
Authors: Dhayashri Dhavapalani, MD (EM Resident Physician, Rutgers New Jersey Medical School); Marwa Ali, MD (Clinical Ultrasound Fellow, Rutgers New Jersey Medical School); Caroline Shepherd, DO (Assistant Professor of EM, Rutgers New Jersey Medical School); Reviewed by Stephen Alerhand, MD (Associate Professor of EM, Rutgers New Jersey Medical School) // Reviewed by: Jessica Pelletier, DO, MHPE (APD/Assistant Professor of EM/Attending Physician, University of Missouri-Columbia); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Case
A 67-year-old male with a past medical history of poorly-controlled diabetes complicated by peripheral neuropathy presents to the emergency department (ED) with worsening swelling, redness, and moderate discomfort in his right calf, ankle, and foot. The patient was evaluated in the ED two days prior for right foot pain, redness, and swelling. X-rays and duplex ultrasound studies at that time were negative, and labs were reassuring, so he was discharged with cephalexin to treat presumptive cellulitis. In the following 48 hours, the patient’s symptoms worsened, and he returned to the ED. He is afebrile and tachycardic to the 110s bpm with a blood pressure of 110/80 mmHg. Physical examination shows a 5 x 8 cm erythematous lesion with ill-defined borders on the right medial calf with slight induration, pitting edema, and a dusky-appearing ankle and dorsal foot. There is no palpable crepitus. He is neurovascularly intact.
Labs during this visit are remarkable for a leukocytosis of 24,000/µL, which is increased from prior, and a lactate of 4.2 mg/d. The rest of the patient’s labs are at baseline. A repeat x-ray of the right lower leg does not show free air within the soft tissues.
POCUS evaluation for necrotizing soft tissue infection
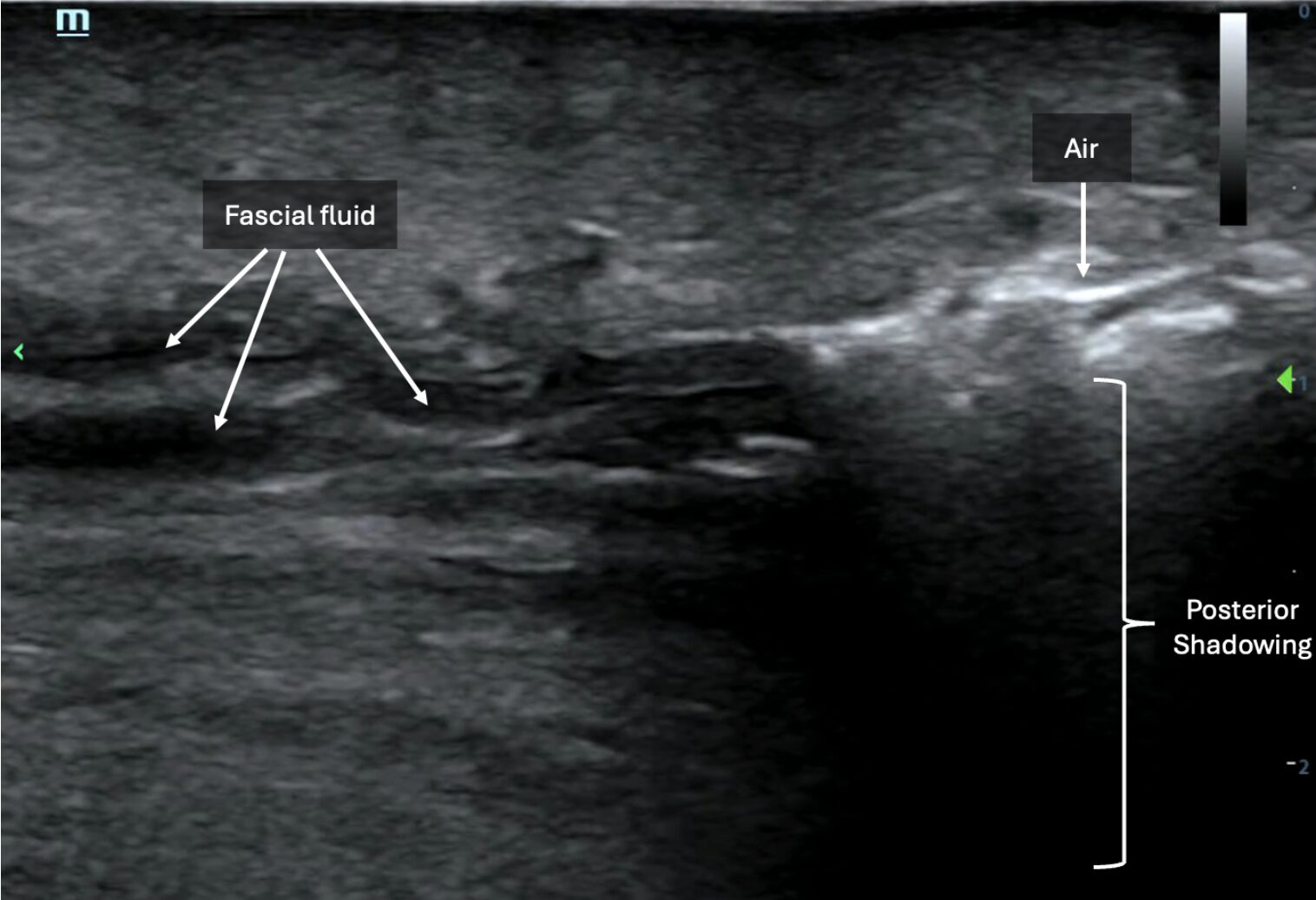
Ultrasonographic findings of necrotizing soft tissue infections include Subcutaneous Thickening, subcutaneous emphysema (Air), and Fascial Fluid – sometimes recalled by the mnemonic “STAFF.”1 The high-frequency linear probe is preferred, as it allows for optimal image resolution of the superficial soft tissue and muscle.1,2
Subcutaneous thickening refers to the widening of the subcutaneous layers. It often occurs with notable edematous infiltration in the form of anechoic streaking between isoechoic dermal layers on POCUS. Classifying the area of interest as abnormal can be established by comparing the affected region of concern to nearby unaffected tissue or to an unaffected contralateral limb (Image 1). This disruption of normal subcutaneous architecture can also demonstrate the finding of “cobblestoning” typically seen in cellulitis or edema. This finding occurs due to the presence of volume overload, inflammation, or infection.
