the tonsillar capsule, the superior constrictor muscle, and the palatopharyngeus muscle.1 Patients often present with odynophagia, uvular deviation (away from the PTA), fever, +/- trismus.
Peritonsillar cellulitis is often times difficult to differentiate from a PTA, however, intraoral sonography improves diagnostic accuracy. 32
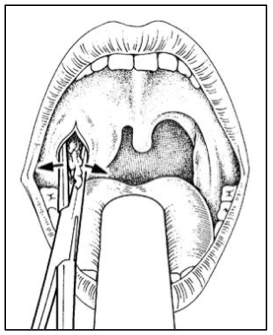
Needle Aspiration
- Obtain a long 18 or 20G needle, remove the cap and cut off the distal 1cm. Replace the cap.
- Anesthetize the posterior pharynx with topical lidocaine.
- Using a 27G needle, superficially inject 1-2cc lidocaine with epinephrine in the area to be aspirated (do not forget to draw back prior to aspiration; this aspect of the procedure is similar to creating a superficial weal).
- Using your previously prepared 18 or 20 gauge needle with the cut cap, attached to a 10-20cc syringe, advance the needle the 1cm distance in the sagittal plane and aspirate. 1
*Do not direct the needle laterally toward the carotid artery or jugular vein. If the superior pole of the tonsil is aspirated initially without pus obtained, the middle and inferior poles should be sequentially aspirated for pus return.1,32
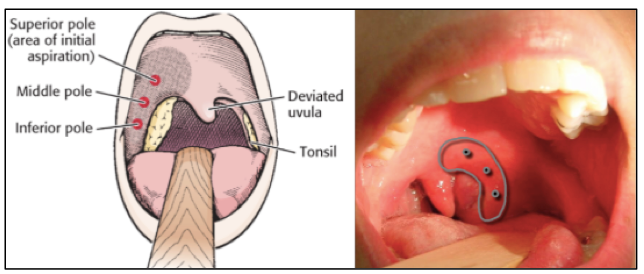
Sites of PTA Aspiration33
Incision and Drainage
- Anesthetize the posterior pharynx with topical lidocaine.
- Using a 27G needle, inject 1-2cc lidocaine with epinephrine in the area to be aspirated.
- Take a #11 or #15 blade and tape over ALL but the most distal 0.5cm of the blade to prevent deeper penetration.
- Incise the area of maximum fluctuance.
- Utilize suction while proving the incision with a closed Kelly clamp to break up loculations.
- Allow the patient to gargle with a saline or saline/dilute peroxide solution.
- Monitor for at least an hour to ensure hemostasis and PO tolerance.
- Home with antibiotics.1
Complications/Disposition
The carotid artery lies 2 cm posterolateral to the tonsillar pillar and is at risk for injury if the procedure is performed inappropriately. A failure rate of 10% occurs with aspiration/I&D. All patients requires 24-36 hour follow-up to ensure adequate drainage.1
Incision and Drainage of a PTA33
References / Further Reading
1. Roberts J, and Hedges J. (2010). Clinical Procedures in Emergency Medicine (5th ed.). Philadelphia, PA: W.B. Saunders
- Stone C, and Humphries R. (2012). Current Diagnosis and Treatment Emergency Medicine (7th ed.). McGraw-Hill.
- Nicks B, Ayello E, Woo K, Nitzki-George D, Sibbald R. Acute wound management: revisiting the approach to assessment, irrigation, and closure considerations. Int J Emerg Med. 2010; 3(4): 399-407.
- Zempsky W, Cravero J. Relief of pain and anxiety in pediatric patients in emergency medical systems. Pediatrics. 2004;114(5):1348–1356
- Sabatino, F and Moskovitz J. Facial wound management. Emerg Med Clin N Am. 2013; 31:529-538.
- Semer N. Practical plastic surgery for non-surgeons. Philadelphia: Haley and Belfus; 2001. p. 145-159.
- Forsch R. Essentials of skin laceration repair. Am Fam Physician. 2008; 78(8):945-951.
- Lin, M. The HAT trick. UCSF School of Medicine, Department of Pediatrics. 2013. Available from https://pediatrics.ucsf.edu/blog/hat-trick#.V1wVS3iJndk
- Ozturk D, Sonmez B, Altinbilek E, Kavalci C, Arslan E, et al. A retrospective observational study comparing hair apposition technique, suturing and stapling for scalp lacerations. World J Emerg Surg. 2013; 8:27.
