Authors: Nour Sinno, MD (EM Resident Physician, Department of Emergency Medicine, Western Michigan University Homer Stryker M.D. School of Medicine, Kalamazoo, Michigan) and Glenn Ekblad, DO, MSN (EM Attending Physician, Department of Emergency Medicine, Western Michigan University Homer Stryker M.D. School of Medicine, Kalamazoo, Michigan) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UT Southwestern Medical Center / Parkland Memorial Hospital) and Brit Long, MD (@long_brit)
A 51 y/o female presents to the ED with a 3-day history of fevers, chills, and sore throat. She states her voice has become hoarse and has developed worsening shortness of breath over the past few hours. She has not had any drooling.
VS: T: 100.7, HR 104, RR 24, BP 152/75, SpO2 97% on room air.
Physical exam: Patient sitting upright in mild distress. There is an audible inspiratory stridor. Neck is supple, without trismus. Erythema present in the oropharynx. Uvula midline, no tonsillar exudate.
What is the highest priority diagnosis?
How would you verify the diagnosis?
When do you decide to intubate this patient?
What additional therapy would you provide for this patient?
What is the disposition?
Background
- Epiglottitis is acute inflammation of the epiglottis and other supraglottic structures that can lead to airway obstruction in severe cases.1
- Etiologies include infectious causes as well as noninfectious causes such as thermal injuries, foreign body ingestion, and caustic ingestion.
- Haemophilus influenzae used to be the most common pathogen prior to the development of the Hib vaccine. Now, common pathogens include Streptococcus pneumoniae, Staphylococcus aureus, and beta-hemolytic streptococci.10
- Due to immunizations against Haemophilus influenzae serotype b, epiglottitis has decreased in the pediatric population over the past several decades. As a result, more cases are now seen in adults, most notably between ages 45 to 64 and those older than 85 years.1
- Those at risk for epiglottitis include middle aged white men, patients with a smoking history, infants younger than 1 year old, elderly older than 85, unvaccinated children, and those with comorbid conditions such as diabetes.1
Differential diagnosis: viral syndrome, pharyngitis, laryngitis, foreign body ingestion, caustic ingestion, angioedema, croup, anaphylaxis, peritonsillar abscess, and retropharyngeal abscess.1,3
Physical Exam
- Classic signs include toxic appearance, febrile, tachypneic, tachycardic, inspiratory stridor, muffled voice, drooling, tripod position, sniffing position, suprasternal, and/or subcostal retractions.3
- However, patients can present with widely varying symptoms.
Evaluation and Management
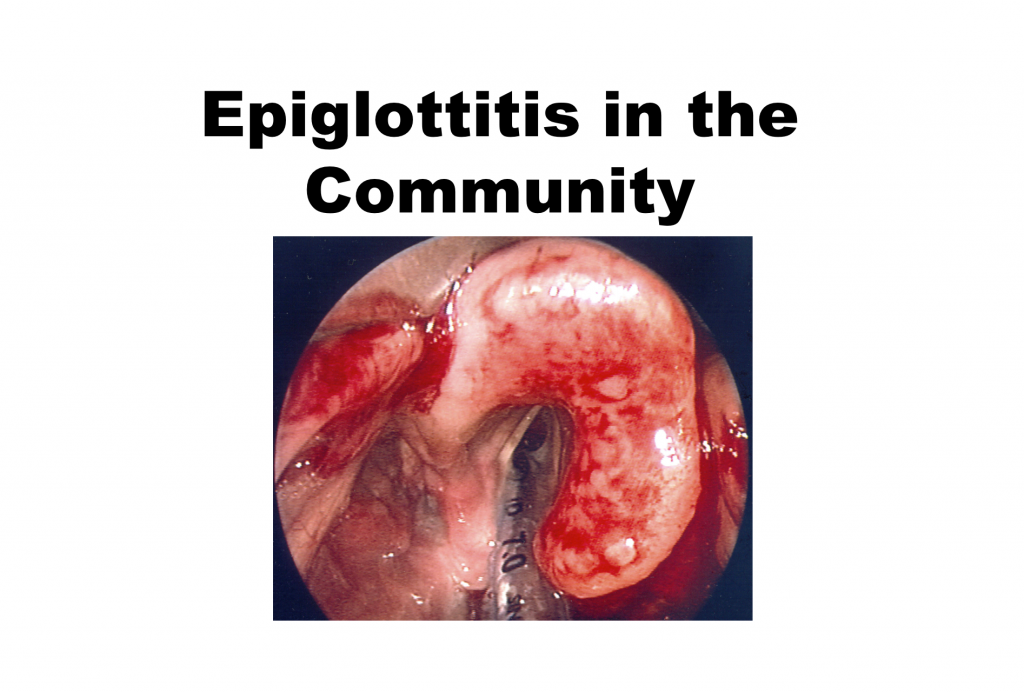
- Diagnosis is clinical and confirmed with laryngoscopy.
