
Author: Leah M. Bralow, MD (@lbralow, St. Barnabas Hospital, Bronx, NY; Affiliate Assistant Medical Professor, City University of New York School or Medicine) // Reviewed by: Jay Khadpe, MD (@resusjay); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case:
A 42-year-old female with no past medical history presents to the Emergency Department (ED) complaining of neck pain for 6 weeks. She has had persistent almost daily temperatures around 99F – 100F and 10 lbs of unintentional weight loss. Her pain is in the anterior neck and has gradually migrated from the right side, across the front, to the left side of her neck. Over the past week, she has begun to have the sensation of orthopnea and painful swallowing, triggering her presentation to the ED.
Vital Signs: BP 145/96, HR 115, RR 16, O2 sat 100%, T 100.2F
Exam reveals a very comfortable appearing patient with loss of a visible sternal notch and loss of sternocleidomastoid definition on the anterior neck. Palpation reveals fullness to the anterior lower neck and bilateral tenderness. No crepitus. Intraoral examination is normal and symmetric. Voice is full and patient is tolerating secretions. No stridor or wheezing.
Her workup reveals a significantly elevated thyroxine (T4), undetectable thyroid-stimulating hormone (TSH) and an ultrasound of the neck shows an enlarged thyroid with heterogeneous appearance bilaterally and decreased color doppler flow.
Background:
Thyroid hormones are essential for growth and development as well as daily functioning of the body. While they affect nearly every system, the most clinically relevant effects seen in the emergency department are due to stimulation of the cardiovascular, central nervous, and metabolic systems.
The thyroid gland is regulated through the hypothalamus-pituitary-thyroid axis. The hypothalamus releases thyrotropin-releasing hormone (TRH), which stimulates the anterior pituitary to release TSH. TSH then triggers the release of T4 and triiodothyronine (T3) from the thyroid gland. Approximately 80% of circulating hormone is T4. T4 is then converted to T3 at target cells and T3 is the active form of thyroid hormone. Both T4 and T3 provide negative feedback to the hypothalamus and pituitary.
Hyperthyroidism is a group of diseases, such as Grave’s Disease, in which the thyroid gland produces inappropriately high amounts of thyroid hormone. Hyperthyroidism is further categorized as subclinical hyperthyroidism and overt hyperthyroidism. As the names suggest, patients with subclinical hyperthyroidism have laboratory abnormalities without clinical effects and patients with overt hyperthyroidism are symptomatic. Typically, symptomatic patients have a very low or undetectable TSH and significantly elevated Free T4 outside of normal reference ranges.1, 2
Thyrotoxicosis refers to the spectrum of illness resulting from elevated circulating thyroid hormone levels. This spectrum ranges from mild symptoms to thyroid storm. Where any patient lies on this spectrum is a matter of clinical judgement. There are no definitive laboratory cutoffs that categorize severity of thyrotoxicosis or “rule in” thyroid storm.2-5
Thyrotoxicosis can result from any process which causes excessive release of thyroid hormone and is not limited only to diseases of hyperthyroidism such as Grave’s Disease. As a result, thyrotoxicosis is divided into two major categories: with hyperthyroidism and without hyperthyroidism (see Table 1). The most common cause of thyrotoxicosis with hyperthyroidism is Grave’s Disease followed by Toxic Multinodular Goiter and, rarely, Thyroid Adenomas.1-3, 5 These disorders involve intrinsic dysfunction of the thyroid gland resulting in overproduction of thyroid hormone. The second category, thyrotoxicosis without hyperthyroidism, consists of the “thyroiditis” diseases. In these cases, destruction of the thyroid gland causes unregulated release of pre-formed thyroid hormone from the cells, however the gland itself does not have abnormal or dysregulated production of hormone.1, 2 These differences will affect management.