- Hock O, Ooi S, Saw S, et al. Treatment of scalp lacerations with a hair apposition technique reduced scarring, pain, and procedure duration compared with suturing. Evid Based Med. 2003; 8:24.
- Hafner H, Rocken M, Breuninger H. Epinephrine-supplemented local anesthetics for ear and nose surgery: clinical use without complications in more than 10,000 surgical procedures. J Dtsch Dermatol Ges. 2005; 3(3):195-199.
- Krunic A, Wang L, Soltani K, Weitzul S, Taylor R. Digital anesthesia with epinephrine: an old myth revisited. J Am Acad Dermatol. 2004; 51(5):755-759.
- Chan T, Harrigan R, Ufberg J, Vilke G. Mandibular reduction. J Emerg Med. 2008; 34(4):435-440.
- Tesfaye Y, Skorzewska A, Lal S. Hazard of yawning. CMAJ. 1991; 145:1560.
- Littler B. The role of local anesthesia in the reduction of long-standing dislocation of the temporomandibular joint. Br J Oral Surg. 1980; 18:81-85
- Hutchens, D and Raghavendra M. Ear Anesthesia. Medscape. 2016. Available from: http://emedicine.medscape.com/article/82698-overview#a1
- Flores S and Herring A. Ultrasound-guided greater auricular nerve block for emergency department ear laceration and ear abscess drainage. J Emerg Med. 2016; 50(4):651-655.
- Lin B. Closing the gap, wound closure for the emergency practitioner. 2016. Available from: https://lacerationrepair.com/special-situations/ear-lacerations-part-ii/
- Marin J and Trainor J. Foreign body removal from the external auditory canal in a pediatric emergency department. Pediatric Emergency Care. 2006; 22(9): 630-632.
- Fritz S, Kelen G, Sivertson K. Foreign bodies of the external auditory canal. Emerg Med Clin North Am 1987;5:183-192.
- Medline. Katz Extractor. Oto-rhino foreign body remover. 2016. Available from: http://www.medline.com/product/Katz-Extractor-Oto-rhino-Foreign-Body-Remover-by-InHealth/Z05-PF30989
- Burke R, Gatton B, Melville L. Mastoiditis and meningitis complicating an aural foreign body. Pediatr Emerg Care. 2012; 28(10):1070-1071.
- Timm N, Iyer S. Embedded earrings in children. Pediatr Emerg Care. 2008; 24(1):31-33.
- Iserson K, Luke-Blyden Z, Clemans S. Orbital compartment syndrome: alternative tools to perform a lateral canthotomy and cantholysis. Wilderness Environ Med. 2016; 27:85-91.
- Rowh A, Ufberg J, Chan T, Vilke G, and Harrigan R. Lateral canthotomy and cantholysis: emergency management of orbital compartment syndrome. J Emerg Med. 2015; 48(3):325-330.
- Colton C, Krikler S, Schatzker J, Trafton P. AO surgery reference: lateral nasal bridge fracture. Available from: https://www2.aofoundation.org/wps/portal/surgery
- Kucik C, Clenney T, Phelan J. Management of acute nasal fractures. Am Fam Physician. 2004; 70(7):1315-1320.
- Kiger J, Brenkert T, Losek J. Nasal foreign body removal in children. Pediatr Emerg Care. 2008; 24(11):785-789.
- Deverill J. ENT gets up your nose. SCHemergency. 2015. Available from http://schemergency.com/stem/ent-gets-up-your-nose
- Mattu, A. (2011). Avoiding common errors in the emergency department. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins Health.
- Magnetic Nasal Ring. Bewild Company. 2016. Available from: https://www.amazon.com/Bewild-Brand-Magnetic-Clear-Stone/dp/B00E3B2G04
- Prokofieva A, Modayil V, Chiricolo G, Ash A, and Raio C. Ultrasound-guided drainage of peritonsillar abscess: shoot with your hockey stick. Intern Emerg Med. 2015. Published online.
- Prime Health Channel. Peritonsillar abscess and symptoms. 2015. Available from: http://www.primehealthchannel.com/peritonsillar-abscess-symptoms-pictures-drainage-and-treatment.html





2 thoughts on “HEENT: Tips for Addressing Your Next Procedure”
Pingback: Procedures! – Rapid On-Shift Learning for Emergency Medicine
Great review. For the mandibular dislocations, they don’t all need sedation. I have had great success with masseter massage. Well tolerated, no sedation needed, patients in and out of the ED in minutes.