Author: Ben Shepherd, MBBS FACEM DRANZCOG (Adv) (@OBCast, Emergency Physician Wollongong & Shoalhaven Hospitals NSW Australia) // Edited by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit); and Manpreet Singh, MD (@MprizzleER)
 emDocs is proud to host posts from Ben Shepherd, creator of OBCast. From Ben: “During my emergency medicine specialist training I spent time training towards and working as a rural GP obstetrician. It remains some of the most enjoyable and rewarding time I have spent in medicine. Coming back to emergency medicine it is obvious that my colleagues are often uncomfortable managing pregnancy-related problems, particularly those in the latter stages. The goal of ‘OBcast’ is to provide clear and practical information for ‘the reluctant obstetrician’ (emergency physician, rural GP) and improve confidence and the quality of care these families receive during what is both a stressful and wonderful time of their lives.”
emDocs is proud to host posts from Ben Shepherd, creator of OBCast. From Ben: “During my emergency medicine specialist training I spent time training towards and working as a rural GP obstetrician. It remains some of the most enjoyable and rewarding time I have spent in medicine. Coming back to emergency medicine it is obvious that my colleagues are often uncomfortable managing pregnancy-related problems, particularly those in the latter stages. The goal of ‘OBcast’ is to provide clear and practical information for ‘the reluctant obstetrician’ (emergency physician, rural GP) and improve confidence and the quality of care these families receive during what is both a stressful and wonderful time of their lives.”
This post evaluates antepartum hemorrhage. Each post will contain a video presentation and downloadable slides for learning on the go.
Presentation PDF: HERE
Antepartum hemorrhage (APH) refers to vaginal bleeding after 20 completed weeks of pregnancy. It is an important condition to understand, as it has a different set of causes compared to the more familiar bleeding in early pregnancy. Additionally, management is going to involve delivery decisions and potentially the risk of a preterm delivery. It is important to have multidisciplinary collaboration early in the care of these women.
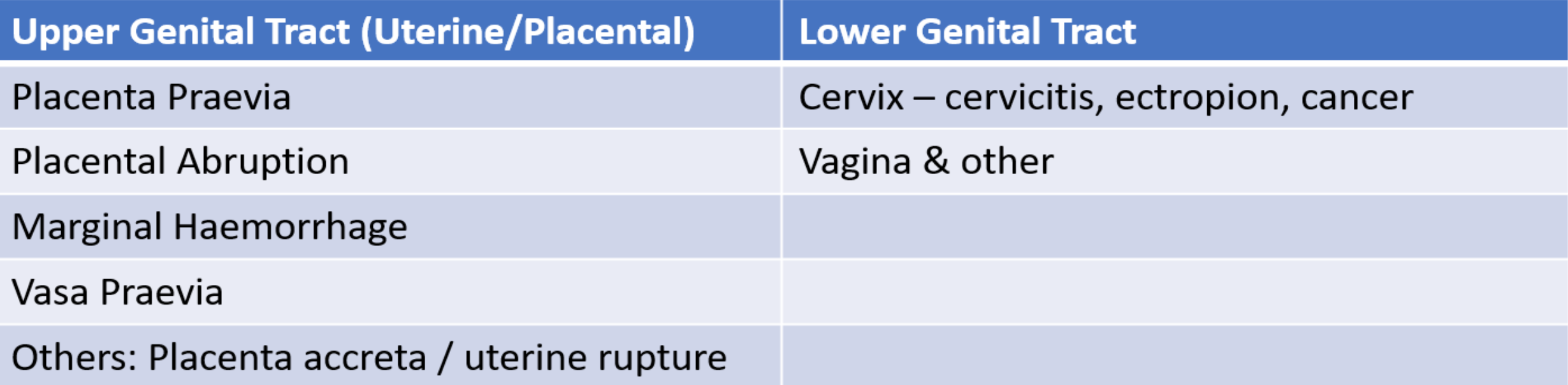
The most common causes are placental abruption and placenta praevia which are covered in more detail, however, for completeness the post will cover a more expanded differential diagnosis.
- 2-5% of pregnancies
- Classification:
- PV Spotting
- Minor APH < 50mL and settled
- Major APH 50-1000mL with no shock
- Massive APH >1000mL and/or signs of shock
- Causes of APH
- Assessment
- History
- Nature and quantity of bleeding
- Presence of contractions/pain/ruptured membranes
- Markers of fetal wellbeing – e.g. movements
- Obstetric history
- General medical history
- Examination
- Vitals / general exam
- Abdominal exam for:
- Tenderness/peritonism
- Contractions
- Fetal lie, presentation, engagement
- Avoid bimanual/speculum exam until placenta praevia excluded
- Investigations
- Mom: CBC, Type and Screen/Cross, Rh status, Kleihauer, coagulation profile
- Baby: Ultrasound
- Management principles
- Resuscitate / Call for help
- Assess fetal and maternal condition – deliver if either compromised
- Seek and treat cause
- History
Placenta Previa
- Definition = placental location below presenting part of fetus
- Usually means adjacent to, or covering internal cervical os
- Grade 1 – 4: Depending on degree of coverage
- If placental edge is more than 2 cm from os, considered “clear” and able to deliver vaginally
- Hallmark feature = painless bleeding
- Small bleed can ‘herald’ a bigger bleed
- Management principles
- Admit all, if time and gestation <35/40 weeks, give/consider corticosteroids/MgSO4
- Resuscitate if required
- Assess maternal and fetal condition (C/S if either is compromised)
- Elective C/S at 37/40 weeks if stable
Placental Abruption
- Separation of placenta with associated bleeding from exposed vessels
- Also reduced functional surface area of placenta
- Can be spontaneous or following trauma (direct abdominal trauma or even deceleration/seat-belt injury)
- Typically associated with abdominal pain and uterine tenderness/irritability
- Concealed vs. revealed abruption
- Management
- Resuscitate if required (coagulopathy can occur early)
- Assess maternal and fetal condition, usually deliver
- Often labour well and can deliver vaginally
- C/S if maternal/fetal compromise
More #FOAMed:
- emDocs – Bleeding in the Third Trimester
- EMin5
- WikEM – Placenta Previa
- WikEM – Placental Abruption








1 thought on “OBCast: Antepartum Hemorrhage”
Pingback: June FOAMed - FRCEM Success