
Authors: Joel Hamm, MD (University of KentuckyDepartment of Emergency Medicine); Anasemon Aioub, PharmD (University of Kentucky Department of Pharmacy); James Warwick (University of Kentucky College of Medicine) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
A 14-year-old male with history of Type 1 Diabetes Mellitus presents with nausea, vomiting, abdominal pain, polyuria, and polydipsia for last 2 days. The pain is constant, nonlocalized, and vomiting is nonbloody, nonbilious. Blood sugar has read “HI”. Of note, his mother states he had an insulin pump placed 1 week ago, and they do not understand how it works.
Initial vitals: T 37.2, HR 130, BP 110/60, Sat 99%, RR 32.
When you arrive in the room, he is uncomfortable, toxic appearing with Kussmaul breathing. On abdominal exam, he has mild tenderness diffusely without guarding or rebound tenderness. The insulin pump is located in the right lower quadrant, with mild edema around the insertion site. As you leave the room, you wish you were up-to-date on insulin pumps, as there is no endocrinologist on call at your hospital.
Besides standard DKA treatment, how do you manage this patient with an insulin pump? Why does he have edema at the insertion site? What education can you provide the family?
Background
The utilization of insulin pumps, or continuous subcutaneous insulin infusion (CSII), has been on the rise for the management of both Type 1 and Type 2 Diabetes. While significant improvements in insulin pump technology have been made over the past decade, a surprising number of complications still arise.1
Insulin Pump Anatomy
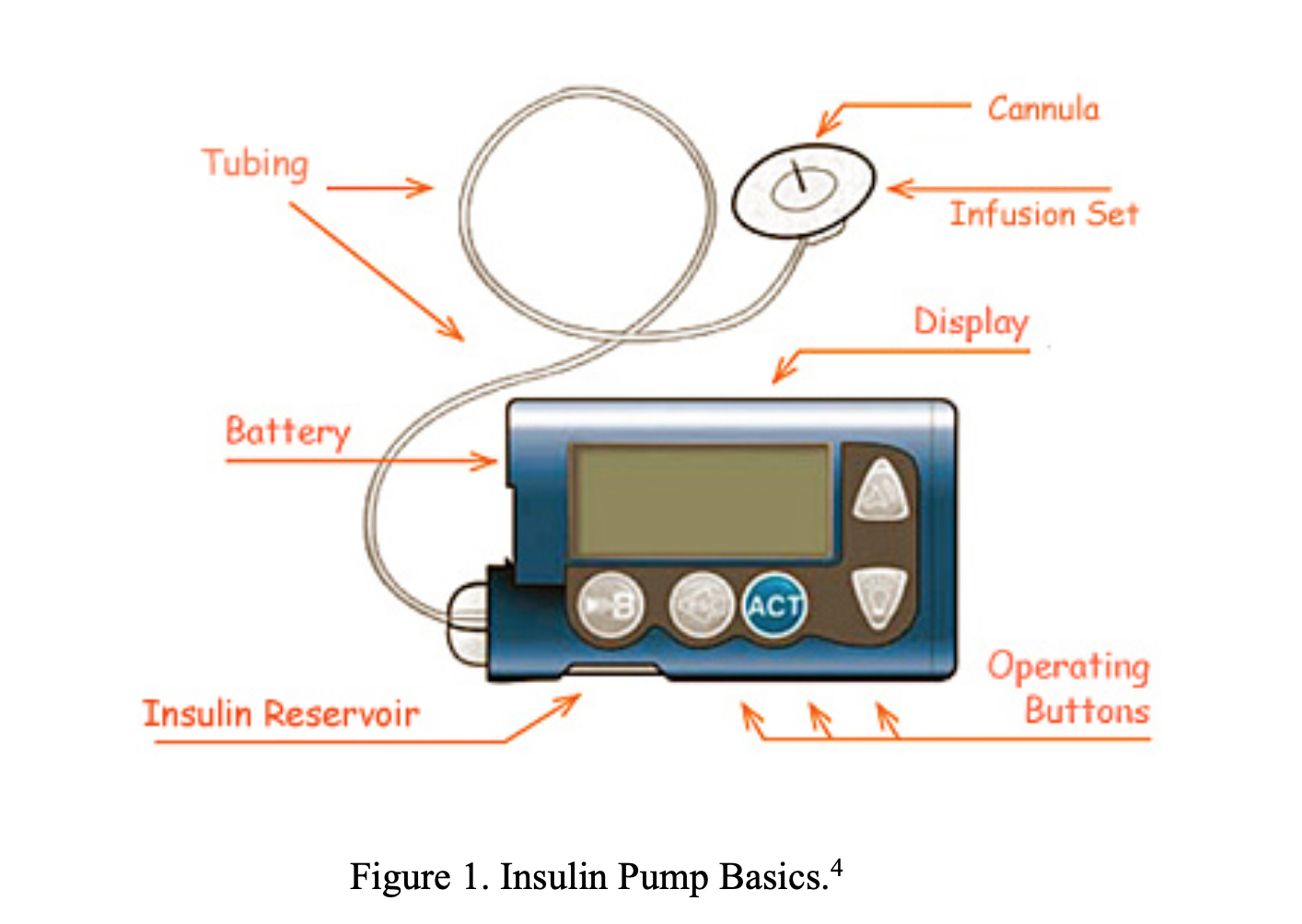
Insulin pumps consists of a reservoir, a pump, and an infusion set.2 The reservoir holds a 2-3 day supply of regular or short-acting insulin2 the battery-powered pump encases the reservoir, and the infusion set consists of tubing (typically smaller in diameter than normal IV tubing) that connects the reservoir to a subcutaneous cannula. Patients insert the needle into their skin and secure the infusion set with an adhesive to allow for medication delivery.3 The most common site for needle insertion and insulin infusion is the abdominal wall, although other infusion sites can be used, including the outer thigh, arms, hips, and buttocks. These alternative sites typically have slower insulin absorption.3
Insulin pump software can be calibrated to individualize insulin delivery to the patient based on that patient’s needs, activity levels, food intake, and time of day, typically delivering a continuous basal rate of insulin along with preset boluses before meals. Recent models integrate the insulin pump with a continuous glucose monitoring patch, which can further fine-tune the pump’s insulin output throughout the day.2,5
Insulin Pump Complications