Subcutaneous emphysema on POCUS is demonstrated by hyperechoic foci with posterior “dirty shadowing” in the subcutaneous tissues. Since air scatters ultrasound beams, it results in a heterogeneous, speckled shadowing deep to the gas (Image 1, Image 2, Video 1).3 While subcutaneous emphysema is a key finding of necrotizing soft tissue infection (NSTI), it is also important to remember that it may be present in situations where there was dermal puncture that would introduce air into the soft tissue, such as in the case of animal bites or in the case of actively draining abscesses. In such clinical examples, subcutaneous air alone may not suffice to seal the diagnosis of NSTI.
Image 1:
LEFT: POCUS of unaffected lower leg using the linear transducer. Normal skin, subcutaneous layers, and muscle architecture are maintained.
RIGHT: POCUS of affected lower leg using the linear transducer. Thickened subcutaneous tissue, disruption of subcutaneous architecture, anechoic streaking, and some notable cobble-stoning in deeper fields are noted. Note also the presence of air with posterior dirty shadowing obscuring underlying muscle and bone. Images courtesy of Dr. Shepherd and Dr. Alerhand.
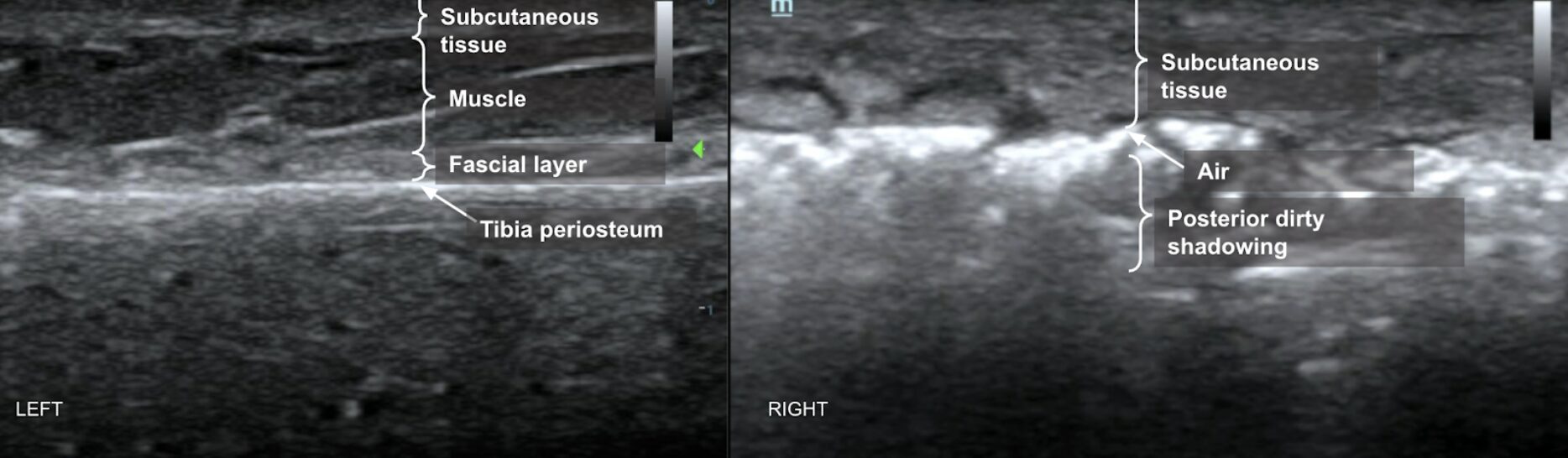
Image 2: POCUS of the tibia in long-axis showing hyperechoic foci (arrows) with shadowing (brackets). Images courtesy of Dr. Shepherd and Dr. Alerhand.
