Welcome back to Small Talk. Every first Wednesday of the month we will release high yield PEM content written by PEM talent from around the country. We hope you enjoy these reviews. Comments, questions, accolades or concerns: feel free to reach out to Joe Ravera, MD (pemgemspod@gmail.com).
Authors: Drew Weinstein, MD, MS (EM Resident physician, UC San Diego Health) and Kristy Schwartz, MD, MPH, FACEP (Assistant Health Sciences Clinical Professor, UC San Diego Health/Rady Children’s Hospital San Diego)
Reviewed by: Joe Ravera MD (@pemuvm1, Director of Pediatric Emergency Medicine, Assistant Professor of Surgery, Division of Emergency Medicine, University of Vermont Medical Center); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
The Emergency Department (ED) is a chaotic, loud, and busy environment. Patients in the ED often face long wait times and a substantial amount of stimulation, which can be especially problematic for people with autism spectrum disorder (ASD). Individuals with ASD require health care or hospitalization at a higher rate when compared to their peers.1,2People with ASD may have trouble coping with new and uncertain environments, such as the ED, have difficulty communicating, and suffer from hyperacusis, making it more complex to provide adequate patient-centered care to these individuals. Therefore, it is critical to understand the challenging concerns of a patient with ASD in the chaotic ED environment, and the effects on clinician interaction and care. This review discusses a case study of a patient with ASD who presented to the ED and strategies for clinicians to make their patients with ASD more comfortable, thereby providing the best care.
Case
A 13-year-old male with a past medical history of autism spectrum disorder and juvenile myoclonic epilepsy presented to the emergency department via emergency medical services (EMS) from daycare for evaluation of abdominal pain. The patient’s mother had yet to arrive. Per EMS, the patient had not been acting himself for the prior two days, had been grabbing his abdomen, crying inconsolably, and was witnessed to be hitting himself more frequently. Starting that morning, he had multiple episodes of non-bloody, non-bilious emesis.
His vital signs on arrival included heart rate 137, respiratory rate 29, oxygen 96% on room air, temperature 38.9oC. Blood pressure was unable to be obtained because the patient flailed his arm when attempts were made.
The patient was dressed in clean clothes, strapped down to an EMS gurney, yelling out, and trying to break free from the safety belts. He appeared flushed and had dried nasal mucus along his cheek. He was tachypneic. An attempt to listen to his lungs was unsuccessful due to the patient’s vocalizations and thrashing. His capillary refill was slightly delayed at 3-4 seconds.
Definition/Prevalence
Autism spectrum disorder can be diagnosed at any age, though most often the diagnosis occurs after age 2 years as the characteristic symptoms become more apparent. Symptoms include deficits in social communication and interaction with others, limited interests, and repetitive behaviors that cause significant impairment in functioning.3,4,5 While early diagnosis is recommended given opportunities for intervention, many children do not receive a final diagnosis until later, most commonly by 4 years of age.6 The prevalence of ASD in the United States is about 1 in 44 children and ASD is 4.2 times more prevalent in boys than girls.7 Individuals with autism may present with a wide variety of symptoms of varying severity, as defined by the DSM-5 diagnostic criteria.3
Autism Spectrum Disorder is frequently associated with a variety of comorbidities. Medical comorbidities include but are not limited to: obesity, gastrointestinal conditions, seizure disorders, and sleep disorders. Psychiatric/behavioral comorbidities include: anxiety disorders, attention deficit-hyperactivity disorder, and depression.8,9 These comorbidities may put people with ASD at greater risk for requiring ED care. It is imperative that physicians in the ED be prepared to properly treat a patient with ASD, with consideration to care of commonly associated conditions and ASD symptoms, which the patient may find challenging to communicate.