- Patient should remain in position of comfort. Avoid agitation as it may precipitate airway obstruction. Examination with a tongue blade is not recommended as it may cause agitation.
- If respiratory distress or stridor is present, prepare for intubation. Tachycardia, tachypnea, dyspnea, and rapid onset of symptoms are predictive factors for impending airway intervention.8
- Intubation should be performed in the OR if the patient is stable for transport. For unstable patients, awake fiberoptic intubation is recommended with a surgeon and an anesthesiologist present at bedside.8 Intubation should be attempted by the most experienced physician present.
- If intubation is unsuccessful, perform emergent tracheostomy or cricothyrotomy
- Below is a recommended checklist for immediate identification and management of a potential difficult airway with possible imminent complete airway obstruction.
- Recognition of a possible “significant airway obstruction” at triage or via EMS. The patient should immediately be moved to a major resuscitation room, and an appropriate team assembled, which may include emergency medicine, ENT, anesthesiology, possibly a trauma surgeon, and the difficulty airway cart to the bedside.
- Immediate evaluation of the patient in the ED by the attending physician. Some facilities may move the patient directly to the OR for the airway evaluation.
- Complete the initial focused Hx and PE, while simultaneously connecting the patient to all monitoring equipment, start a minimum of one IV, and provide for supplemental O2.
- When anesthesiology is available, they may provide topical oral-pharyngeal analgesia for videolaryngoscopy evaluation of the epiglottis.
- Surgical equipment must be at the patient bedside to facilitate a surgical airway, should it be needed.
- Rapid sequence intubation medications must be drawn up, and ready to be given in the event of a rapid deterioration of the patient’s airway. A smaller ET tube may be necessary for successful intubation.
- Medications for awake nasal fiberoptic or video intubation include: ketamine 1 mg/kg IV titrated to effect or fentanyl 1 microgram/kg and/or midazolam (Versed) 0.1 mg/kg titrated in 1 to 2 mg increments to effect. Awake intubation should be at the direction of the individual with the most extensive training and experience in the procedure. This is usually accomplished by an anesthesiologist, who is familiar with topical analgesia of the tongue, pharynx, and epiglottis.
- Consider racemic epinephrine aerosol while preparing for upper airway endoscopy.
- Begin IV antibiotics (CHECK FOR PATIENT ALLERGIES). A third generation cephalosporin (ceftriaxone, 50 mg/kg up to 2 grams IV) and vancomycin (15 mg/kg for concern for MRSA).
- Provide steroids (Decadron 0.1 mg/kg up to 10 mg IV).
- Disposition: All patients with a Dx of Acute epiglottitis, with or without intubation, are admitted to the ICU.
- If the patient must be transported from a small facility to a larger facility, the patient’s airway should secured prior to transport. If the patient has a known structural abnormality in the distal trachea, such as distal tracheal stenosis, the decision to transfer with or without having an endotracheal tube placed prior to transport must be discussed with the receiving ICU physician.
Imaging
- Laryngoscopy is the most accurate method to establish the diagnosis.
- Lateral soft-tissue radiograph of the neck is 88% sensitive.2
- Image findings include a swollen epiglottis termed “thumb sign,” thickened aryepiglottic folds and narrowed epiglottic vallecula.2 Absence of the “thumb sign” does not exclude the diagnosis.
- Diagnostic imaging should not delay airway intervention in those in respiratory distress.1
- CT of the neck, ultrasound, and MRI are generally not necessary in the evaluation of epiglottitis.3
Laboratory Studies
- CBC (may see leukocytosis), Chem-7, blood cultures.
- Obtain labs (CRP, ESR), cultures from epiglottis, and any abscess I&D once airway is secured.
Treatment
- Airway management is the main priority
- Supplemental O2
- Antibiotics
–3rd generation cephalosporins such a Ceftriaxone 1-2 g IV daily; 100 mg/kg for pediatric dose q12hrs or cefotaxime 2 g q12 hrs; 150 mg/kg/day q8hrs for pediatric dose or ampicillin/sulbactam 3 g four times daily; 200-300 mg/kg for pediatric dose q6hrs PLUS vancomycin 15 mg/kg q12 hrs; 40-60 mg/kg 3-4 times daily for pediatric dose 11,12,13 (add vancomycin if sepsis or meningitis is suspected or if patient is from an area of increased prevalence of MRSA).
–Trimethoprim- sulfamethoxazole is an acceptable alternative in patients with PCN allergy.14 320 mg IV initially, then 4-5mg/kg q12hr;13 15-20 mg/kg/day divided doses q6hrs for pediatric dosing.15
- Role of steroids is unsubstantiated in acute epiglottitis but may be used as an adjunct.8
Pearls
- Epiglottitis is a true airway emergency. Maintain a high clinical suspicion as presenting symptoms are variable and delayed diagnosis can have devastating consequences.1
- If airway obstruction is imminent, patient should be directly transported to the OR, or advanced airway equipment should be made readily available.3
- Stridor in a patient is the clinical finding which identifies patients needing emergent intubation. Airway management resources should be readily available for the entire duration of the patient’s ED stay.10
- Early ENT and anesthesiology consultation is critical (if available).10
- Greater than 50% occlusion is recommended in the literature (consensus decision) as a finding that establishes the need for intubation.