Insulin pump complications can be broadly divided into two categories: those that develop from insulin pump therapy itself, and those that develop from pump malfunctions. The vast majority of complications can be corrected independently and do not require hospitalization, but a high number of complications continue to require emergency department care.
Complications from Insulin Pump Therapy
The most common complications of insulin pump therapy involve the skin and soft tissue. These are usually direct results of CSII therapy and are typically milder in presentation. Skin and soft tissue complications can include any of the following:
- Local insulin reactions: These are particularly common at the beginning of insulin therapy. Newly diabetic patients can have cutaneous allergic reactions or edema while the body adjusts to the tighter glycemic control provided by the insulin pump. The majority of these local reactions are harmless and do not require treatment, but can certainly worry patients.6,7
- Lipohypertrophy and lipoatrophy: These are a direct result of insulin action in tissues.6,7 Areas of focal lipohypertrophy may appear to be an abscess and mistakenly diagnosed as such. These areas are often associated with focal scarring. If lipohypertrophy occurs, patients should be instructed to change insertion site and avoid that area for 3 to 4 weeks to allow healing.8
- Scarring: This can occur from any continued subcutaneous infusion. To minimize scarring, the infusion set should be inserted at 90 degrees. Previously scarred areas should be avoided during infusion set placement as they can impair insulin absorption.7
- Cellulitis: This is a historically common side effect.6 Infections with Streptococcus and Staphylococcus sp. are often precipitated by poor site preparation before insertion. If infection occurs, the area should be cleaned and the infusion site should be changed. Topical and/or systemic antibiotics may be required depending on the severity of the infection. Abscesses near the insulin pump infusion site should be drained and cultured to guide antibiotic therapy.8
Insulin pump users are recommended to switch infusion sites every 48-72 hours to avoid local skin reactions and other skin and soft tissue complications.7
Complication from Insulin Pump Malfunctions
As described, the insulin pump is a complex therapeutic system. Battery failure, kinked tubing, reservoirs leaking, software malfunctioning, or needles slipping can all cause pump failure and lead to severe metabolic disturbances. Many insulin pumps have various alarms and reminders to alert the patient to low battery, low cartridge, time to test blood glucose, and even dangerous glucose levels.9 However, many insulin pump alarms will not detect insulin leakage or will detect dangerous glucose levels too late to avoid metabolic disturbances.7 The most urgent complications of insulin pump therapy are Diabetic Ketoacidosis (DKA) and Hypoglycemia.