The Visit
Individuals with ASD typically react better in structured environments with set expectations. In the ED, patients with ASD often face unfamiliarity and unpredictability, which may exacerbate their symptoms and put a strain on the patient-clinician relationship. Individuals with ASD have unique sensory, behavioral, and communication needs that are often difficult to assess or address when in an emergent situation. It is important that clinicians be prepared for such patients so that treating them and addressing their unique needs becomes second nature.1
One thing that remains true throughout treating all patients with ASD, beyond the patient, is that parents/guardians, caregivers, and family are the experts. Never delay consulting them. Include them in the care early and often.1
Preparation is critical to caring for patients with ASD in the ED. It begins with team members who are trained in appropriate, effective communication and providing a safe, comfortable environment for patients with ASD and their caregivers. The Center for Disease Control (CDC) and the American Academy of Pediatrics (AAP) provide training resources on ASD and offer evidence-based practices.10 Preparation and ongoing professional development can build the team’s confidence and effectiveness when treating patients with ASD in the ED, therefore improving overall patient care.
When a patient with ASD arrives at the ED, strive to identify them early. If possible, offer a separate waiting area with less stimulation, or allow the patient to wait outside or in their car if a separate space is not available.9 Additionally, placing these patients in rooms earlier and providing them with developmentally appropriate toys may also be beneficial.1
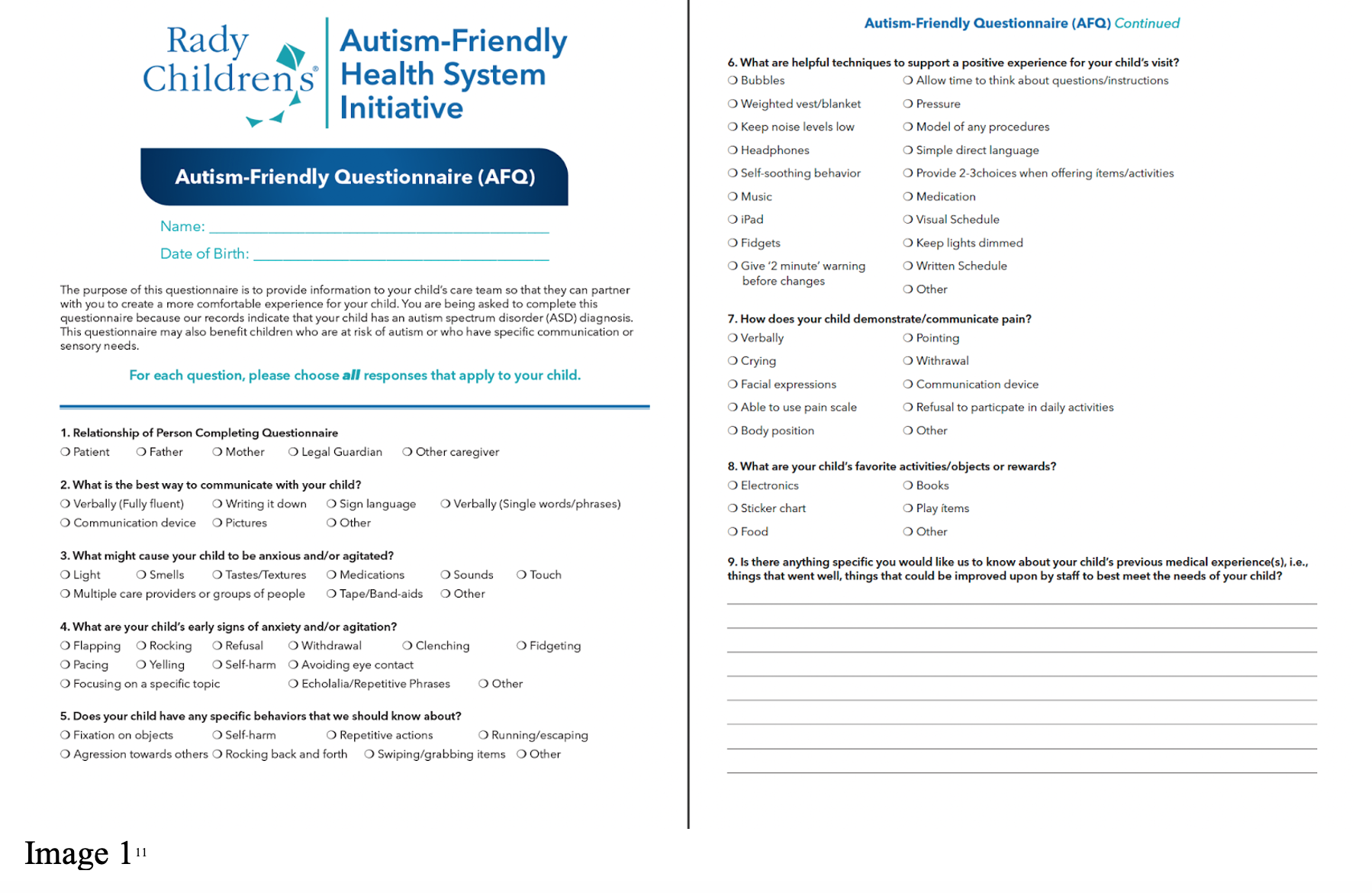
An instrument to identify patient-specific information may help, such as a short questionnaire to assist the team with knowing and understanding the patient. Offer this questionnaire at triage to collect details on stressors, triggers, and communication styles. Here is an example of an ASD questionnaire used at Rady Children’s Hospital San Diego.11
Child Life Specialists are excellent allies in treating patients with ASD. They provide the team with helpful tools and offer calming techniques to create an environment suitable for the patient.