Clinical Presentation: Mild to Moderate Thyrotoxicosis
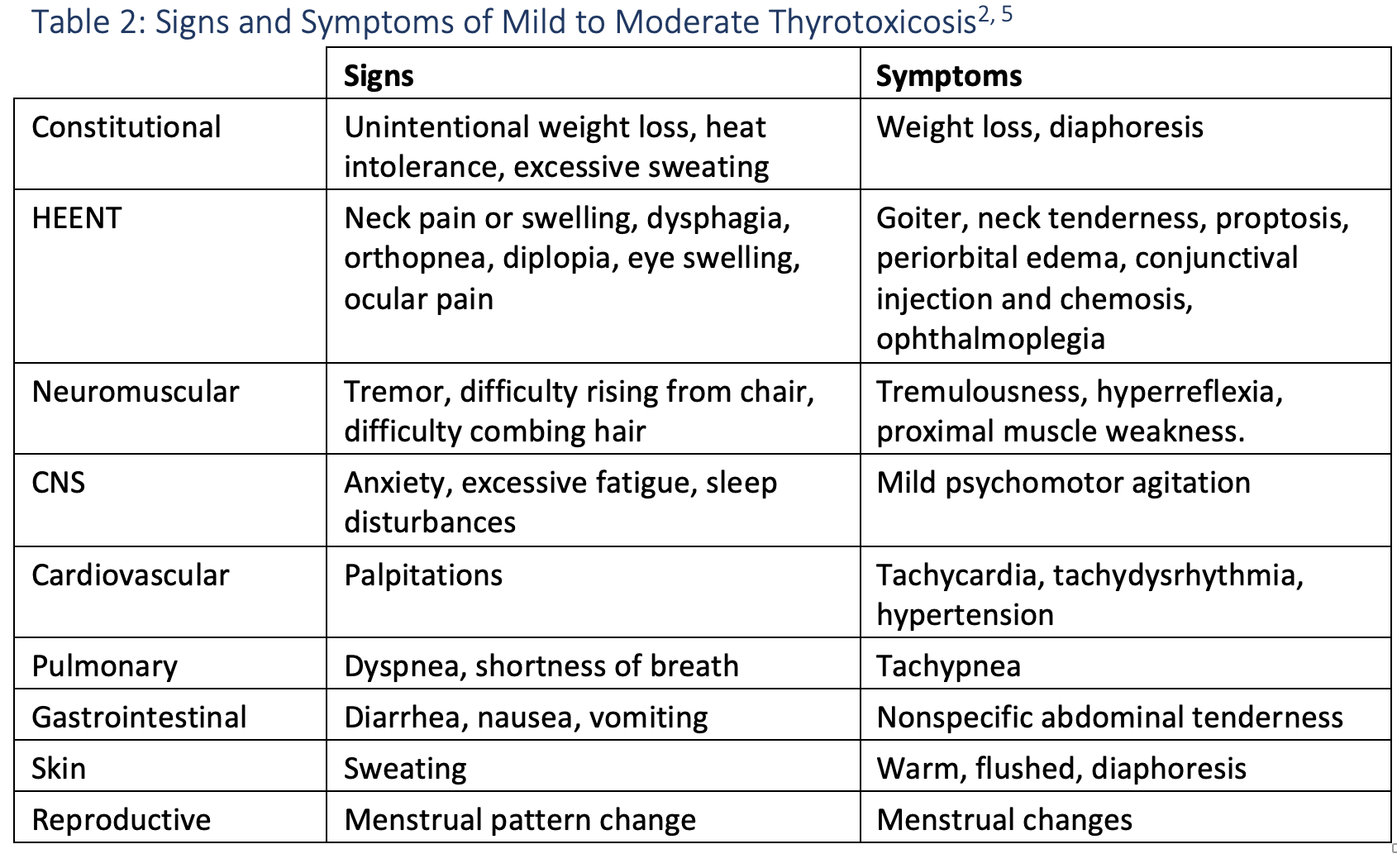
Patients with thyrotoxicosis have highly varied ED presentations and are often initially mis-diagnosed as either sepsis or sympathomimetic surge. Hallmarks of thyrotoxicosis are the presence of fevers, tachycardia out of proportion to clinical appearance, hypertension, and anxiety or tremulousness. Goiter is typically present, and the thyroid gland may be tender or nontender, depending on the underlying disease process (see Table 2).
