Authors: Anthony Scoccimarro, MD and Muhammad Waseem, MD, MS (Emergency Physicians, Lincoln Medical & Mental Health Center, Bronx New York) // Editors: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit, EM Resident at SAUSHEC, USAF)
BACKGROUND
One of the functions of an emergency department (ED) is to screen patients for preventable causes of harm. Harm itself may take on many forms from inherited or acquired disease states to the ill effects of social interaction. Intimate partner violence (IPV) falls into the latter category and is defined by the CDC as any physical, sexual, or psychological harm by a current or former partner or spouse.1 IPV affects more than 32 million Americans, more frequently involving women than men.2 Globally, intimate partners are responsible for greater than one out of seven homicides overall and one in three female homicides.3 The consequences of IPV are broad, from the physical to psychological. It has been linked to an increased risk of cardiac disease, asthma, and alcoholism.4 The emergency physician in particular has a unique opportunity to identify patients who are victims of IPV, as many IPV patients may have limited medical contact.
SCREENING
Although there are several populations that may be at higher risk, IPV should be considered whenever there are historical inconsistencies or physical findings incongruent with a proposed mechanism. There are numerous screening tools that have been shown to be effective, including HITS (Hurt Insult Threaten Scream), the AAS (Abuse Assessment Screen), and the OAS (Ongoing Abuse Screen).5 As an example, consider the HITS assessment:6
How often does your partner:
Physically hurt you?
Insult you or talk down to you?
Threaten you with harm?
Scream or curse at you?
In patients presenting to a family practice, this questionnaire was found to be 86% sensitive and 99% specific.6 Despite this success, a meta-analysis of several of these screening tools has found that the sensitivities and specificities of each vary widely and that no single tool is superior.7 In this regard, the vital step lies in choosing one specific survey rather than none at all.
The United States Protective Services Task Force updated its recommendations in 2013 to a grade B level of evidence for screening all women of child-bearing age, meaning there is moderate benefit. However, there remains insufficient evidence for the screening of elderly or vulnerable adults.8
HISTORY
Common presenting complaints include physical (difficulty with ambulation, dizziness, gynecologic symptoms), psychological (depression, suicidality, eating disorders), and somatic (irritable bowel syndrome, musculoskeletal pain).2 According to the American Congress of Obstetricians and Gynecologists, 2 out of 3 adolescent mothers on public assistance who are affected by IPV experienced birth control sabotage by a partner.9 IPV itself was also three times more likely among women seeking abortion than among their counterparts who chose to continue the pregnancy.9
Beyond the physical, there is a growing amount of evidence strengthening the association between IPV and mental illness, especially eating disorders. In a systematic review, Bundock, et al. discussed several studies demonstrating this relationship. This includes a survey by Jonas, et al. who found an increased risk of IPV among both men and women with eating disorders, with an odds ratio of 4.8 and 9.2, respectively.10 There has yet to be any evidence of causality between IPV and mental illness, but the associations are well-known.
PHYSICAL EXAMINATION
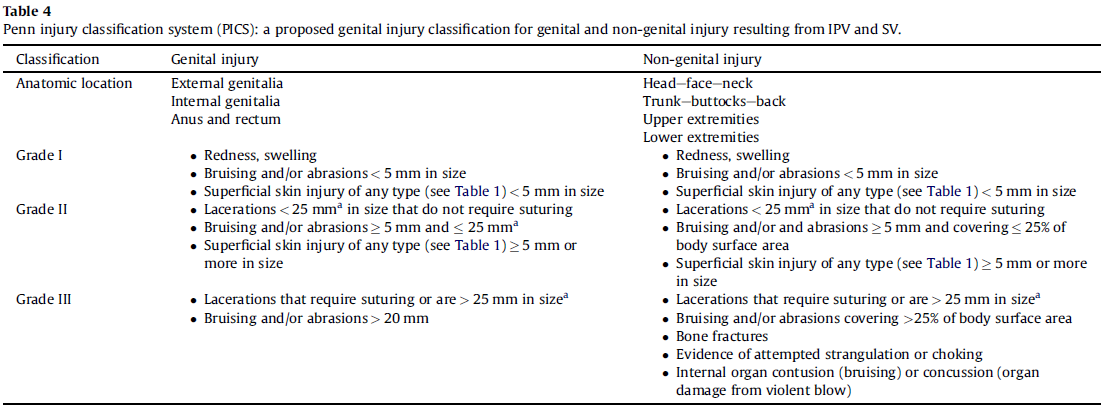
The physical examination can be seen as a double-edged sword when it comes to IPV. Although not all violence is physical (e.g. psychological abuse), even physical abuse may result in limited physical exam findings. This lack of forensic evidence can delegitimize the event for the victim when not contextualized appropriately. One of the more popular typological systems is TEARS (Tears, Ecchymosis, Abrasions, Redness, Swelling), which is more applicable to genital trauma.11 Sommers, et al. discussed how even this system is not widely accepted, noting a lack of uniformity. In addition, these grading systems do not necessarily reflect the degree of force or trauma involved.11 Despite this, Sommers ultimately does recommend the Penn Injury Classification System (PICS) for IPV and sexual violence (SV), as demonstrated by the following table:
As has been the case with survey tools, none of these classification systems has been shown to be superior to any other and they also require further validation before one can be definitively recommended.