Diabetic Ketoacidosis
- Definition: DKA is characterized by the classic triad of hyperglycemia, ketosis, and metabolic acidosis. It is the result of a relative or absolute deficiency of insulin, and an excess of counter-regulatory hormones, resulting in hyperglycemia. Hyperglycemic crises can be classified as either DKA or Hyperglycemic Hyperosmolar State (HSS), however, HSS rarely presents as an acute complication of insulin pump therapy.10
- Precipitating Factors: With insulin pumps, the most common precipitating events are catheter dislodgement or infusion tubing occlusion during sleep. Less commonly, DKA can result from inadequate site changes and impaired insulin absorption.7
- Diagnosis: Serum glucose > 250 mg/dL (> 200 mg/dL in pediatric patients), Serum bicarbonate < 15 mEq/L, pH < 7.3, Anion Gap > 12, Ketonemia or ketonuria.
- Management in Setting of Insulin Pump:
- Turn off the pump once IV access is established!
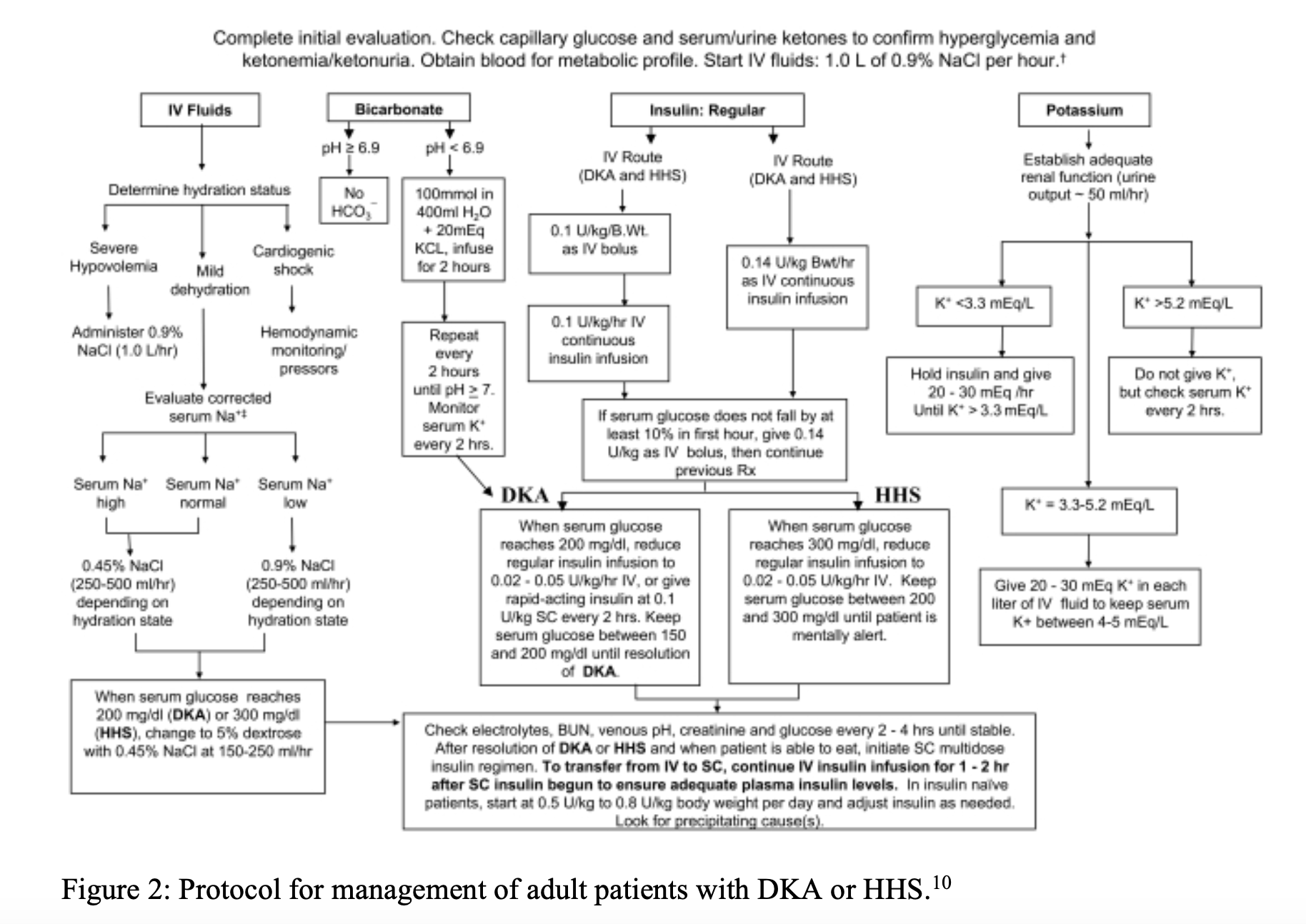
- IV Fluids, Potassium, Bicarbonate (consider if pH < 6.9): standard management as per ADA treatment algorithm in Figure 2.10
- Insulin: Insulin therapy should be withheld until the serum potassium is > 3.3 mEq/L. Premature insulin administration can precipitate hypokalemia due to intracellular shifts.10,11 The patient’s insulin pump should be turned off as soon as an IV is established as glycemic control for these patients is best attained using IV therapy. Make sure the pump is completely shut down and turned to OFF. It is typically not necessary to remove the insertion needle in the acute setting, as doing so may result in misplacement or damage of the pump.
- Begin insulin at a continuous infusion rate of 0.1-0.14 unit/kg/hour (0.05-0.1 units/kg/hr for pediatric patients).10,12
- Following DKA resolution, insulin infusion should be scaled back to the patient’s normal basal rate.1,10