Most thyrotoxic patients will have Grave’s Disease that is either undiagnosed, untreated, or the result of noncompliance with medical therapy. The majority are women who classically present with thyrotoxicosis, goiter, proptosis, and myxedema. Approximately 25% of patients with Grave’s Disease will present with Grave’s Orbitopathy consisting of the triad of proptosis, periorbital edema, and diplopia.1, 2 Grave’s Orbitopathy can progress to blindness and is treated primarily with glucocorticoids and urgent referral to ophthalmology and endocrinology.
Thyroiditis should be considered in all patients who do not have a previous diagnosis of Grave’s Disease. Many types of Thyroiditis exist with slight variations in clinical features (see Table 1). Patients with thyroiditis typically have a self-limited triphasic course. They often present to the ED in the first phase of illness, which is the thyrotoxic phase lasting for approximately three to six weeks. This is followed by a hypothyroid phase lasting up to six months. The majority of patients will return to a euthyroid state by 12 months after onset of illness.2
Due to the anatomic location of the thyroid gland, any patient reporting orthopnea, a globus sensation, or difficult or painful swallowing should have a careful evaluation of airway stability as all of these symptoms can result from compression of the trachea or esophagus due to goiter.2
Clinical Presentation: Thyroid Storm
Thyroid Storm is a medical emergency and represents the most severe form of thyrotoxicosis. Unfortunately, there is no single, unifying clinical definition of thyroid storm and there are no diagnostic laboratory findings or cutoffs. Patients frequently have a prior diagnosis of hyperthyroid disease, however, thyroid storm can be the initial clinical presentation for patients without known hyperthyroidism. Thyroid storm is a notorious mimic, and patients with thyroid storm are commonly initially misdiagnosed as sepsis or sympathetic overdrive. Even with prompt recognition and appropriate treatment, mortality from thyroid storm is estimated to be between 8 – 25%.2-7
Typically, patients present with high fever, tachycardia out of proportion to underlying illness and some form of CNS involvement ranging from agitation to delirium and coma. Deeper evaluation will reveal multisystem involvement.
Thyroid storm patients display a spectrum of CNS derangement from restlessness or anxiety through to coma. The majority of patients will show evidence of psychomotor agitation or delirium and may require treatment with benzodiazepines for symptom control.
The cardiovascular system is heavily involved in thyroid storm. Early in the disease course, patients may complain of dyspnea on exertion and palpitations. Cardiac rhythm can range from sinus tachycardia to tachydysrhythmias (most commonly atrial fibrillation). Physical examination may reveal hypertension with a widened pulse pressure. As thyroid storm worsens, patients can develop high-output heart failure. Late-stage patients progress to low-output heart failure and cardiogenic shock. Care must be taken to evaluate for the type of heart failure prior to initiation of β-blockade, as β-blockers are contraindicated in low-output cardiogenic shock states.
Metabolic derangements can become significant. Patients with thyroid storm can have core temperatures exceeding 104F. Increased gluconeogenesis and glycogenolysis as a result of elevated thyroid hormone levels can also lead to significant hyperglycemia. Finally, thyroid hormone stimulates bone breakdown resulting in hypercalcemia.
Patients may also present with profuse vomiting and severe diarrhea as a result of gastrointestinal (GI) involvement. The combination of insensible losses, electrolyte derangement and GI losses can lead to severe dehydration and acute kidney injury.5
Approximately 76% of patients with thyroid storm will have more than 3 major organ systems involved at the time of presentation and multisystem organ failure is the leading cause of death.4, 5 Liver failure and the presence of jaundice are late findings and are associated with particularly poor prognosis.3
Evaluation:
The evaluation of patients with suspected thyrotoxicosis or thyroid storm focuses on identification of the trigger, medical stabilization, and regulation of both circulating thyroid hormone levels and thyroid hormone effects. In patients with mild disease, categorization of type of thyroid disease can aid in tailoring therapy and preventing inappropriate long-term use of antithyroid drugs.