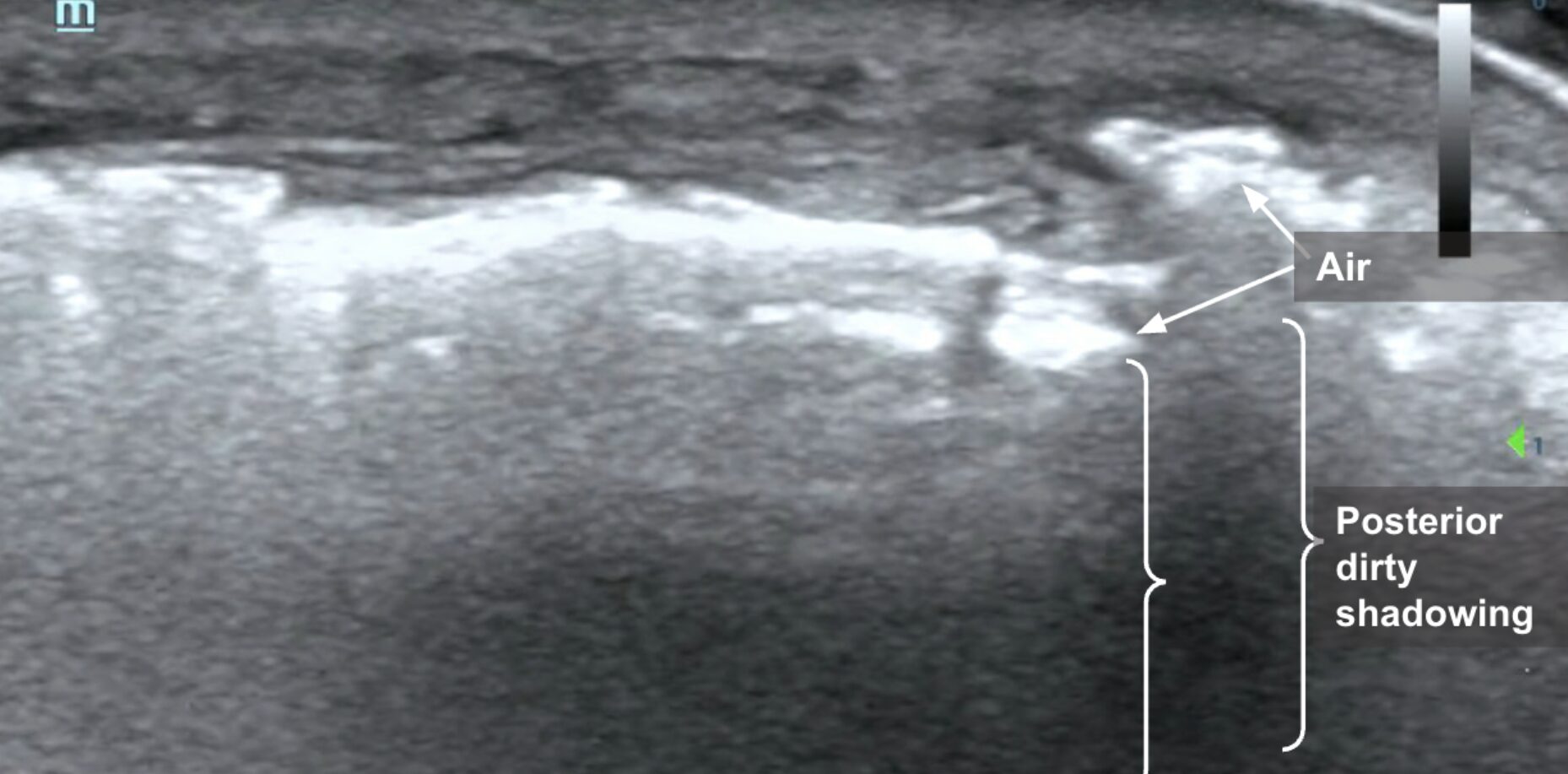
Video 1: Linear transducer view of the tibia in long-axis demonstrating hyperechoic foci with shadowing scattered throughout subcutaneous layers.
Presence of fascial fluid appears as hypoechoic to anechoic layering deep to subcutaneous tissues along the fascial plane superior to and in between muscle layers (Image 3, Video 2).
Image 3: Fascial fluid in the form of anechoic linear streaking (white arrows) visualized deep to the subcutaneous tissue invading deep to the muscle and overlying the tibia in cross-section. Images courtesy of Dr. Shepherd and Dr. Alerhand
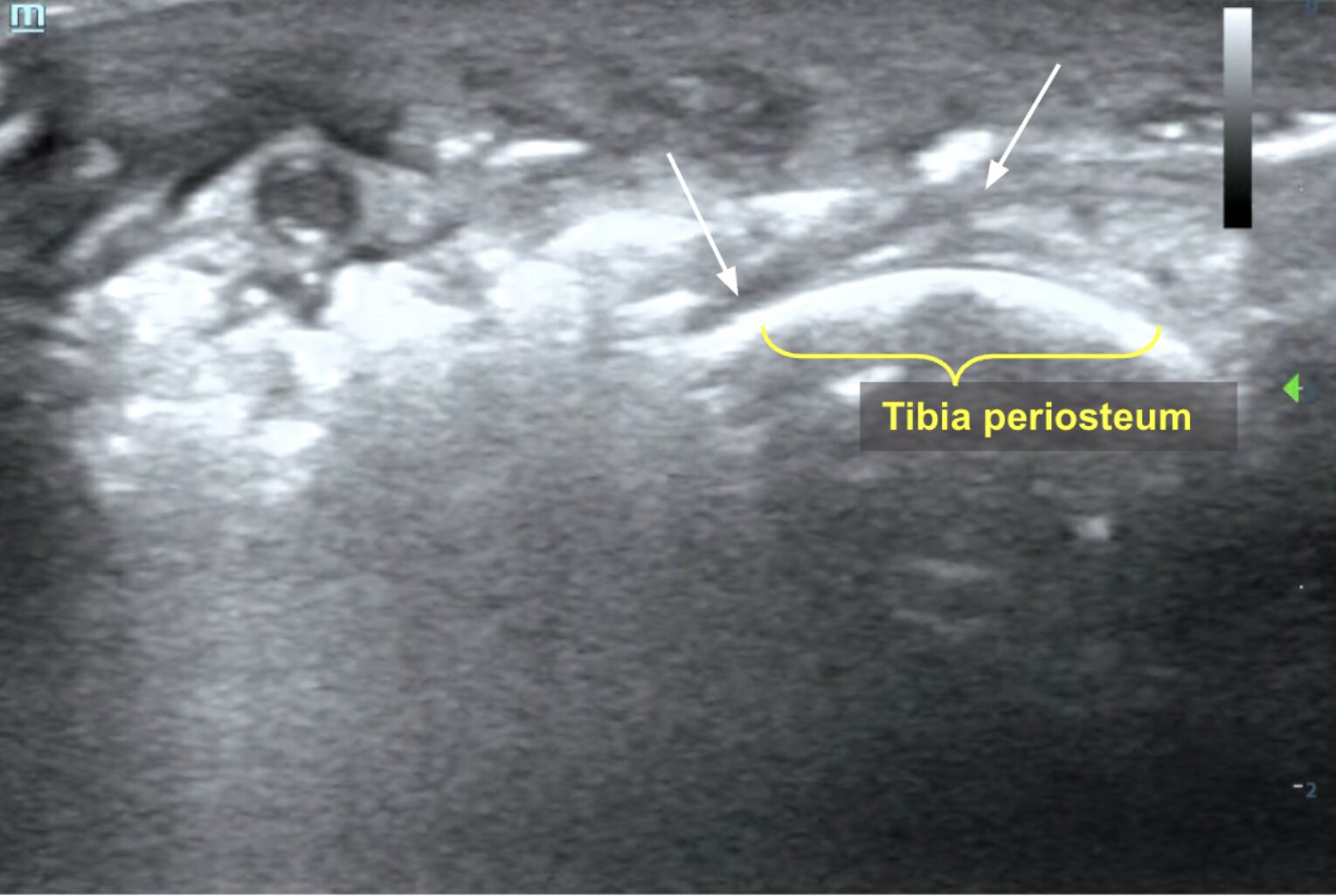
Video 2: Linear transducer view of the tibia in short-axis showing anechoic layering along fascial planes just superior to bone (hyperechoic line in far field). Images courtesy of Dr. Shepherd and Dr. Alerhand
