
Authors: Kriti Gupta, MD (Pediatric Emergency Medicine Fellow, NewYork-Presbyterian Brooklyn Methodist Hospital, Division of Pediatric Emergency Medicine, Department of Emergency Medicine); Nessy Dahan, MD (Pediatric Emergency Medicine Attending Physician, Emergency Ultrasound Faculty, Division of Pediatric Emergency Medicine, Division of Emergency Ultrasound, Department of Emergency Medicine, NewYork-Presbyterian Brooklyn Methodist Hospital) // Reviewed by: Jessica Pelletier, DO (EM Education Fellow, Washington University in St. Louis); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Introduction
Over 15,000 children are diagnosed with cancer annually, and approximately 10% of those children eventually succumb to their illness [1, 2]. The most common pediatric oncologic processes physicians will encounter in the emergency department (ED) setting are leukemias and lymphomas. Solid organ tumors such as Wilms tumors and neuroblastomas, along with intracranial tumors like pilocytic astrocytomas, are other common malignancies in the pediatric population [1]. Once diagnosed, children typically receive their care at major pediatric cancer centers across the country and enter treatment protocols for chemotherapy or clinical trials (if eligible). The overall outlook for children has improved significantly in the last few decades. In 2013, the 5-year survival rate for children with any type of malignancy was approximately 85%, up from 58-68% in the 1970s [1]. Once pediatric cancer patients achieve remission, they are followed in survivorship clinics for continued surveillance well into adulthood.