Placing patients with ASD in a private room modified to best suit the patient’s needs should be a priority.1 Often, caregivers will come prepared with adequate interventions such as headphones or electronic devices for the patient. On the occasion that caregivers did not bring these items or the patient arrived alone, utilizing the ED’s devices (or, if willing, the team’s personal devices) to play videos or providing noise-canceling headphones may be helpful.
Clinicians may have difficulty taking a medical history and performing a physical exam on patients with ASD. It is important to build rapport and talk with the patient at their level of understanding. Clinicians should not force themselves into the patient’s personal space. When describing what will happen or eliciting information from the patient, utilize visual charts or drawings, as people with ASD often respond better to visual rather than verbal information. It may be helpful to use a “First-Then” board to illustrate the plan and identify a reward once completed. The Autism Speaks Treatment Network has an example of a “First-Then” board.12 Additionally, roughly 30% of people with ASD are nonverbal, so give caregivers an opportunity to provide the medical history and help the team interpret the patient’s nonverbal cues.8,9
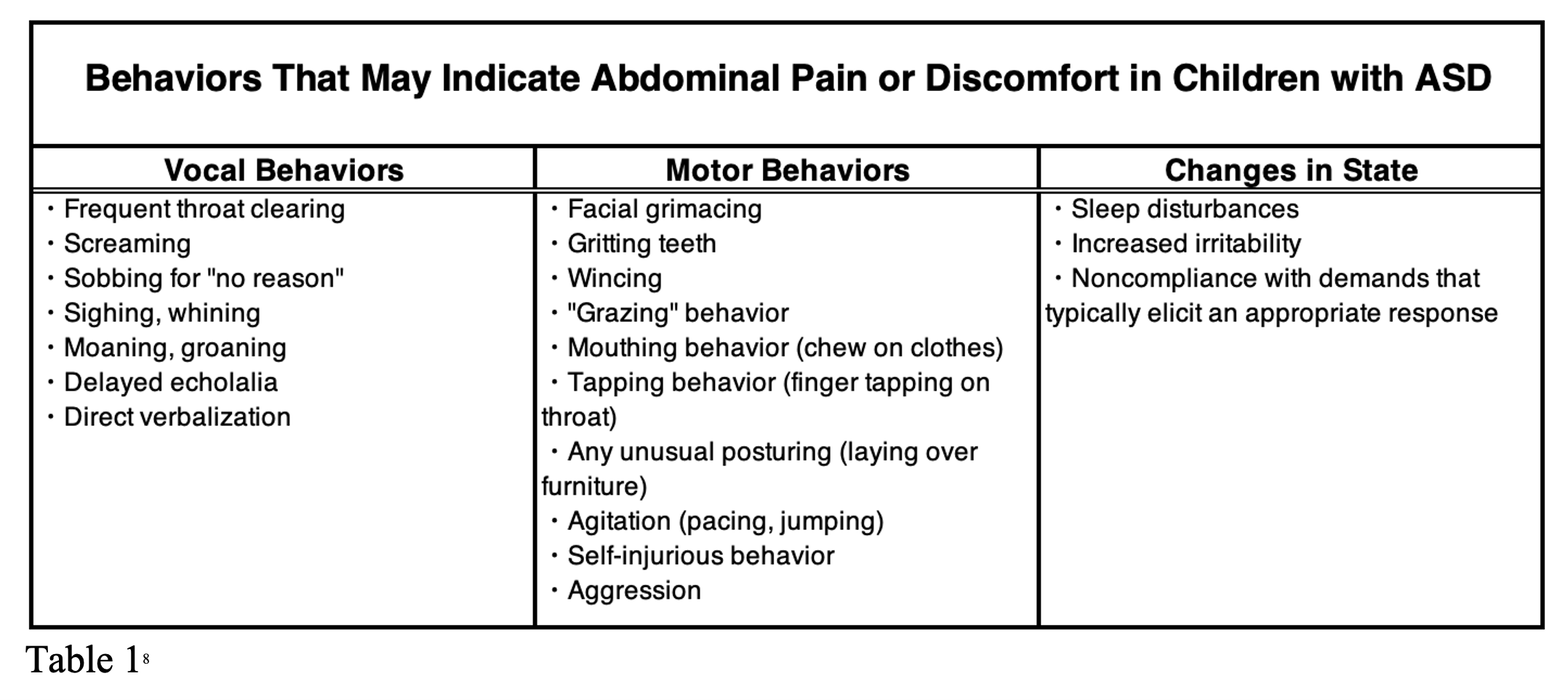
This table adapted from the AAP may be useful in interpreting behaviors suggestive of abdominal pain or discomfort in patients with ASD (Table 1).8
Individuals with ASD benefit from consistency and predictability. Therefore, try to maintain a consistent care team with as few staff members as possible who interact with the patient. New faces may cause undue stress on the patient and impede quality patient care. Limit the number of people in the room, ensuring that each team member introduces themselves and clearly explains their role. Team members and, if helpful, caregivers should talk outside the room and only the necessary individuals should enter the room to interact with the patient. The goal remains the same: cultivate a safe, calm environment for the patient.1