Here we present additional examples of POCUS scans demonstrating sonographic findings of NSTI:
In the case below, note the subcutaneous emphysema appearing as a single linear hyperechoic line with posterior shadowing. Adjacent to that line appears dynamic sparkling echogenic material suggestive of mobile fluid (possibly purulence), interspersed with gas bubbles (within yellow brackets) (Image 4, Video 3).
Image 4: Still image demonstrating subcutaneous air and posterior shadowing (hyperechoic line to the right of the image) and purulence (left side of image). Images courtesy of Dr. Shepherd and Dr. Alerhand.
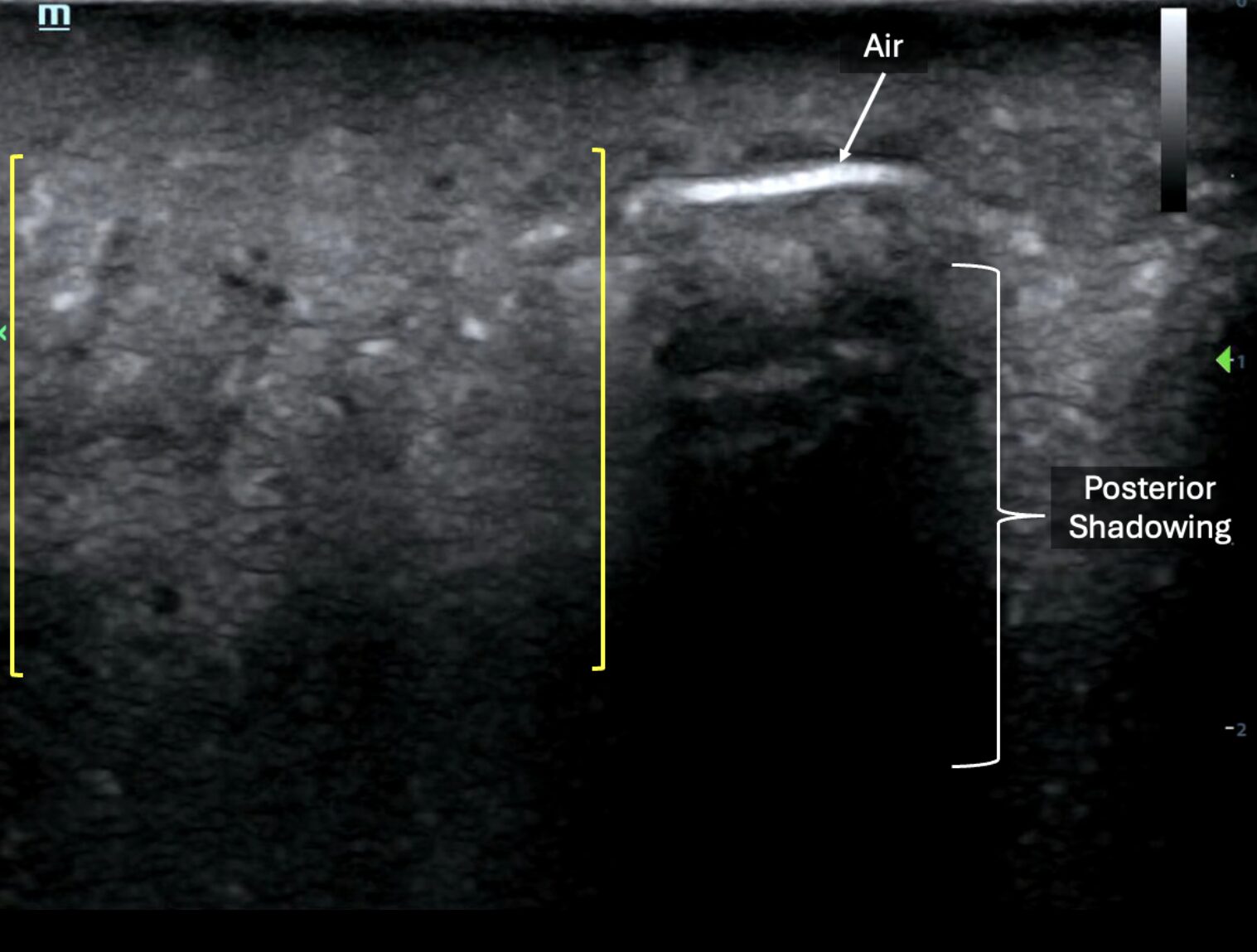
Video 3: Video clip of the above still image demonstrating posterior shadowing and purulence. Images courtesy of Dr. Shepherd and Dr. Alerhand.