A prerequisite to this article is the understanding of how malignancy in children can present prior to initial diagnosis, as well as the emotional and physical burden upon patients and their families during this vulnerable time in their lives. The focus of this article, however, is to increase recognition of and management of the most common pediatric oncologic emergencies. Even though it is not common for pediatric patients to have oncologic processes, if you work in a pediatric ED it is almost certain you may encounter a patient with this medical history. Our job as a pediatric emergency medicine (EM) clinician is to ask a few salient questions with your history-taking (see Table 1), maintain a high index of suspicion for associated emergencies, perform a thorough physical exam (Table 1), and treat your patient with compassionate care. Be on the lookout for these particular emergencies that are “can’t-miss” diagnoses. Early recognition and treatment may significantly improve morbidity and mortality.
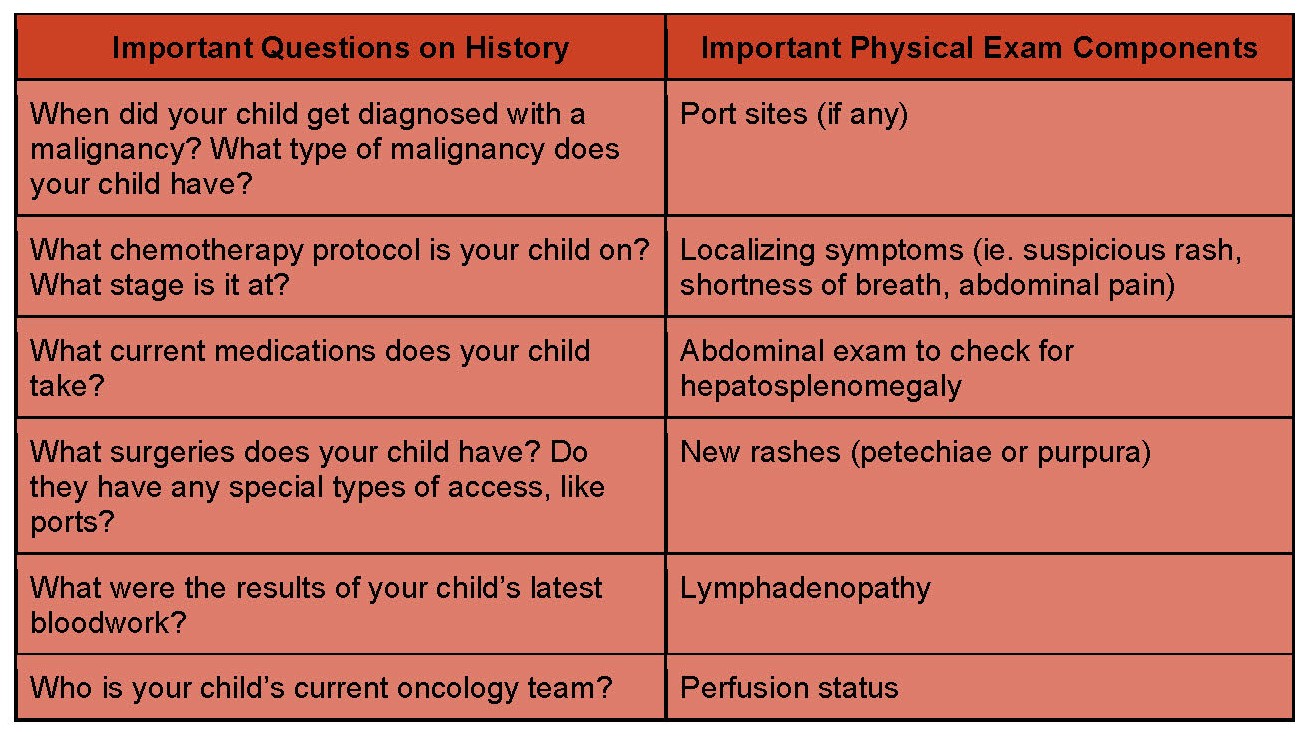
Table 1: Details to consider on history and physical examination of pediatric oncology patients [3]
Case 1: Oncologic Patient with Abdominal Pain
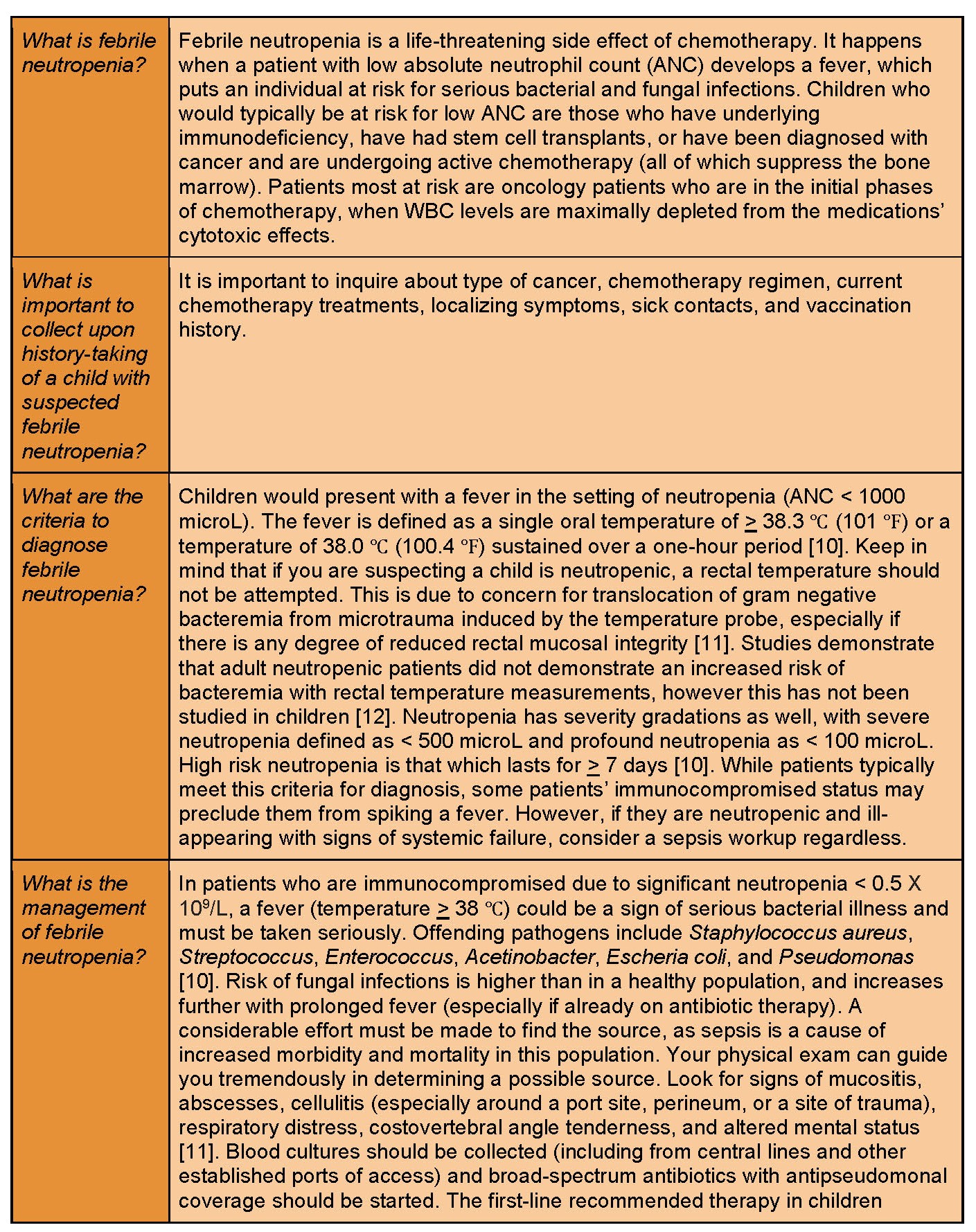
A 4-year-old male recently started chemotherapy for acute B-cell acute lymphoblastic leukemia (ALL). Today, he developed a fever to 101.4 ℉ at home. On further questioning, the child had watery stools the past three days. His parents have been told to come to the ED for any fevers that occur. His only abnormal vital sign in the ED is a temperature of 100.9 ℉. When you examine him, he complains of abdominal pain in his lower quadrants.