This post is sponsored by www.ERdocFinder.com, a supporter of FOAM and medical education, who with their sponsorship are making FOAM material more accessible to ER physicians around the world.

References/Further Reading:
- Lindquist B, Zachariah S, Kulkarni A. Adult epiglottitis: A case series. Perm J 2017;21:16-089. DOI: https://doi.org/10.7812/TPP/16-089.
- Takata M, Fujikawa T, Goto R. Thumb sign. Acute epiglottitis. BMJ Case Reports. 2016; 2016.http://ezproxy.med.wmich.edu/login?url=http://search.proquest.com/docview/1793825034?accountid=160899. doi: http://dx.doi.org/10.1136/bcr-2016-214742.
- Adil EA, Adil A, Shah RK. Epiglottitis. Clinical Pediatric Emergency Medicine. 2015;16(3):149-153. http://ezproxy.med.wmich.edu/login?url=http://search.proquest.com/docview/1714335421?accountid=160899. doi: http://dx.doi.org/10.1016/j.cpem.2015.07.005.
- Darras KE, Roston AT, Yewchuk LK. Imaging Acute Airway Obstruction in Infants and Children. RadioGraphics 2015; 35:2064-2079. https://www.ncbi.nlm.nih.gov/pubmed/26495798
- Zoorob R, Sidani MA, Freemont RD, et al. Antibiotics use in Acute Upper Respiratory Tract Infections. American Family Physician. 2012;86(9): 817-822. http://www.aafp.org/afp/2012/1101/p817.pdf
- Hartman ND. Neck and Upper Airway. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e New York, NY: McGraw-Hill; 2016. http://accessemergencymedicine.mhmedical.com.ezproxy.med.wmich.edu/content.aspx?bookid=1658§ionid=109387281. Accessed May 22, 2017.
- Qazi IM, Jarar AM, Hadi KAA, Hussain Z. Acute epiglottitis: A retrospective review of 47 patients in Kuwait. Indian J Otolaryngol Head Neck Surg. 2009; 61: 301-305. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3450074/pdf/12070_2009_Article_87.pdf
- Cirilli, A. R. (2013). Emergency evaluation and management of the sore throat. Emergency Medicine Clinics of North America, 31(2), 501-515. doi:10.1016/j.emc.2013.01.002
- Gonzalez MN, Weston B, Yuce TK, et al., One-Year experience with the institution of a critical airway team at an academic Medical Center. J. of Emergency Medicine. 2016; 50(1): 194-197.http://www.jem-journal.com/article/S0736-4679(15)00941-5/pdf
- Richards, A. M. (2016). Pediatric respiratory emergencies. Emergency Medicine Clinics of North America, 34(1), 77-96. doi:10.1016/j.emc.2015.08.006
- Bradley, John S., John D. Nelson, and MD, Joseph B. Cantey. 2015 Nelson’s Pediatric Antimicrobial Therapy, 21st Edition, pg 55, edited by John S. Bradley, et al., American Academy of Pediatrics, 2015. ProQuest Ebook Central, https://ebookcentral.proquest.com/lib/wmichlib-ebooks/detail.action?docID=1977785.
- Schaider, J. (2015). Epiglottitis, Pediatric. ROSEN & BARKIN’S 5-MINUTE EMERGENCY MEDICINE CONSULT. Retrieved May 29, 2017 from https://www-r2library-com.ezproxy.med.wmich.edu/Resource/Title/1451190670/ch0005s5861
- Schaider, J. (2015). Epiglottitis, Adult. ROSEN & BARKIN’S 5-MINUTE EMERGENCY MEDICINE CONSULT. Retrieved May 29, 2017 from https://www-r2library-com.ezproxy.med.wmich.edu/Resource/Title/1451190670/ch0005s5829
- Irwin, R. (2012). SUPRAGLOTTITIS (EPIGLOTTITIS). Irwin and Rippe’s Intensive Care Medicine. Retrieved May 29, 2017 from https://www-r2library-com.ezproxy.med.wmich.edu/Resource/Title/160831183X/ch0067s2010
- Hauser, A. (2013). APPENDIX 2 Dosing of Antibacterial Agents in Children. Antibiotic Basics for Clinicians. Retrieved May 29, 2017 from https://www-r2library-com.ezproxy.med.wmich.edu/Resource/Title/1451112211/ap0002





2 thoughts on “Management of Epiglottitis in the Community Setting”
Pingback: emDOCs.net – Emergency Medicine EducationEM@3AM - Epiglottitis - emDOCs.net - Emergency Medicine Education
Pingback: emDOCs.net – Emergency Medicine EducationMore Than a Sore Throat: Evaluation and Management of Retropharyngeal Abscess in the Adult - emDOCs.net - Emergency Medicine Education