Below is another example of anechoic layering of fascial fluid (left side of image) tracking deep to subcutaneous tissues juxtaposed next to hyperechoic foci of air with posterior shadowing, indicating subcutaneous emphysema (right side of image) (Image 5, Video 4).
Image 5: Image demonstrating presence of subcutaneous emphysema (right side of image) and layering of fascial fluid (left side of image). Images courtesy of Dr. Shepherd and Dr. Alerhand
Video 4 : Video clip of the above still image demonstrating subcutaneous emphysema and layering of fascial fluid. Images courtesy of Dr. Shepherd and Dr. Alerhand
POCUS Differential Diagnosis
As necrotizing soft tissue infections are part of a continuum of skin and soft tissue infections that includes cellulitis and abscesses, it is important to recognize and distinguish these diagnoses using POCUS. Cellulitis demonstrates a cobblestone appearance on POCUS but lacks other findings characteristic of NSTI, such as subcutaneous emphysema and fascial fluid (Image 6, Video 5).
Image 6: Disorganized, globular changes localized to the subcutaneous tissue known as “cobblestoning.” Images courtesy of Dr. Shepherd and Dr. Alerhand.
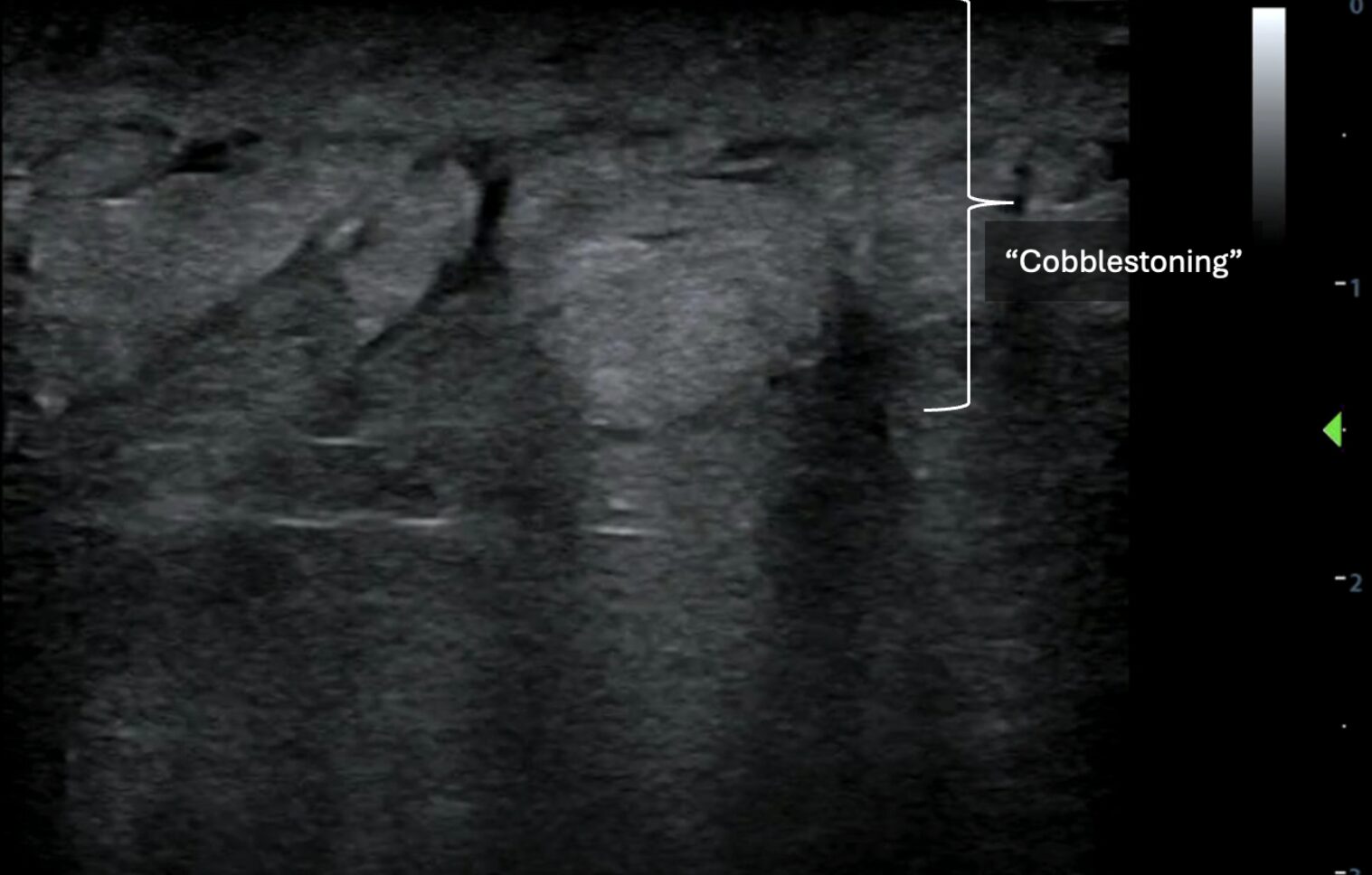