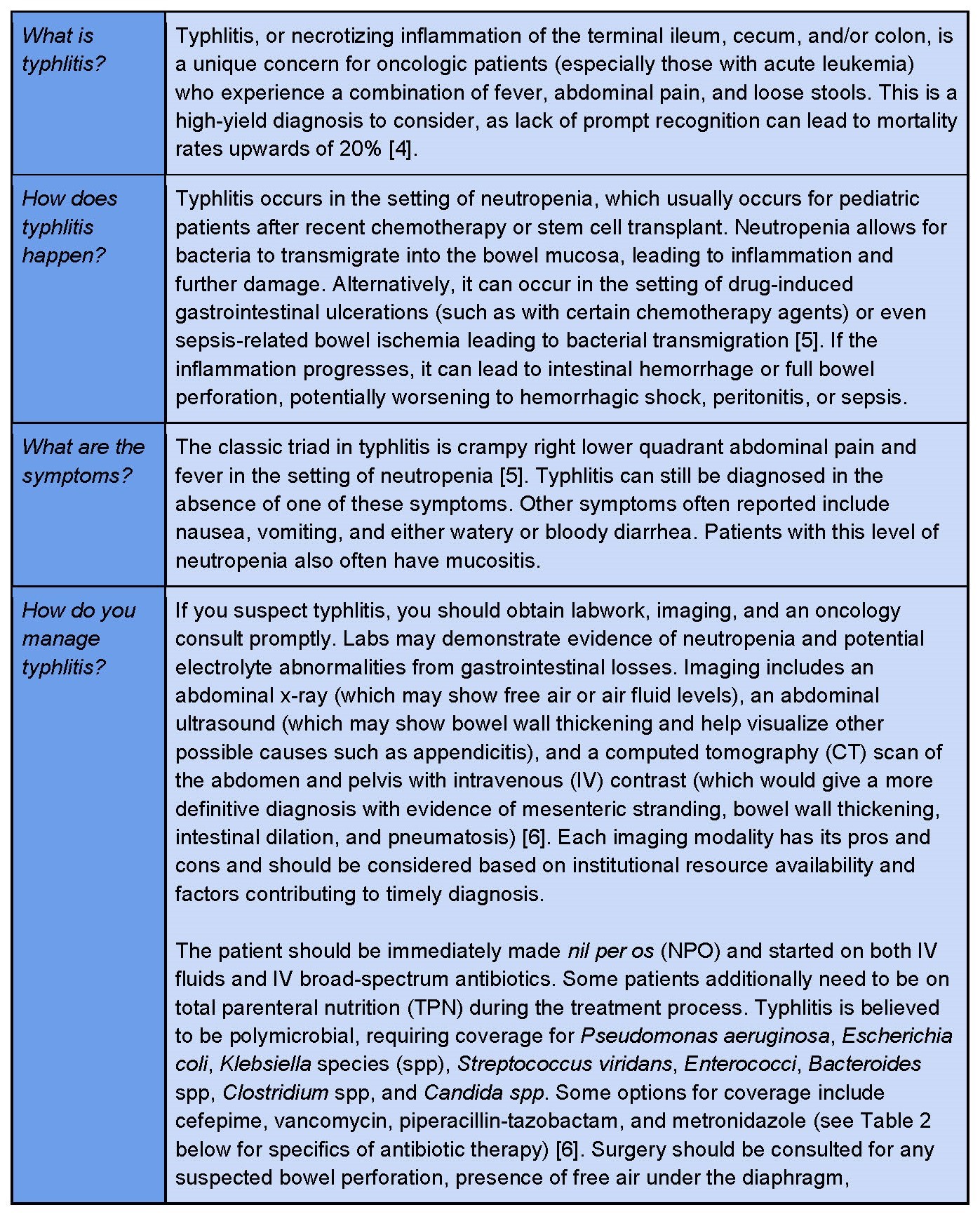
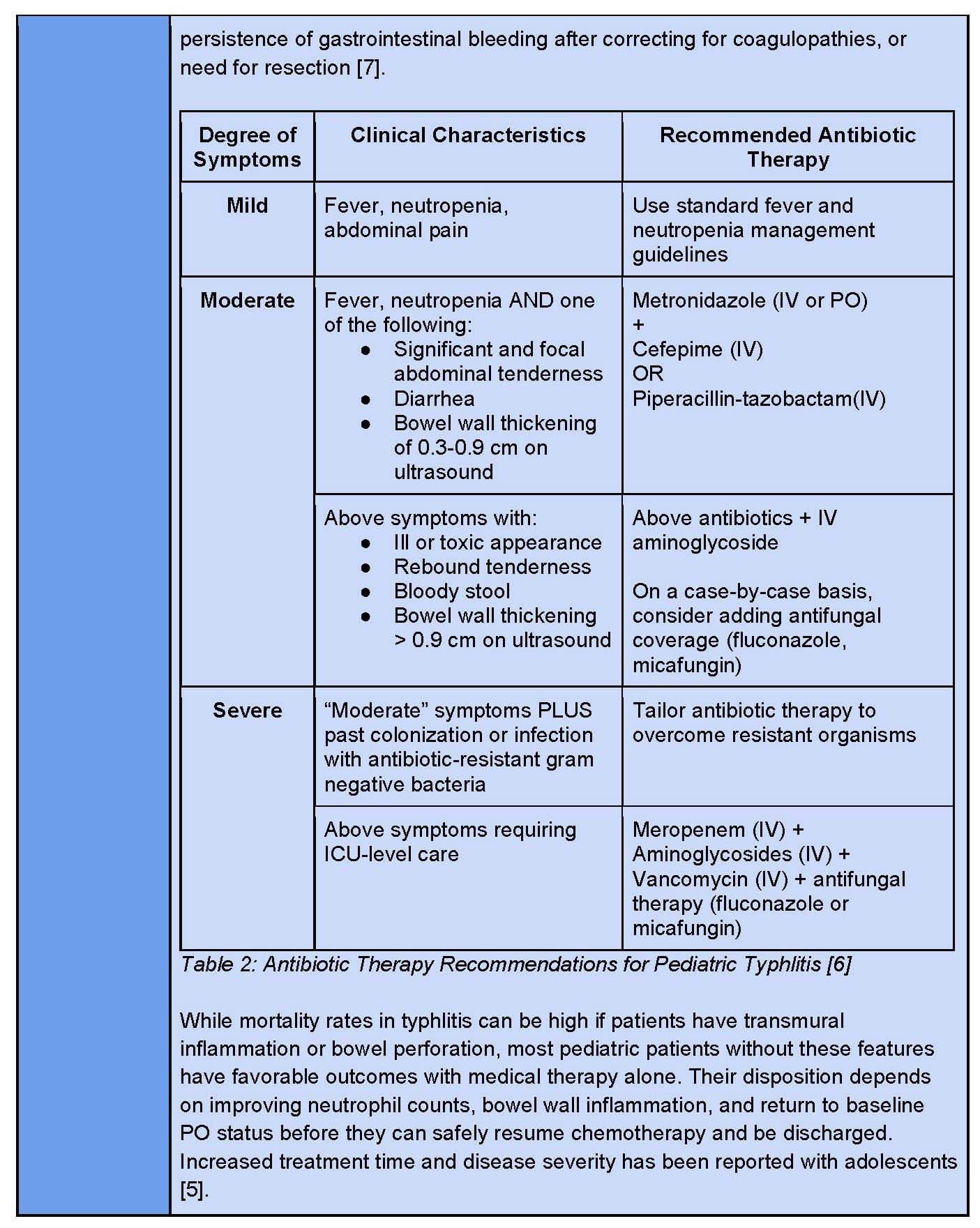
Concern: Typhlitis
Case 2: Complications of New Oncologic Diagnosis
A 10-year-old female presents to the ED with fatigue, weight loss, easy bruising, and a petechial rash for the past month. She is