All patients with suspected thyrotoxicosis should undergo hormone evaluation in the ED. Free T4 is used as a surrogate measure of the amount of active thyroid hormone in circulation and TSH is used to evaluate the integrity of the HPT axis. Thyrotoxic patients will have a very low or undetectable TSH with a Free T4 above the normal range. Rarely, a patient with a pituitary tumor secreting unregulated TSH will have high TSH and high T4. Some laboratories will also report Free T3, which is useful only when differentiating exogenous ingestions of a thyroid hormone product from intrinsic disorders. There are no defined diagnostic laboratory cutoffs for thyrotoxicosis or thyroid storm. These diagnoses are made based upon clinical judgement in the presence of laboratory-confirmed hyperthyroidism.
A careful evaluation for the stressor causing the patient’s decompensation must be undertaken. The most common stressor is infection.3, 6 Other potential triggers include (but are not limited to) surgery, neck trauma, myocardial infarction, stroke, and diabetic ketoacidosis. Long-term use of certain drugs can also cause thyroiditis. Amiodarone, Lithium and Interferon-α are major triggers of thyroiditis with delayed onset after months to years of chronic use. A significant portion of patients with thyrotoxicosis will have a known hyperthyroid state and have inappropriate medication use or medication noncompliance. Despite careful analysis, approximately 30% of patients who have thyroid storm will not have a diagnosable precipitant.3, 6
CT scan of the soft tissues of the neck without IV contrast should be considered in any patient complaining of orthopnea, hoarseness, a globus sensation in the throat, or difficulty swallowing as goiter can cause compression of the trachea and esophagus.
In stable patients who do not already have a diagnosed thyroid disease, a thyroid ultrasound with color doppler can provide useful information (see Table 1). 8 In most cases, ultrasound imaging can be deferred to the inpatient team or outpatient setting unless clinical concern for compromise of mediastinal structures exists. Where ultrasound cannot be obtained, a CT scan of the soft tissues of the neck can be obtained, however note that IV contrast contains iodine, which may worsen certain types of thyrotoxicosis and can precipitate thyroid storm as discussed previously here on EM Docs.9
Patients with clinical evidence of severe illness and hemodynamic instability have thyroid storm. In 1993, Burch and Wartofsky developed and published a score (Table 3) to establish diagnostic criteria for thyroid storm.10 Due to the rarity of this disease, the score has not been externally validated, however it is widely used as an adjunct to clinical judgement for diagnosis. Values greater than 45 are considered to support a diagnosis of thyroid storm. Scores between 25-44 are considered suggestive of thyroid storm, but not diagnostic. Scores less than 25 indicate that thyroid storm is unlikely, however the patient may still be suffering from thyrotoxicosis requiring treatment.

General Management Considerations:
For patients who have thyrotoxicosis without thyroid storm, therapy consists primarily of β-blockers for thyroid hormone-related symptoms and NSAIDs or glucocorticoids for pain control and inflammation.1, 2, 5 Patients with moderate thyrotoxicosis and associated vital sign abnormalities should be admitted to the hospital with endocrinology consultation for initiation of therapy and monitoring until symptoms start to improve. It is estimated that 1-5% of patients admitted with thyrotoxicosis will progress to thyroid storm.2
The initiation of Antithyroid drugs (ATDs) such as propylthiouracil or methimazole in the ED may be considered for any patient with thyrotoxicosis until the type of thyroid disease has been determined. ATDs are a cornerstone therapy for thyrotoxicosis with hyperthyroidism. Patients who have thyrotoxicosis without hyperthyroidism (e.g. thyroiditis or exogenous thyroid hormone administration) can have ATDs stopped as these patients do not have dysregulated production of hormone and therefore ATDs are not indicated.1, 2
Management: Thyroid Storm
Thyroid Storm is a true medical emergency with mortality ranging from 8-30% despite early recognition and aggressive management.3, 6, 11 Rapid recognition, diagnosis of the trigger, and a comprehensive approach to treatment are critical. The first and most important aspect of treatment is appropriate resuscitation with intravenous fluids, temperature control, benzodiazepines for CNS effects, evaluation of cardiac status, and electrolyte correction. Aggressive supportive care is vital to the treatment of these patients.