Video 5: Video clip of the above still image demonstrating “cobblestoning.” Images courtesy of Dr. Shepherd and Dr. Alerhand
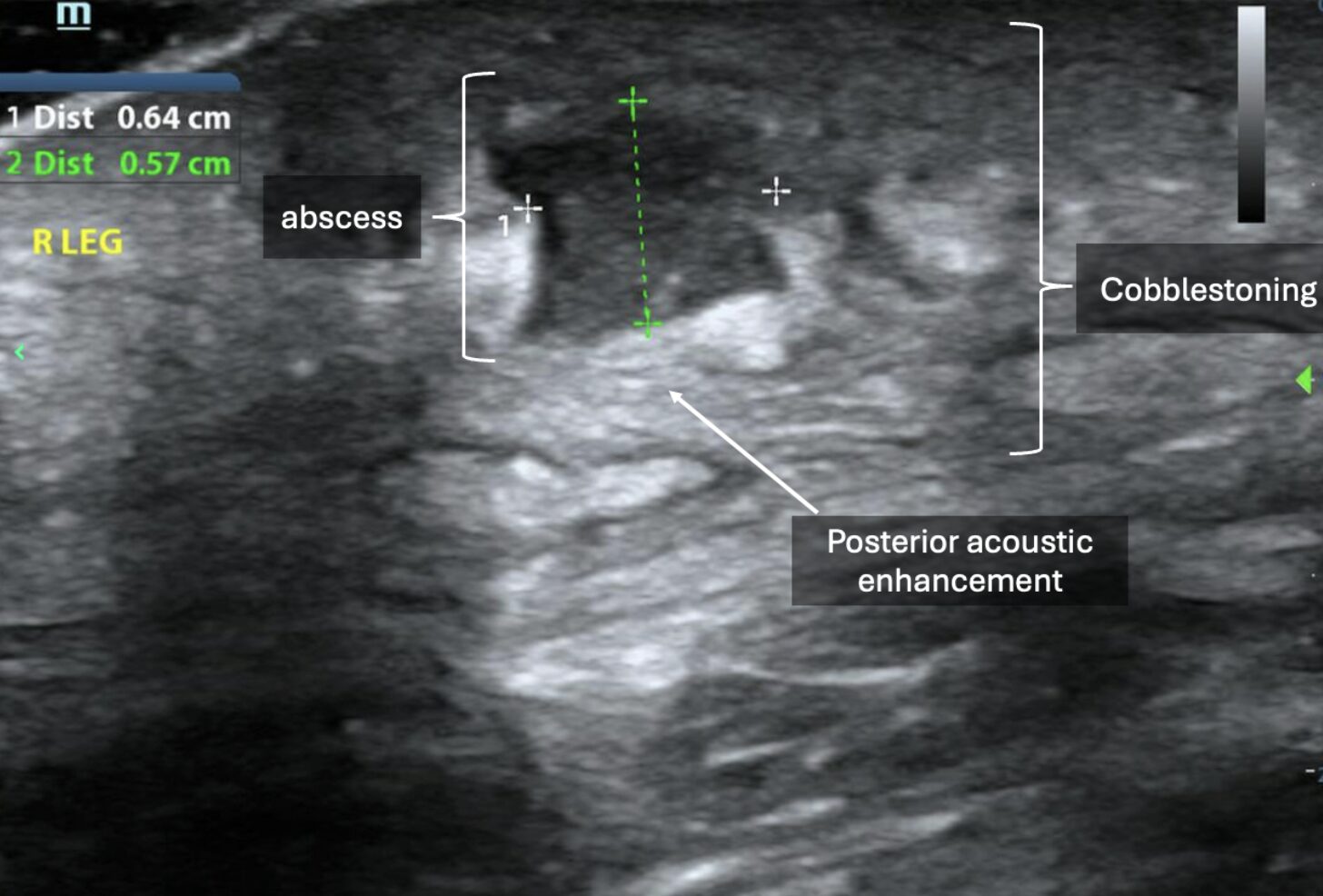
Sonographically, abscesses appear as collections of anechoic, hypoechoic, or heterogeneous material depending on the contents of the purulence. Often, there is notable posterior acoustic enhancement deep to these collections (Images 7-8, Video 6-7). Surrounding cobblestoning, as seen in cellulitis, may also be present. When downward, axial pressure is applied to the abscess using the probe, contents within the abscess may demonstrate a dynamic swirling motion referred to as “the squish sign” or “pus-istalsis” (Video 9).
If the abscess is noted to be draining superficially, there may be foci of air noted within the collection itself (Video 9). Unlike in NSTI, however, subcutaneous emphysema will not be present in the surrounding tissues, as it lacks channels or connections to the draining abscess. It is therefore important to ensure adequate depth when evaluating abscesses to ensure thorough assessment of extension and/or involvement of surrounding structures.
Image 7: Small, hypoechoic collection of material with posterior acoustic enhancement and adjacent cobblestoning. Images courtesy of Dr. Shepherd and Dr. Alerhand.