ill-appearing and complaining of a headache. Labs are performed, which demonstrate a white blood cell (WBC) of 105 X 109/L.
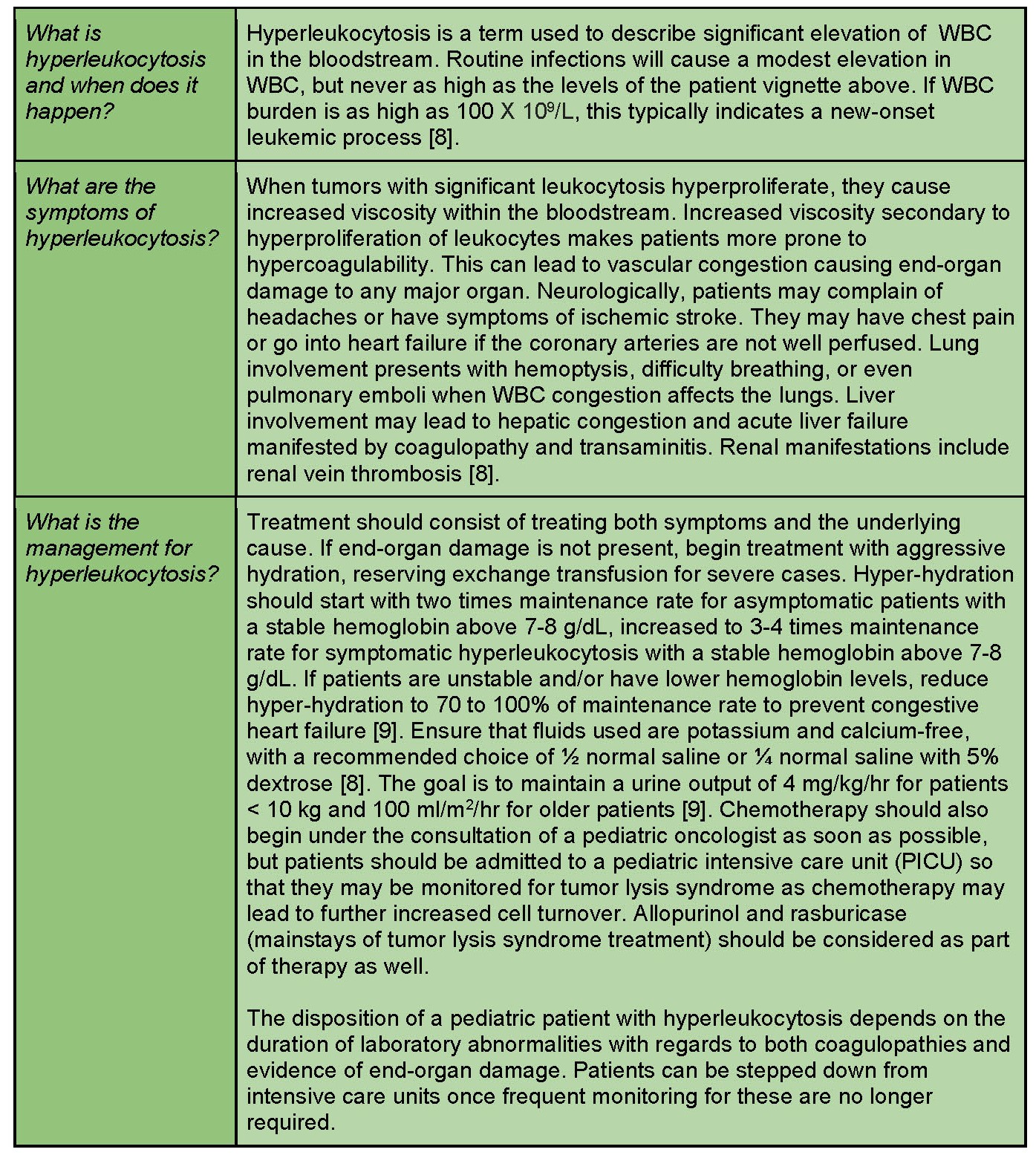
Concern: Hyperleukocytosis
Case 3: Oncologic Patient with a Fever
A 4-year-old male with a new diagnosis of B-cell ALL started