- Importantly, patients with Type 1 DM always require physiologic insulin dosing to prevent recurrence of DKA. The use of a correctional (sliding) insulin scale as sole therapy is associated with worse glycemic control.5,10
- Physiologic insulin therapy includes a basal insulin infusion rate, mealtime insulin boluses, and correctional insulin as needed. In the acute setting, correctional and basal insulin should be given as outlined, with a transition back to the patient’s normal pump infusion protocols.
- Transitioning back to CSII
- DKA resolution criteria:
- serum glucose <200 mg/dL
- bicarb >15 mEq/L
- pH >7.3
- Anion gap <12
- Once ketoacidosis has been resolved, subcutaneous insulin therapy can be re-implemented. However, it is important to allow a 1-2 hour overlap between IV therapy and administration of subcutaneous therapy to prevent rebound hyperglycemia and complication.10
- DKA resolution criteria:
Hypoglycemia
- Definition: Serum glucose less than 70 mg/dL. Severe hypoglycemia is a common occurrence of insulin pump therapy in Type 1 Diabetes, and to a lesser extent Type 2 Diabetes.13
- Precipitating Factors: Most often, hypoglycemic episodes are associated with bedtime infusion set changes along with an insulin correction bolus, with no subsequent monitoring.7 Hypoglycemia can also result from inadequate carbohydrate consumption, excessive exercise, or improper dosage adjustment. The net result is excess insulin relative to the patient’s glucose levels. Type 1 Diabetics are completely dependent on exogenous insulin for glycemic control, but over time also lose the ability to effectively release glucagon and other regulatory hormones.13,14 This leaves Type 1 Diabetics at high risk for hypoglycemia; they have no ability to compensate for too much insulin.