Video 6: In earlier, developing stages, abscesses may demonstrate irregular borders. Images courtesy of Dr. Shepherd and Dr. Alerhand
Image 8: In later clinical stages, abscesses may appear as more well-circumscribed collections with posterior acoustic enhancement.
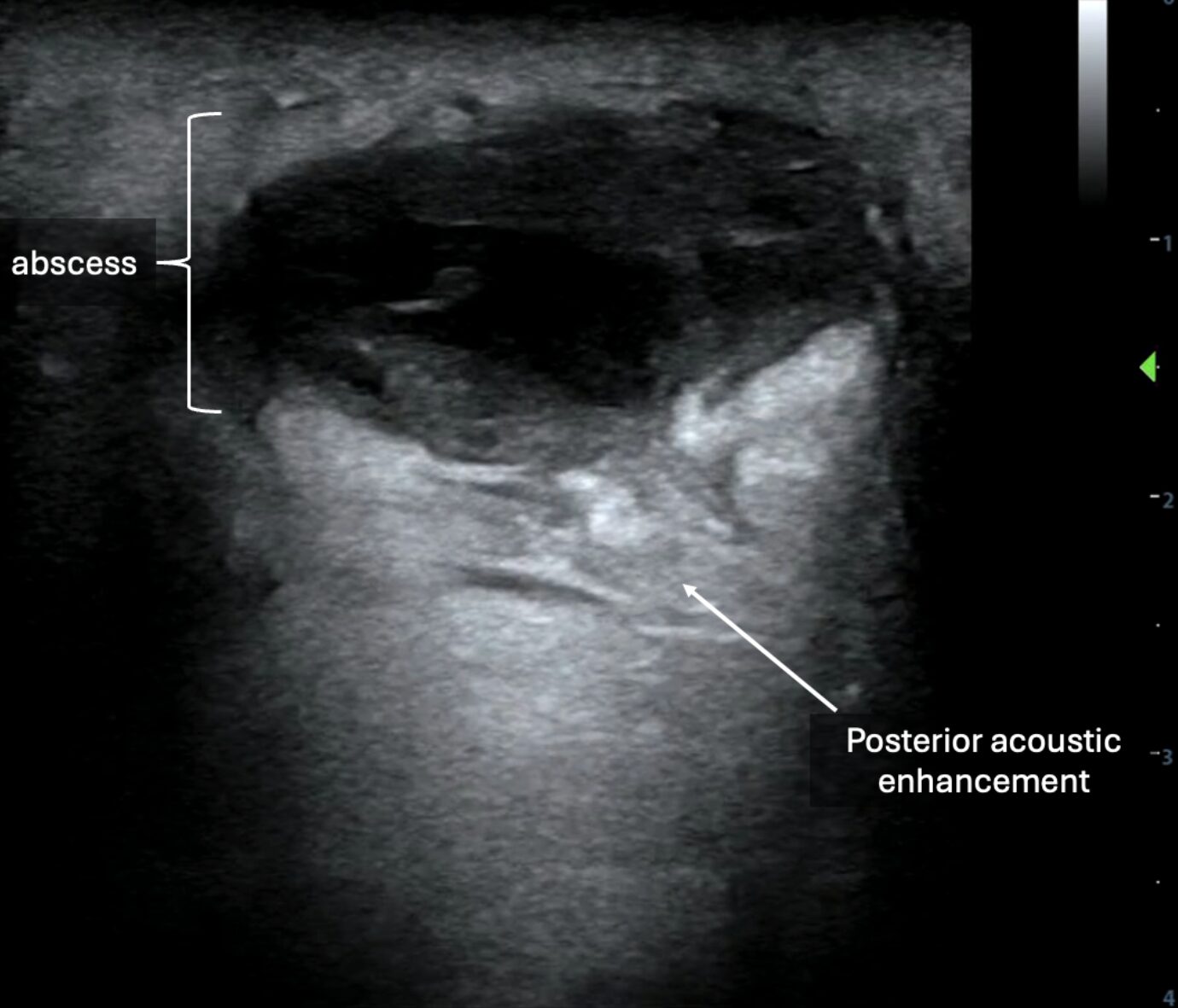
Video 7: Video of the above still image demonstrating an abscess.
Video 8: The use of color or power Doppler over the suspected “abscess” to demonstrate absence of flow (vs. with a vascular structure) is critical prior to considering incision and drainage.
Video 9: When downward, axial pressure is applied over the abscess with the probe, purulent material may demonstrate dynamic motion, colloquially referred to as “the squish sign” or “pus-istalsis.” Also note the subcutaneous air within this abscess’s distal fields, which likely appears due to active drainage to the skin surface that exposed the purulent pocket to the introduction of air.
Review of the literature
Necrotizing soft tissue infections are deep soft tissue infections affecting the fascial planes.1 The “hard” signs of NSTI, such as skin necrosis, hemorrhagic bullae, pain out of proportion to examination, and hypotension, are found at initial presentation in less than half of cases, often contributing to delayed diagnosis.4 When these hard signs are present on initial presentation, they are often associated with higher mortality rates.5
Timely diagnosis of NSTI can be challenging. In its early stages, it may be difficult to distinguish from other superficial soft-tissue infections, such as cellulitis. While clinical decision-making tools like the LRINEC score have been studied, they have variable specificities and sensitivities, and thus they should not be used in isolation to exclude the diagnosis of NSTI. An LRINEC score > 6 (which is the intermediate risk group for necrotizing soft tissue infection, NSTI) has a sensitivity of 68.2% and specificity of 84.8%, while an LRINEC score ≥ 8 has a sensitivity of 40.8% and specificity of 94.9%.6
While imaging, such as computed tomography (CT), is often requested by the specialist consultant prior to performing the operative debridement, NSTI is a clinical diagnosis.7 The sensitivity of CT in diagnosing NSTI is reported as 88.5%, while the specificity is 93.3%.7 Furthermore, obtaining imaging may be challenging and can delay surgical intervention, which is both diagnostic and therapeutic. Patients must be stable enough to leave the patient care area for the CT scan, which may not be obtained expeditiously in a busy emergency department.