the induction phase of his chemotherapy regimen. He spiked a fever of 38.7 ℃ and presents to the emergency room with a cough, congestion, and runny nose. The patient appears pale and fatigued.
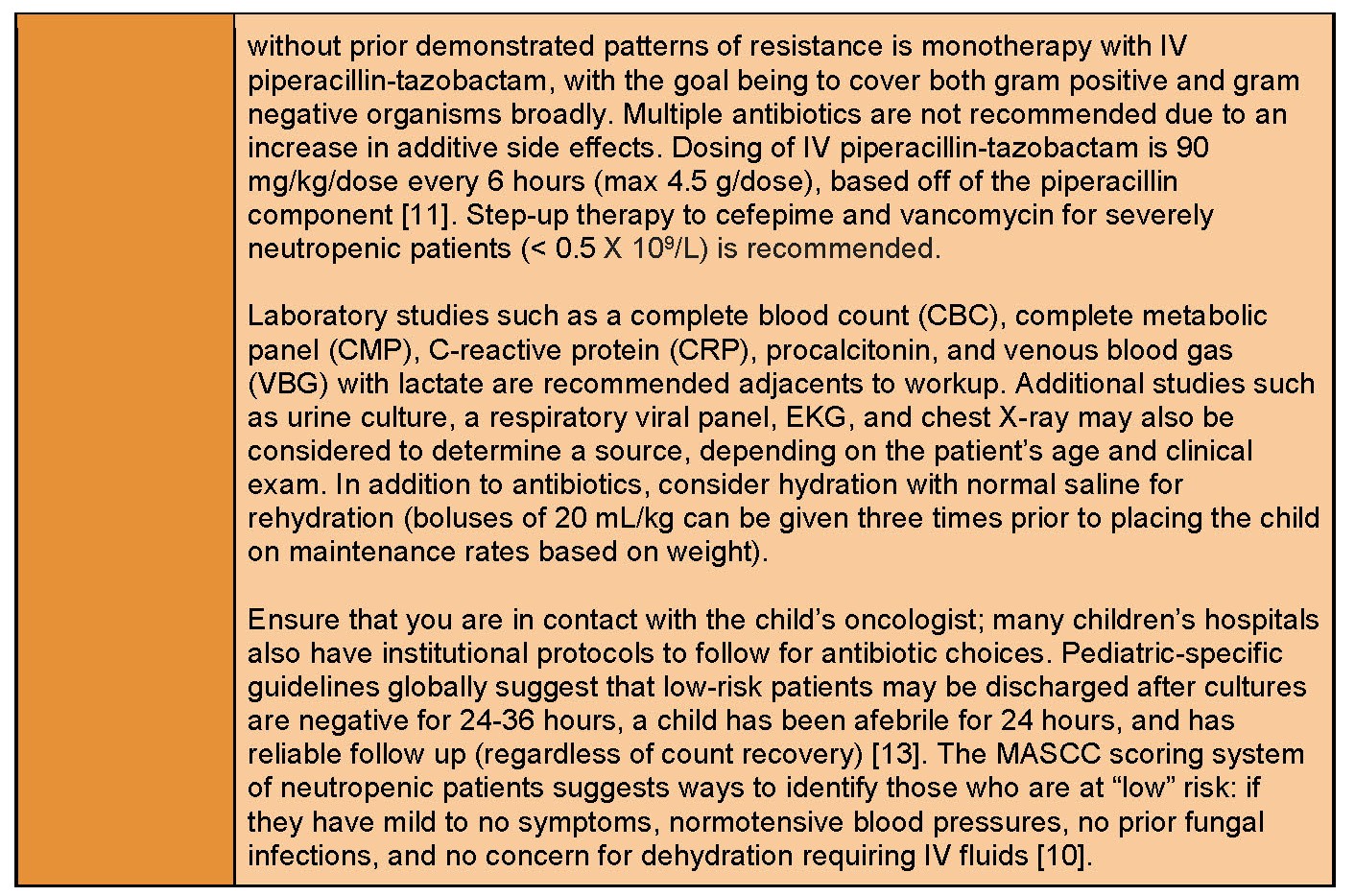
Concern: Febrile Neutropenia