Targeted therapies in thyroid storm address three key mechanisms: 1) Block thyroid hormone effects, 2) decrease circulating thyroid hormone, and 3) treat the trigger. The order in which therapy is administered is important in treating thyroid storm and can be remembered as “ABC WI.” (“ABC Wisconsin”, see Table 4)
- Antithyroid Drug
- Beta Blocker
- Corticosteroid
- Wait > 1 hour
- Iodine
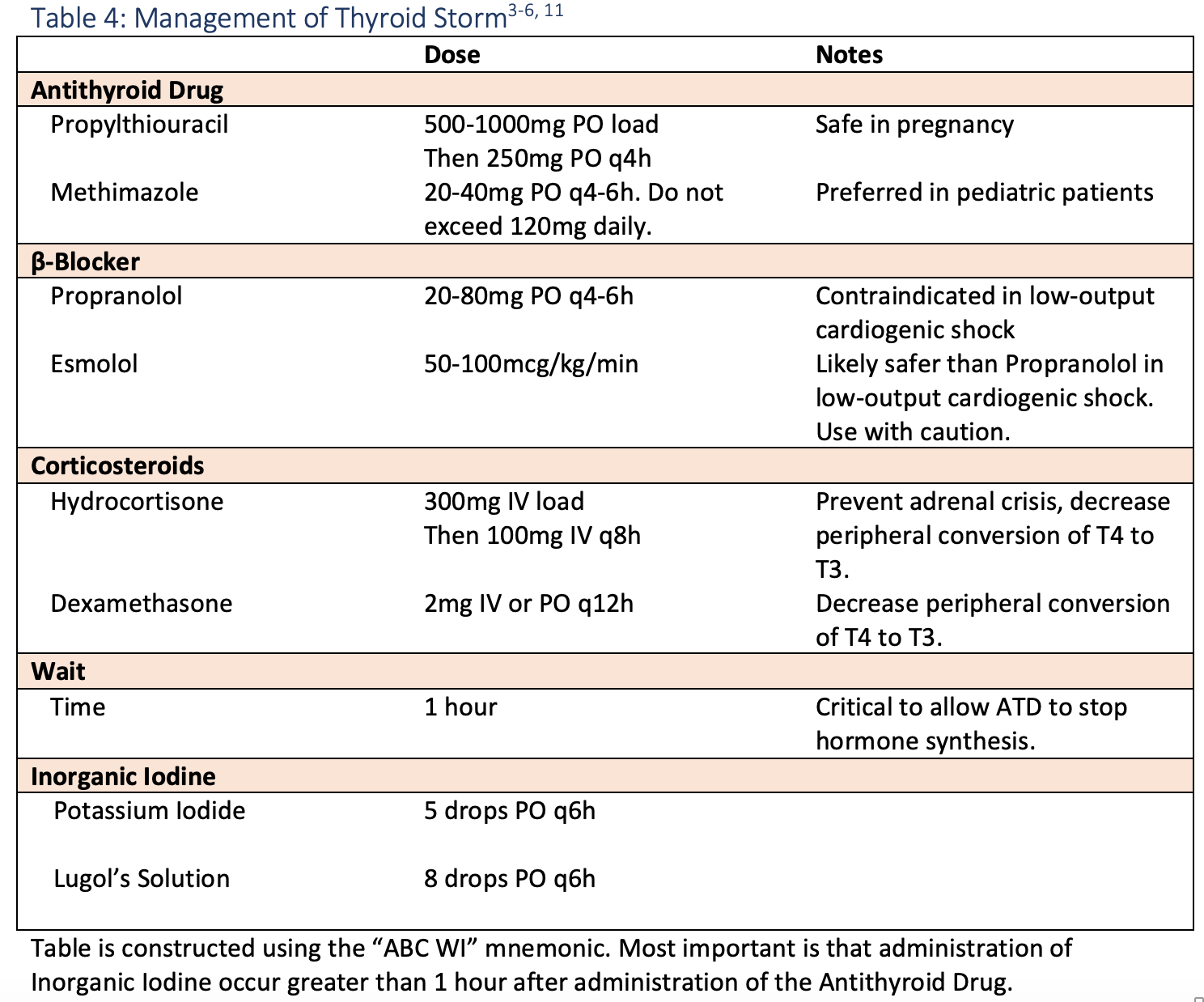
ATDs are the thionamides. Most commonly used are Propylthiouracil (PTU) and Methimazole. These drugs inhibit thyroid peroxidase (TPO) in the thyroid gland thereby preventing the formation of T3 and T4. PTU has an additional benefit of also inhibiting peripheral conversion of T4 to T3. PTU is safe for the management of hyperthyroidism in pregnancy, however, its use is contraindicated in children1. Methimazole is the preferred ATD in pediatric patients.1
β-blockers such as Propranolol are first line agents for thyroid storm. Propranolol not only blocks the downstream effects of thyroid hormone as a nonselective inhibitor of α- and β-adrenergic receptors, but also blocks conversion of T4 to T3 in the tissues. β-blocker therapy is clinically targeted to decreasing hormone effects, not normalization of vital signs. Esmolol can be used as an alternative to Propranolol because of its IV formulation and highly titratable nature. Note that β-blockers are contraindicated in low-output heart failure states and therefore a bedside echocardiogram should be performed prior to initiation of β-blocker therapy.
Stress-dose hydrocortisone is administered to treat concomitant adrenal insufficiency, which has a high rate of occurrence with thyroid storm.4, 6 Both Hydrocortisone and Dexamethasone have the additional benefit of blocking peripheral conversion of T4 to T3.