- Hypoglycemic Unawareness (HU): Recurrent episodes of hypoglycemia can blunt the body’s response to low blood glucose. The result is that episodes of hypoglycemia beget more episodes. This can decrease the symptom severity, masking hypoglycemia and increasing the risk for hypoglycemic episodes to develop into severe events. This is defined as the onset of neuroglycopenia before the appearance of sympathoadrenal symptoms.14

- Clinical Presentation
- Sympathoadrenal: Palpitations, tachycardia, diaphoresis, general malaise
- Neuroglycopenic: Confusion, lightheadedness, blurred vision, slurred speech, seizures, coma13
- Symptoms can be non-specific and are not required for the diagnosis of hypoglycemia, but severe hypoglycemia should be proven by fulfillment of Whipple’s Triad:13
- Symptoms consistent with hypoglycemia
- Measured low plasma glucose
- Resolution of symptoms after glucose levels are raised
- Diagnosis
- Serum glucose < 70 mg/dL
- Severe hypoglycemia is typically defined as a blood glucose < 54 mg/dL with symptoms15
- Management in Setting of Insulin Pump
- Mild Hypoglycemia (BG > 54 mg/dL): The 15-15 rule should be applied. Give the patient 15 grams of oral carbohydrates (half a cup of apple juice, half a sandwich, or 4 or 5 pieces of hard candies) and check the serum glucose after 15 minutes. Repeat as necessary.5
- Severe Hypoglycemia (BG < 54 mg/dL with symptoms): Feed as above if alert and able to tolerate by mouth and turn insulin pump to OFF.11,15
- If unable to feed patient…
- IV 50% Dextrose, 15-20g
- Glucagon IM if neuroglycopenic symptoms
- Monitor closely for rebound hyperglycemia
Prevention of Insulin Pump Complications
Prevention of both DKA and hypoglycemia from insulin pump complications revolves around patient education.5,16 It is important to emphasize early recognition and frequent blood glucose monitoring to patients and families, and to provide them with resources to prevent metabolic episodes in the future.
- Monitor frequently! Insulin pump users should monitor their blood glucose levels before and after meals, before and after exercise, and before bed at a minimum.5
- Patients should change infusion site every 2-3 days to decrease the risk of severe complications. Infusion site failures increase after 3 days of catheter use.7
- Most insulin pump manufacturers offer free education materials related to the technical aspects of their devices, and can replace device hardware if damaged. Patients should check with their insurance to see if replacement parts are covered.
- UpToDate offers a wealth of patient education materials endorsed by the ADA, split into two categories, “The Basics” and “Beyond the Basics.” UpToDate’s entries on insulin pumps give comprehensive overviews of insulin pump usage and technology, with more detailed information under the “related topics” tab.
- Pumps are not a replacement for a functioning pancreas. Patients still need to exercise careful glucose intake and make appropriate dosing adjustments per a pre-set plan. Upon resolution of DKA or hypoglycemia the patient should meet with the clinician managing their diabetes as an outpatient to fine tune their therapy program.
- Many community health systems have offered training programs and local support for insulin pump users.16 Pharmacists can become certified diabetes educators or certified pump trainers for insulin pump companies, allowing them to implement CSII support to DM patients.9 Make sure your patients are aware of the resources available to them.
Future of Insulin Pumps
- Many insulin pumps on the market today are associated with a glucometer or continuous glucose monitor (CGM). These are termed “closed loop” insulin pumps; systems that use continuous real time glucose levels to adjust dosage rather than adhering to a preset basal rate and calculated boluses.2 Closed loop systems are meant to better mimic physiologic pancreas activity and have the potential to improve patient adherence and glycemic control. However, closed loop systems still have limitations, including delays in response times, accurate signal feedback, software malfunctions, high cost, and user errors.9
- Other technological advances are being integrated into insulin pump therapy, including smartphone applications, Bluetooth compatibility, and data sharing.9 Research involving biological models of insulin therapy, including nanopolymer-mediated insulin delivery and pancreatic islet regeneration, are currently being investigated and may provide improved therapy options for diabetic patients in the future.17,18
Take Home Points
- Failure of any component part of the insulin pump cause complications, ranging from local skin reactions to severe metabolic disturbances. Bedtime infusion complications are the most common culprit for both DKA and hypoglycemia.