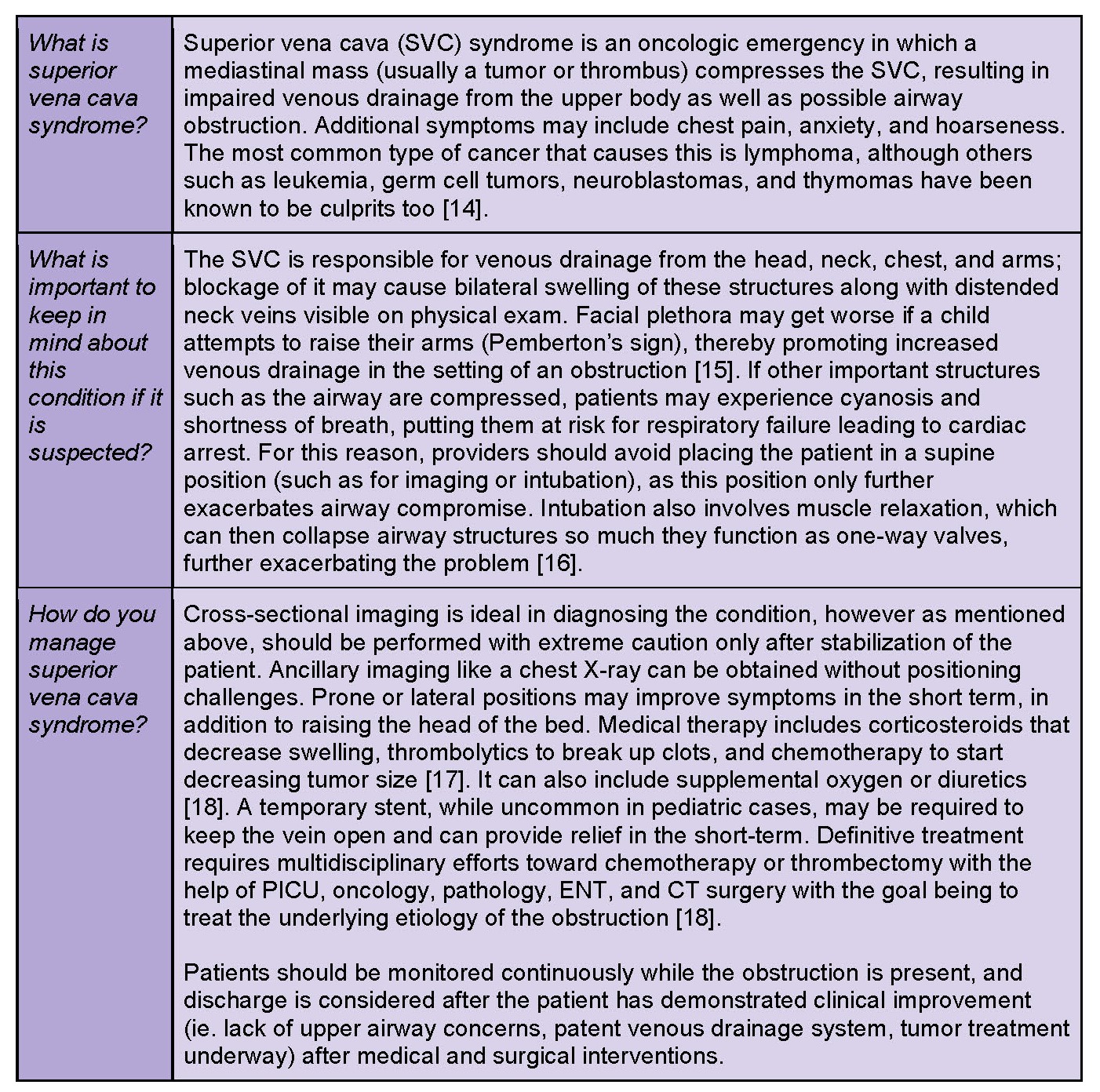
Case 4: Upper Body Swelling in New Oncologic Process
A 10-year-old male presents with fevers, night sweats, and weight loss for a few weeks. His mother noted difficulty breathing and swelling of his face and arms, increasing significantly over the past two days.