The next “medication” in treating thyroid storm is a classic “tincture of time”. Wait at least 1 hour after administering the ATD before giving the final medication, inorganic iodine.
Iodine, in the form of Potassium Iodide solution or as Lugol’s Solution, should be administered last. Small amounts of iodine administration typically increase thyroid hormone release, however, overloading the receptors with Iodide will have the paradoxic effect of decreasing thyroid hormone release, known as the Wolff-Chaikoff Effect.6 It is vitally important to stop hormone synthesis before Iodide administration.
Disposition:
Any patient in which goiter is causing voice changes, difficulty swallowing, orthopnea, a globus sensation, or otherwise impacting mediastinal structures on imaging should be admitted for airway monitoring during treatment.
All patients with thyrotoxicosis should receive an endocrinology consultation, as the majority will require hospitalization for monitoring while treatment takes effect. At the discretion of endocrinology, a select subset of the mild and clinically stable thyrotoxicosis patients can have treatment initiated in the ED and then be managed as outpatients. These patients must be able to receive close outpatient follow-up and be reliable to return to the ED for worsening symptoms.
All patients with thyroid storm must be admitted, typically to the ICU.
Patients with subclinical hyperthyroidism can be discharged home with PCP and/or endocrine follow-up and return precautions. Treatment does not need to be initiated in the Emergency Department.
Take Home Points:
- Hyperthyroidism represents a broad spectrum of disease from subclinical, which requires no ED intervention, to thyroid storm, a life-threatening medical emergency.
- There are no specific laboratory “cutoffs” that define thyroid storm. This is a clinical diagnosis. The Burch-Wartofsky score can help support clinical gestalt.