Communicating with patients with ASD may be different than with other patients. Do not be surprised if the patient with ASD avoids eye contact.3,4,5 They are listening to everything you say and will take things quite literally. Use a calm and gentle voice, give simple commands, and avoid idioms or sarcasm. People with ASD may have a slower processing speed, so pause to give them time to respond to questions or requests.13 Since patients with ASD benefit from predictability and touching can be stressful, explain or demonstrate what will happen before touching them. Reassure them that nothing will happen without you telling them what to expect first, then be consistent with this practice.1,13
If a procedure is indicated for a patient with ASD, a considerable amount of time should be taken to prepare for it. Procedures can be the most stressful part of the experience for these patients; therefore, take time to discuss the procedure in advance with the patient and their caregiver. When discussing the procedure with the patient, use visual aids to help them understand.1 For example, allow the patient to see and touch a tourniquet or catheter (with the needle removed, of course) before placing an intravenous (IV) line.13 Clinicians and team members should review the patient’s coping mechanisms and ensure that their environment is still suitable for them. Patience is key. The team should plan for a longer procedure time than the average patient, ensuring that steps are carefully explained and performed without rushing.1
Pearls and Pitfalls
- People with ASD are four times more likely to be seen in the ED when compared to their peers.2
- People with ASD present atypically and have barriers to communication which can obfuscate the diagnosis. Caregivers are a vital resource. They are knowledgeable of the patient’s nonverbal cues, can help obtain a history and exam, and can help the team provide a smooth visit for the patient.
- Preparation is key: have tools such as a triage survey to identify triggers and coping mechanisms, noise-canceling headphones, developmentally appropriate toys, visual aids, and separate waiting areas and staff training on how to interact with patients with ASD is extremely important
- Making the patient feel comfortable is critical. Modify the environment to make it more suitable for the patientby providing a private room, lowering the lights, and decreasing the number of staff interactions.
- Communication is important: be calm and patient, use literal phrases, and explain everything. Look for nonverbal cues, give the patient time to process, and be patient if procedures take more time.