Concern: Superior Vena Cava Syndrome
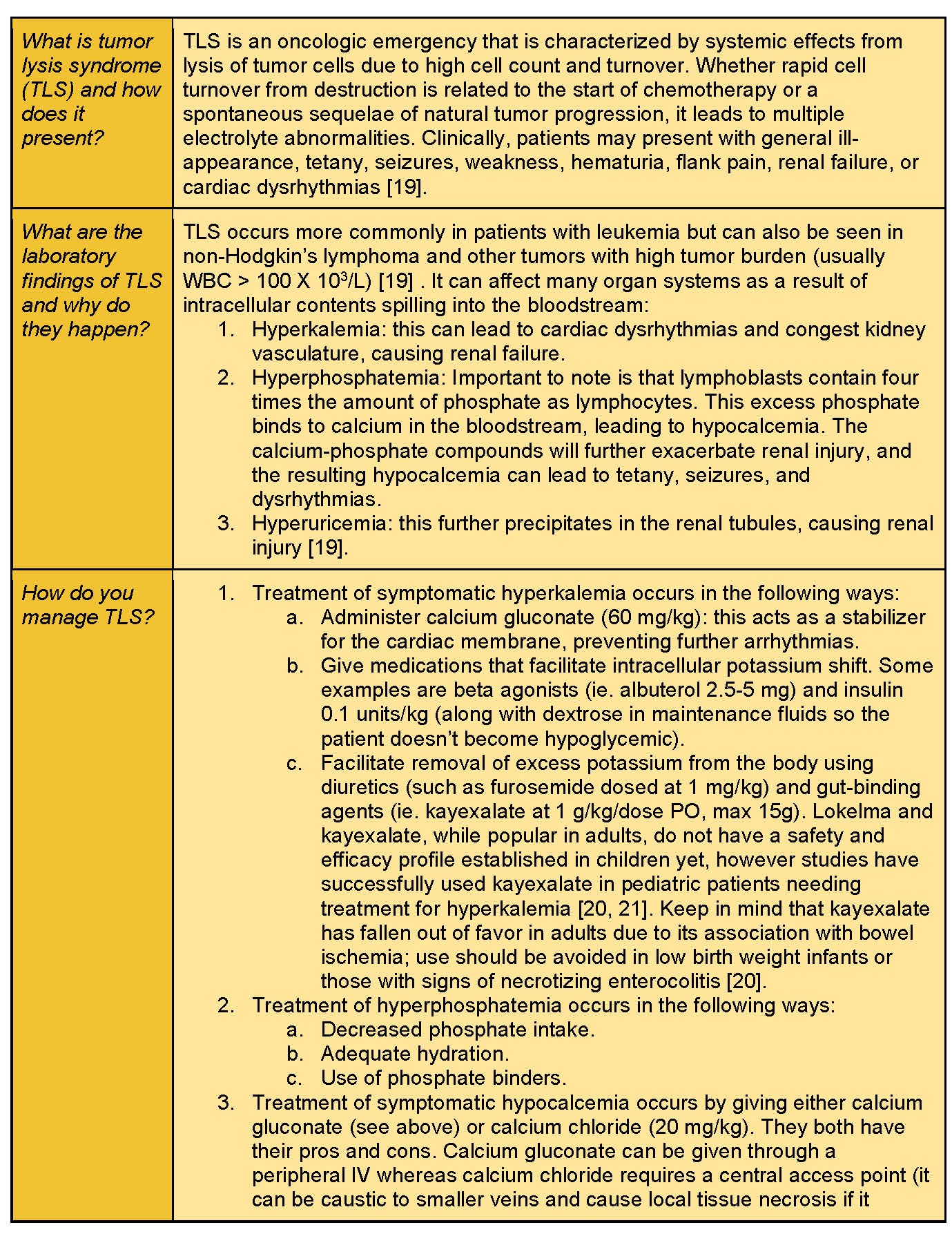
Case 5: Complications of Recent Chemotherapy
A 4-year-old female presents to your ED with a chief complaint of weakness and tetany noticed by the parent. You note multiple electrolyte abnormalities on your iSTAT machine: a high potassium and low calcium. You perform blood work as part of your evaluation and note a high WBC burden with evidence of blasts. The patient then has a seizure.
Concern: Tumor Lysis Syndrome

Take Home Points
- Pediatric oncology patients may have chief complaints (such as fever and abdominal pain) that are considered emergencies, even if they are typically uncomplicated complaints in children who are healthy.
- A careful history and physical exam, understanding of the patient’s chemotherapy regimen, in addition to timely contact with a child’s oncology team, are all paramount to improve outcomes for children with cancer who present to the emergency room.
- Consider a broad differential in oncologic patients while tailoring care to prepare for the “worst-case” scenario.