- There are a myriad of Thyroiditis syndromes which are caused by a destructive process to the thyroid gland. These diseases are self-limited and are not associated with true hyperthyroidism. As such, treatment focuses on symptom management with β-blockers and pain control with NSAIDs.
- Thyroid storm treatment can be remembered as “ABC WI”: Antithyroid Drugs, β-Blockers, Corticosteroids, Wait 1 hour, Iodine.
- The first step in managing a patient with thyroid storm is aggressive supportive care.
Case Resolution:
Endocrinology is consulted. Her history, laboratory and ultrasound evaluation are most suggestive of subacute thyroiditis, however, she is endorsing new orthopnea and difficulty swallowing. Further evaluation of the airway is obtained with computed tomography (CT) scan of the neck. CT scan shows diffuse subacute thyroiditis and an acute suppurative thyroiditis to the left lobe with phlegmon extension into the deep tissues of the left neck. The patient has 4mm rightward deviation of the trachea and esophagus due to asymmetric goiter. She is started on antibiotics, Methimazole 20mg TID, Propranolol 20mg q6h, Hydrocortisone 300mg IV bolus followed by 100mg q8h and Potassium Iodide 5 drops TID pending further evaluation for possible underlying Grave’s Disease. She is admitted for further observation and diagnostic evaluation.
Ultimately, her evaluation shows no evidence of Grave’s Disease or other underlying hyperthyroid state. This patient represents a classic case of thyrotoxicosis without hyperthyroidism, and her final diagnosis is that of Subacute Thyroiditis with overlying Acute Suppurative Thyroiditis. Antithyroid drugs and iodine therapy are stopped by endocrinology on hospital day #3. She is discharged home after four days on β-blockers, NSAIDs, and antibiotics with close outpatient endocrinology follow-up.
From Dr. Katy Hanson at Hanson’s Anatomy:

Further Reading:
- Ross D, Burch H, Cooper D, Greenlee M. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid. 2016 Oct 2016;26(10)doi:10.1089/thy.2016.0229
- De Leo S, Lee S, Braverman L. Hyperthyroidism. The Lancet. 2016-08-01 2016;388(10047):906-918. doi:10.1016/s0140-6736(16)00278-6
- Chiha M, Samarasinghe S, Kabaker A. Thyroid storm: an updated review. Journal of intensive care medicine. 2015 Mar 2015;30(3)doi:10.1177/0885066613498053
- Cimino-Fiallos N. Thyroid EmergenciesIn: Mattu A and Swadron S, ed. CorePendium. CorePendium LLC. Accessed December 30, 2020. https://www.emrap.org/corependium/chapter/reczuGCKanuAFIt5c/Thyroid-Emergencies.
- Devereaux D, Tewelde S. Hyperthyroidism and thyrotoxicosis. Emergency medicine clinics of North America. 2014 May 2014;32(2)doi:10.1016/j.emc.2013.12.001
- Farkas J. Thyroid Storm In: the Internet Book of Critical Care. 2017.
- Mackey C. Quality Corner: Thyroid Storm and Aortoiliac Occlusive Disease. Accessed December 12, 2020. http://www.emdocs.net/quality-corner-thyroid-storm-and-aortoiliac-occlusive-disease/
- Chaudhary V, Bano S. Thyroid ultrasound. Indian journal of endocrinology and metabolism. 2013 Mar 2013;17(2)doi:10.4103/2230-8210.109667
- Bodford I. EMDocs Handout Thyroid Storm. Accessed December 12, 2020. http://www.emdocs.net/wp-content/uploads/2015/01/ThyroidStorm-Bodford-.pdf
- Burch H, Wartofsky L. Life-threatening thyrotoxicosis. Thyroid storm. Endocrinology and metabolism clinics of North America. 1993 Jun 1993;22(2)
- Awad N. Thyroid Storm: Treatment Strategies. Accessed December 30, 2020. https://www.aliem.com/thyroid-storm-treatment-strategies/