- Recurrent hypoglycemia blunts the normal counterregulatory response in patients with type 1 DM and can mask the early warning signs of hypoglycemic episodes. Careful blood glucose monitoring is key in the setting of insulin pumps!
- Patient education is essential for prevention of insulin pump complications.
References/Further Reading:
- Tran TTT, Pease A, Wood AJ, et al. Review of Evidence for Adult Diabetic Ketoacidosis Management Protocols. Front Endocrinol (Lausanne). 2017;8:106. Published 2017 Jun 13. doi:10.3389/fendo.2017.00106
- Reece S, Williams C. Insulin Pump Class: Back to the Basics of Pump Therapy Diabetes Spectrum 2014; vol. 27 no. 2.
- Pickup, JC. Insulin-pump therapy for type 1 diabetes mellitus. New England Journal of Medicine. 2012;366(17), 1616-24.
- Joseph, Josh. “Insulin Pumps: Understanding them and their complications. Endocrine-Metabolic, ALiEM. 2013.
- Chiang JL, Kirkman MS, Laffel LM, Peters AL, Type 1 Diabetes Sourcebook Authors. Type 1 diabetes through the life span: a position statement of the American Diabetes Association. Diabetes Care. 2014;37(7):2034-54.
- Hayek A, Robert A, Al Dawish M. Skin-Related Complications Among Adolescents With Type 1 Diabetes Using Insulin Pump Therapy. Endocrinology and Diabetes. 2018; 11:1-5.
- Ross P, Milburn J, Reith D, Wheeler B Clinical review: insulin pump-associated adverse events in adults and children. Acta Diabetol 2015;52: 1017-1024.
- Saboo BD, Talaviya PA. Continuous subcutaneous insulin infusion: practical issues. Indian J Endocrinol Metab. 2012;16(Suppl 2):S259-S262.
- Kessinger H, Knezevich E, DeSimone E, Davidian M. Pumping it up: new advancements in insulin delivery. U.S. Pharmacist 2017.
- Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. 2009;32(7):1335-43.
- Laufgraben M, Kaufman S. Acute Diabetic Emergencies, Glycemic Control, and Hypoglycemia. Critical Care Medicine: Principles of Diagnosis and Management in the Adult. 2014.
- Wolfsdorf JI, Glaser N, Agus M, et al. ISPAD Clinical Practice Consensus Guidelines 2018: Diabetic ketoacidosis and the hyperglycemic hyperosmolar state. Pediatr Diabetes. 2018;19(Suppl 27):155-177.
- Tsai SH, Lin YY, Hsu CW, Cheng CS, Chu DM. Hypoglycemia revisited in the acute care setting. Yonsei Med J. 2011;52(6):898-908.
- Martín-Timón I, Del Cañizo-Gómez FJ. Mechanisms of hypoglycemia unawareness and implications in diabetic patients. World J Diabetes. 2015;6(7):912-26.
- International Hypoglycemia Study Group. Glucose Concentrations of Less Than 3.0 mmol/L (54 mg/dL) Should Be Reported in Clinical Trials: A Joint Position Statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2017;40(1):155-157.
- Boyd LC, Boyd ST. Insulin pump therapy training and management: an opportunity for community pharmacists. J Manag Care Pharm. 2008;14(8):790-794.
- Gu Z, Aimetti AA, Wang Q, et al. Injectable nano-network for glucose-mediated insulin delivery. ACS Nano. 2013;7(5):4194-201.
- Huising MO, van der Meulen T, Vaughan JM, et al. CRFR1 is expressed on pancreatic beta cells, promotes beta cell proliferation, and potentiates insulin secretion in a glucose-dependent manner. Proc Natl Acad Sci U S A. 2009;107(2):912-7.
- Seaquist ER, Anderson J, Childs B, Cryer P, Dagogo-Jack S, Fish L, Heller SR, Rodriguez H, Rosenzweig J, Vigersky R. Hypoglycemia and diabetes: a report of a workgroup of the American Diabetes Association and the Endocrine Society. Journal of Clinical Endocrinol Metabolism. 2013;98(5):1845-59.
- Cryer PE, Axelrod L, Grossman AB, et al. Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinol Metabolism. 2009; 94:709.