Related Posts:
- https://www.emdocs.net/oncologic-emergencies-part-i-pearls-and-pitfalls/
- https://www.emdocs.net/oncologic-emergencies-part-ii-pearls-and-pitfalls/
- https://pedemmorsels.com/neutropenic-fever/
- https://pedemmorsels.com/tumor-lysis-syndrome/
- https://pedemmorsels.com/superior-vena-cava-syndrome-in-children/
- https://pedemmorsels.com/typhlitis/
References
- National Cancer Institute. Cancer in Children and Adolescents. National Cancer Institute. Published 2017. https://www.cancer.gov/types/childhood-cancers/child-adolescent-cancers-fact-sheet
- American Childhood Cancer Organization. American Childhood Cancer Organization (ACCO). ACCO. Published April 5, 2019. https://www.acco.org/us-childhood-cancer-statistics/
- Altınel E, Yarali N, Isık P, Bay A, Kara A, Tunc B. Typhlitis in acute childhood leukemia. Med Princ Pract. 2012;21(1):36-39. doi:10.1159/000331587
- McCarville MB, Adelman CS, Li C, et al. Typhlitis in childhood cancer. Cancer. 2005;104(2):380-387. doi:10.1002/cncr.21134
- Cross, Shane J. PharmD, BCPS*,†; Patel, Jay R. MS‡; Wolf, Joshua MBBS, PhD, FRACP. Diagnosis and Management of Typhlitis and Neutropenic Enterocolitis in Children with Cancer. The Pediatric Infectious Disease Journal 41(8):p e326-e328, August 2022. | DOI: 10.1097/INF.0000000000003556
- Shamberger RC, Weinstein HJ, Delorey MJ, Levey RH. The medical and surgical management of typhlitis in children with acute nonlymphocytic (myelogenous) leukemia. Cancer. 1986 Feb 01;57(3):603-9
- Jain R, Bansal D, Marwaha RK. Hyperleukocytosis: emergency management. Indian J Pediatr. 2013;80(2):144-148. doi:10.1007/s12098-012-0917-3
- Ruggiero, A., Rizzo, D., Amato, M. et al. Management of Hyperleukocytosis. Treat. Options in Oncol. 17, 7 (2016). https://doi.org/10.1007/s11864-015-0387-8
- Baluch A, Shewayish S. Neutropenic Fever. Infections in Neutropenic Cancer Patients. 2019;105-117. Published 2019 Aug 11. doi:10.1007/978-3-030-21859-1_8
- Davis K, Wilson S. Febrile neutropenia in paediatric oncology. Paediatr Child Health (Oxford). 2020;30(3):93-97. doi:10.1016/j.paed.2019.12.002
- Olchowski J, Zimhony-Nissim N, Nesher L, Barski L, Rosenberg E, Sagy I. The Risk of Rectal Temperature Measurement in Neutropenia. Rambam Maimonides Med J. 2023;14(3):e0014. Published 2023 Jul 31. doi:10.5041/RMMJ.10501
- Mario Melgar et al. Guidance Statement for the Management of Febrile Neutropenia in Pediatric Patients Receiving Cancer-Directed Therapy in Central America and the Caribbean. JCO Glob Oncol 6, 508-517(2020). DOI:1200/JGO.19.00329
- Gupta, V., Ambati, S.R., Pant, P. et al. Superior vena cava syndrome in children. Indian J Hematol Blood Transfus 24, 28–30 (2008). https://doi.org/10.1007/s12288-008-0020-0
- Basharia, S. (2004, March 24). Pemberton’s sign | NEJM.https://www.nejm.org/doi/full/10.1056/NEJMicm990287
- Miller SM, Cervantes SS. Superior Vena Cava Syndrome in an Infant: A Case of Delayed Diagnosis. Cureus. 2021;13(10):e18583. Published 2021 Oct 7. doi:10.7759/cureus.18583
- Ozcan A, Unal E, Karakukcu M, Coskun A, Ozdemir MA, Patiroglu T. Vena cava superior syndrome in the children with mediastinal tumors: Single-center experience. North Clin Istanb. 2020 Apr 9;7(3):255-259. doi: 10.14744/nci.2019.46354. PMID: 32478297; PMCID: PMC7251265.
- Pediatric Oncology: Superior vena cava syndrome. telemedicina.med.muni.cz. https://telemedicina.med.muni.cz/pediatric-oncology/index.php?pg=emergencies-in-pediatric-oncology–superior-vena-cava-syndrome
- Howard SC, Jones DP, Pui CH. The tumor lysis syndrome [published correction appears in N Engl J Med. 2018 Sep 13;379(11):1094]. N Engl J Med. 2011;364(19):1844-1854. doi:10.1056/NEJMra0904569
- Lee J, Moffett BS. Treatment of pediatric hyperkalemia with sodium polystyrene sulfonate. Pediatr Nephrol. 2016;31(11):2113-2117. doi:10.1007/s00467-016-3414-5
- Chaitman M, Dixit D, Bridgeman MB. Potassium-Binding Agents for the Clinical Management of Hyperkalemia. P T. 2016;41(1):43-50.
- Heining, M. P. D., D. M. Band, and R. A. F. Linton. “Choice of calcium salt: A comparison of the effects of calcium chloride and gluconate on plasma ionized calcium.” Anaesthesia11 (1984): 1079-1082.
- Mirrakhimov AE, Voore P, Khan M, Ali AM. Tumor lysis syndrome: A clinical review. World J Crit Care Med. 2015;4(2):130-138. Published 2015 May 4. doi:10.5492/wjccm.v4.i2.130
- Cheung WL, Hon KL, Fung CM, Leung AK. Tumor lysis syndrome in childhood malignancies. Drugs Context. 2020;9:2019-8-2. Published 2020 Feb 25. doi:10.7573/dic.2019-8-2