Case conclusion
The 13-year-old boy was well-known in the hospital system. When he arrived, a private room was identified for him, as his caregiver had not yet arrived. The team used a preference questionnaire previously recorded in the electronic healthcare record to identify patient preferences and subsequently created a comfortable environment for him. His nurse provided the patient with a stress ball and used her phone to play animal videos, which the patient identified as one of his preferences. The patient’s mother, who was en route, was contacted and placed on speakerphone to help soothe the patient and to provide further information for the staff. When a new team member entered the patient’s room, they introduced themselves and explained in detail what they were going to do. Antipyretics were administered to the patient in his preferred manner and visual aids were utilized by the clinician to perform an adequate physical examination. Upon examination, the patient was found to have McBurney’s point tenderness. With the help of a Child Life Specialist, an IV was placed, labs were collected, and antiemetics were given. The patient underwent an ultrasound, which showed findings suggestive of appendicitis. Surgery was immediately notified and the patient underwent emergent appendectomy later that evening. The patient spent two days in the hospital recovering and was discharged in stable condition.
References
- Straus J, Coburn S, Maskell S, Pappagianopoulos J, Cantrell K. Medical Encounters for Youth With Autism Spectrum Disorder: A Comprehensive Review of Environmental Considerations and Interventions. Clin Med Insights Pediatr. 2019;13:1179556519842816. Published 2019 Apr 29. doi:10.1177/1179556519842816.
- Liu G, Pearl AM, Kong L, Leslie DL, Murray MJ. A Profile on Emergency Department Utilization in Adolescents and Young Adults with Autism Spectrum Disorders [published correction appears in J Autism Dev Disord. 2017 Mar 23;:]. J Autism Dev Disord. 2017;47(2):347-358. doi:10.1007/s10803-016-2953-8.
- Diagnostic criteria. Centers for Disease Control and Prevention. https://www.cdc.gov/ncbddd/autism/hcp-dsm.html. Published June 29, 2020. Accessed April 18, 2022.
- National Institute of Mental Health. Autism spectrum disorder. National Institute of Mental Health. https://www.nimh.nih.gov/health/topics/autism-spectrum-disorders-asd. Accessed April 18, 2022.
- Hyman SL, Levy SE, Myers SM, et al. Identification, evaluation, and management of children with autism spectrum disorder. Pediatrics. 2020;145(1). doi:10.1542/peds.2019-3447.
- Spotlight on: Delay between first concern to accessing services. Centers for Disease Control and Prevention. https://www.cdc.gov/ncbddd/autism/addm-community-report/delay-to-accessing-services.html#:~:text=Of%20the%20children%20who%20received,limiting%20the%20services%20they%20receive. Published August 27, 2019. Accessed April 18, 2022.
- National Institute of Mental Health. Autism spectrum disorder (ASD). National Institute of Mental Health. https://www.nimh.nih.gov/health/statistics/autism-spectrum-disorder-asd. Published January 2020. Accessed April 18, 2022.
- American Academy of Pediatrics. AAP – Welcome to Identifying and Caring for Children with Autism Spectrum Disorder: A Course for Pediatric Clinicians. Identifying and Caring for Children with Autism Spectrum Disorder. http://asd.pedialink.courses.aap.org/script/unit-4-management-of-co-occurring-conditions/unit-4-recording?req=202205051414312495. Accessed April 18, 2022.
- Al Sharif S, Ratnapalan S. Managing Children With Autism Spectrum Disorders in Emergency Departments. Pediatr Emerg Care. 2016;32(2):101-103. doi:10.1097/PEC.0000000000000705.
- Autism case training landing page. Centers for Disease Control and Prevention. https://www.cdc.gov/ncbddd/actearly/act.html. Published October 6, 2020. Accessed April 18, 2022.
- Rady Children’s Hospital San Diego. Autism-Friendly Healthy System Initiative. 2022.
- Visual Supports and Autism. Autism Speaks. https://www.autismspeaks.org/sites/default/files/2018-08/School%2520Community%2520Tool%2520Kit.pdf. Published March 2011. Accessed May 3, 2022.
- Watson LR, Fraser M, Ballas P. Interacting with a child who has autism spectrum disorder. University of Rochester Medical Center-Health Encyclopedia. https://www.urmc.rochester.edu/encyclopedia/content.aspx?contenttypeid=160&contentid=46. Accessed May 3, 2022.