A 2023 systematic review found that POCUS has comparable sensitivity to CT and much higher sensitivity than clinical signs and the LRINEC score for diagnosing NSTI, with overall sensitivity ranging from 85.4-100% and specificity ranging from 44.7-98.2%.2 Of the findings described above that are concerning for NSTI, fluid accumulation in the deep fascia layer had the highest sensitivity (85.4%), and subcutaneous emphysema had the highest specificity (98.2%).2,8 The presence of any one of the classic three findings listed above (subcutaneous thickening, the presence of fascial fluid, and subcutaneous emphysema) suggests NSTI, and in combination with lab results and clinical suspicion, is more helpful than relying on any single finding alone.2 Therefore, POCUS findings in conjunction with the clinical picture could serve as a surrogate for CT findings when CT is not practical or readily available in an ED. It also helps expedite bedside diagnosis and prompt early surgical consultation.
Case Resolution
A POCUS assessment of the right lower extremity was notable for diffuse subcutaneous thickening and fluid layering along fascial planes. The patient was started on broad-spectrum antibiotics and intravenous fluids. General Surgery was consulted for emergent debridement. On initial discussion with General Surgery, a CT scan of the right lower extremity was recommended. However, on repeat POCUS with the General Surgery consultant present, subcutaneous fluid accumulation along the fascial planes was now extending into previously unaffected regions, and subcutaneous emphysema was newly identified. The patient was taken to the operating room for surgical debridement, followed by subsequent monitoring and medical treatment in the surgical intensive care unit.
Take-Home Points
Timely diagnosis of NSTI can be challenging, especially in patients with chronic comorbidities that diminish their ability to localize and quantify their symptoms of pain, swelling, and erythema. CT is not a perfect test for this disease process. Soft tissue POCUS is a real-time, dynamic, repeatable, and noninvasive bedside adjunct that can aid in the rapid diagnosis of NSTI by evaluating for the presence of specific findings, including subcutaneous thickening, subcutaneous emphysema (air), and fascial fluid.
References
- Gan RK, Sanchez Martinez A, Abu Hasan MA, Castro Delgado R, Arcos González P. Point-of-care ultrasonography in diagnosing necrotizing fasciitis-a literature review. J Ultrasound. 2023 Jun;26(2):343-353. doi: 10.1007/s40477-022-00761-5. Epub 2023 Jan 24. PMID: 36694072; PMCID: PMC10247625.
- Marks A, Patel D, Sundaram T, Johnson J, Gottlieb M. Ultrasound for the diagnosis of necrotizing fasciitis: A systematic review of the literature. Am J Emerg Med. 2023 Mar;65:31-35. doi: 10.1016/j.ajem.2022.12.037. Epub 2022 Dec 22. PMID: 36580698.
- Tso DK, Singh AK. Necrotizing fasciitis of the lower extremity: imaging pearls and pitfalls. Br J Radiol. 2018 Jul;91(1088):20180093. doi: 10.1259/bjr.20180093. Epub 2018 Mar 28. PMID: 29537292; PMCID: PMC6209465.
- Chan T, Yaghoubian A, Rosing D, Kaji A, de Virgilio C. Low sensitivity of physical examination findings in necrotizing soft tissue infection is improved with laboratory values: a prospective study. Am J Surg. 2008 Dec;196(6):926-30; discussion 930. doi: 10.1016/j.amjsurg.2008.07.025. PMID: 19095111.
- Stevens DL, Bryant AE. Necrotizing Soft-Tissue Infections. N Engl J Med. 2017 Dec 7;377(23):2253-2265. doi: 10.1056/NEJMra1600673. PMID: 29211672.
- Fernando SM, Tran A, Cheng W, Rochwerg B, Kyeremanteng K, Seely AJE, Inaba K, Perry JJ. Necrotizing Soft Tissue Infection: Diagnostic Accuracy of Physical Examination, Imaging, and LRINEC Score: A Systematic Review and Meta-Analysis. Ann Surg. 2019 Jan;269(1):58-65. doi: 10.1097/SLA.0000000000002774. PMID: 29672405.
- Pelletier J, Gottlieb M, Long B, Perkins JC Jr. Necrotizing Soft Tissue Infections (NSTI): Pearls and Pitfalls for the Emergency Clinician. J Emerg Med. 2022 Apr;62(4):480-491. doi: 10.1016/j.jemermed.2021.12.012. Epub 2022 Jan 31. PMID: 35115188.
- Lin CN, Hsiao CT, Chang CP, Huang TY, Hsiao KY, Chen YC, Fann WC. The Relationship Between Fluid Accumulation in Ultrasonography and the Diagnosis and Prognosis of Patients with Necrotizing Fasciitis. Ultrasound Med Biol. 2019 Jul;45(7):1545-1550. doi: 10.1016/j.ultrasmedbio.2019.02.027. Epub 2019 Apr 26. PMID: 31031033.