INTERVENTIONS
Once you have identified an at-risk patient, what can you offer them? ED interventions should focus on identification of those at risk, education, safety, referral, and prevention. Educational materials may take many forms including brochures, online resources from the CDC and WHO, and more recently, phone apps such as the ASPIRE news app, which disguises itself as a news application.12 These interventions should be based on the services offered by your institution in coordination with your social work and nursing staff. Resources may include, but are not limited to, referrals to shelters, support groups, hotlines, and legal aid. Each of these components may play a role in constructing a safe discharge plan prior to patient disposition. It is important that this information is disseminated with discretion and that the perpetrators of IPV are not directly confronted.
Besides out-of-hospital resources, the clinician is also able to intervene directly. In addition to education on safety planning and discreet methods of contraception such as IUDs and Depo injections, harm-reduction strategies have been shown to reduce coercion pregnancies by 71% of women who experienced IPV.9 The clinician may also offer testing for STIs (including HIV), since this population has reported a higher frequency of risk factors.13 In general, there have been a number of studies which have demonstrated that interventions in IPV have resulted in significant reduction of IPV, improvement in health, safety-promoting behaviors, and the use of community-based resources.4
SUMMARY
– Screen all women of child-bearing age
– Consider adopting a standard questionnaire, e.g. HITS
– The physical examination does not rule out IPV
– Interventions are effective – determine what resources your institution has to offer
– Safe discharge is a team effort
References / Further Reading:
- Centers for Disease Control and Prevention. Intimate Partner Violence: Risk and Protective Factors. Atlanta: Centers for Disease Control and Prevention: 2010. Accessed at http://www.cdc.gov/ViolencePrevention/intimatepartnerviolence/riskprotectivefactors.html on 20 April 2015
- Weil, Amy. Intimate Partner Violence: Diagnosis and Screening. In: UpToDate, Fletcher, Suzanne (Ed), UpToDate, Waltham, MA. Accessed on April 30, 2015.
- Stöckl, Heidi, et al. “The global prevalence of intimate partner homicide: a systematic review.” The Lancet 382.9895 (2013): 859-865.
- Bair-Merritt, Megan H., et al. “Primary Care–Based Interventions for Intimate Partner Violence: A Systematic Review.” American journal of preventive medicine 46.2 (2014): 188-194.
- McFarlane J, Parker B, Soeken K, Bullock L. Assessing for abuse during pregnancy. Severity and frequency of injuries and associated entry into prenatal care. JAMA 1992; 267:3176
- Sherin, Kevin M., et al. “HITS: a short domestic violence screening tool for use in a family practice setting.” FAMILY MEDICINE-KANSAS CITY- 30 (1998): 508-512.
- Rabin, Rebecca F., et al. “Intimate partner violence screening tools: a systematic review.” American journal of preventive medicine 36.5 (2009): 439-445.
- Final Recommendation Statement: Intimate Partner Violence and Abuse of Elderly and Vulnerable Adults: Screening. U.S. Preventive Services Task Force. December 2014. Accessed at http://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/intimate-partner-violence-and-abuse-of-elderly-and-vulnerable-adults-screening
- The American College of Obstetricians and Gynecologists, Committee on Health Care for Underserved Women. Reproductive and sexual coercion. Committee Opinion Number 554. February 2013.
- Bundock, Louise, et al. “Prevalence and risk of experiences of intimate partner violence among people with eating disorders: A systematic review.” Journal of psychiatric research 47.9 (2013): 1134-1142.
- Sommers, Marilyn S., et al. “Injuries from intimate partner and sexual violence: Significance and classification systems.” Journal of forensic and legal medicine 19.5 (2012): 250-263.
- Weil, Amy. Intimate Partner Violence: Intervention and patient management. In: UpToDate, Fletcher, Suzanne (Ed), UpToDate, Waltham, MA. Accessed on April 30, 2015.
- Jannone, Laura. “Community services for victims of interpersonal violence.” Nursing Clinics of North America 46.4 (2011): 471-476.
- http://www.ncbi.nlm.nih.gov/pubmed/26004851
- http://www.ncbi.nlm.nih.gov/pubmed/25533139
- http://www.ncbi.nlm.nih.gov/pubmed/25282121
- http://www.ncbi.nlm.nih.gov/pubmed/25671018
- http://www.ncbi.nlm.nih.gov/pubmed/25421993
- http://www.ncbi.nlm.nih.gov/pubmed/23870859





1 thought on “Intimate Partner Violence – An Emergency Department Perspective”
Pingback: Asynchronous Learning: Psychiatric, Abuse, and Special Situations - Bold City Emergency Medicine