
Author: Brit Long, MD (@long_brit) // Reviewed by Alex Koyfman, MD (@EMHighAK)
The AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN published a de novo guideline providing recommendations for evaluation, management, and follow-up of adults patients with PE. This post will summarize these new guidelines.
Our Big Takeaways:
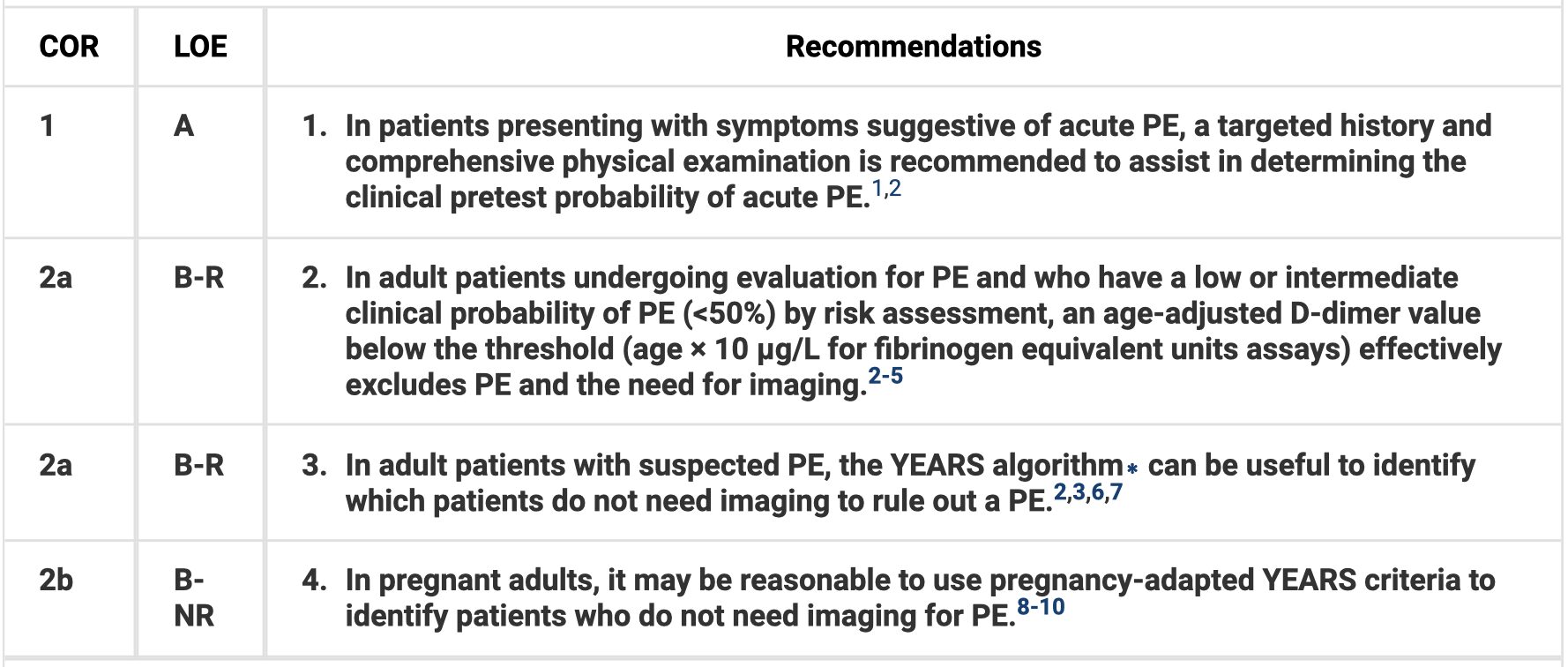
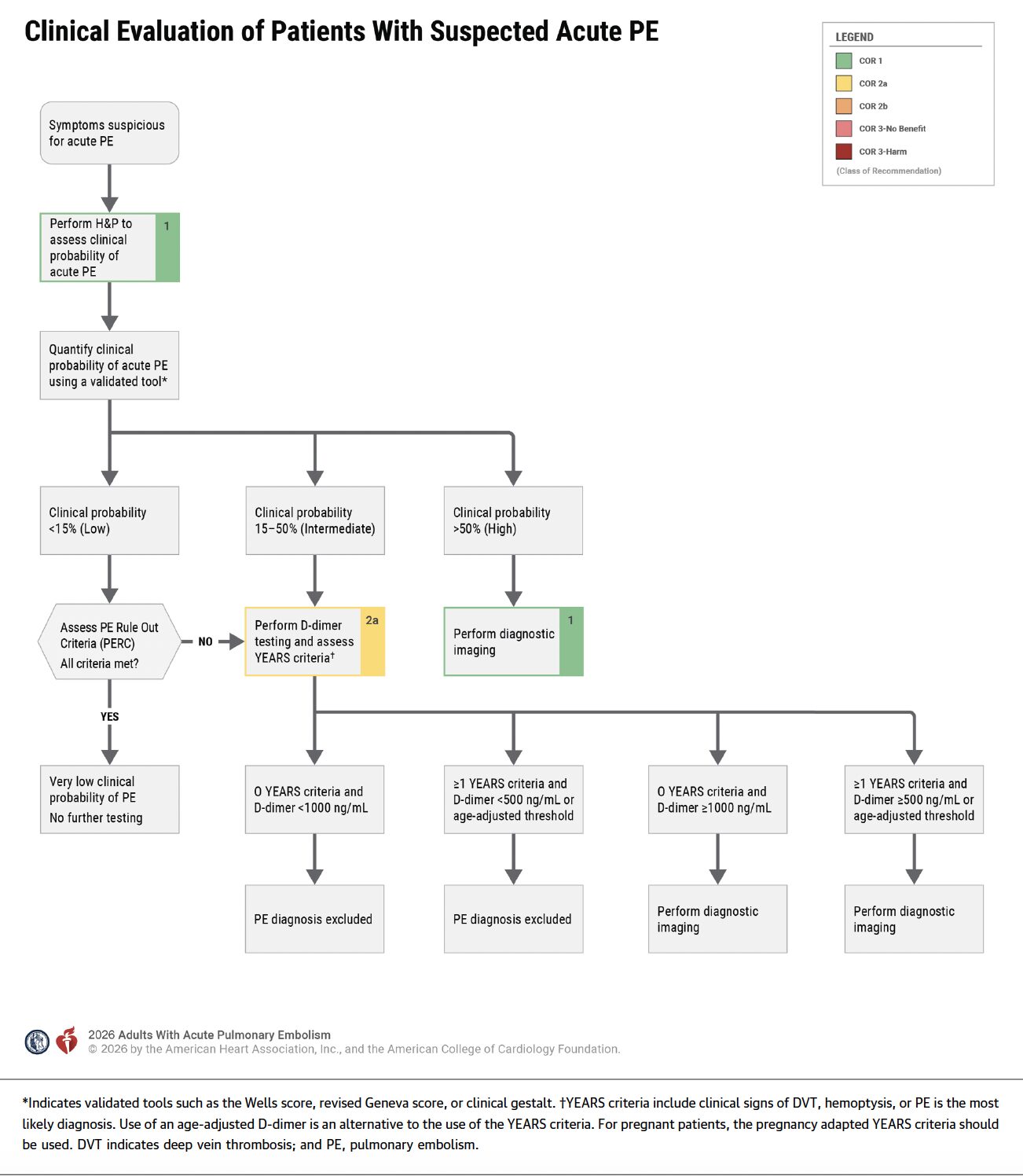
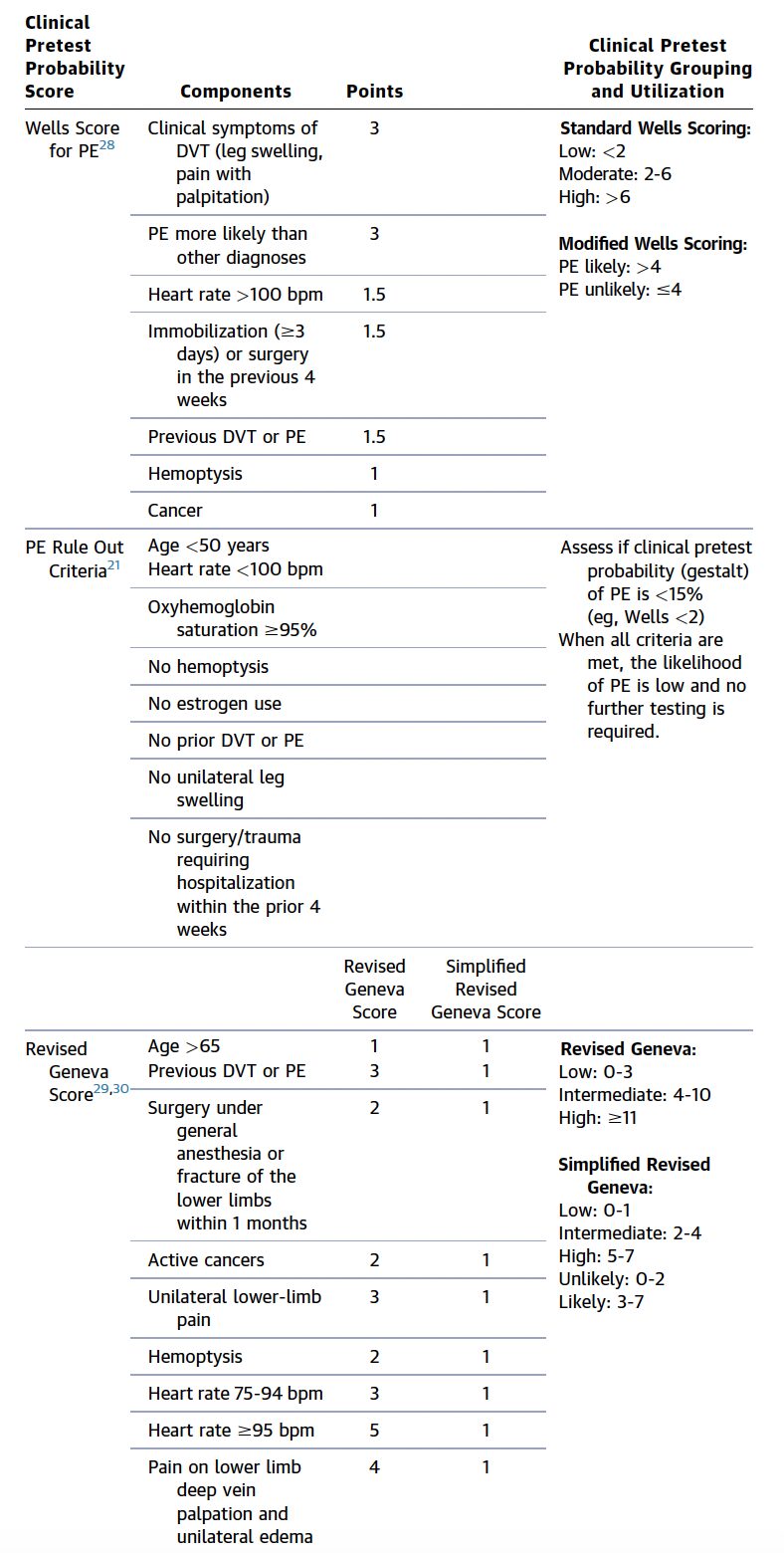
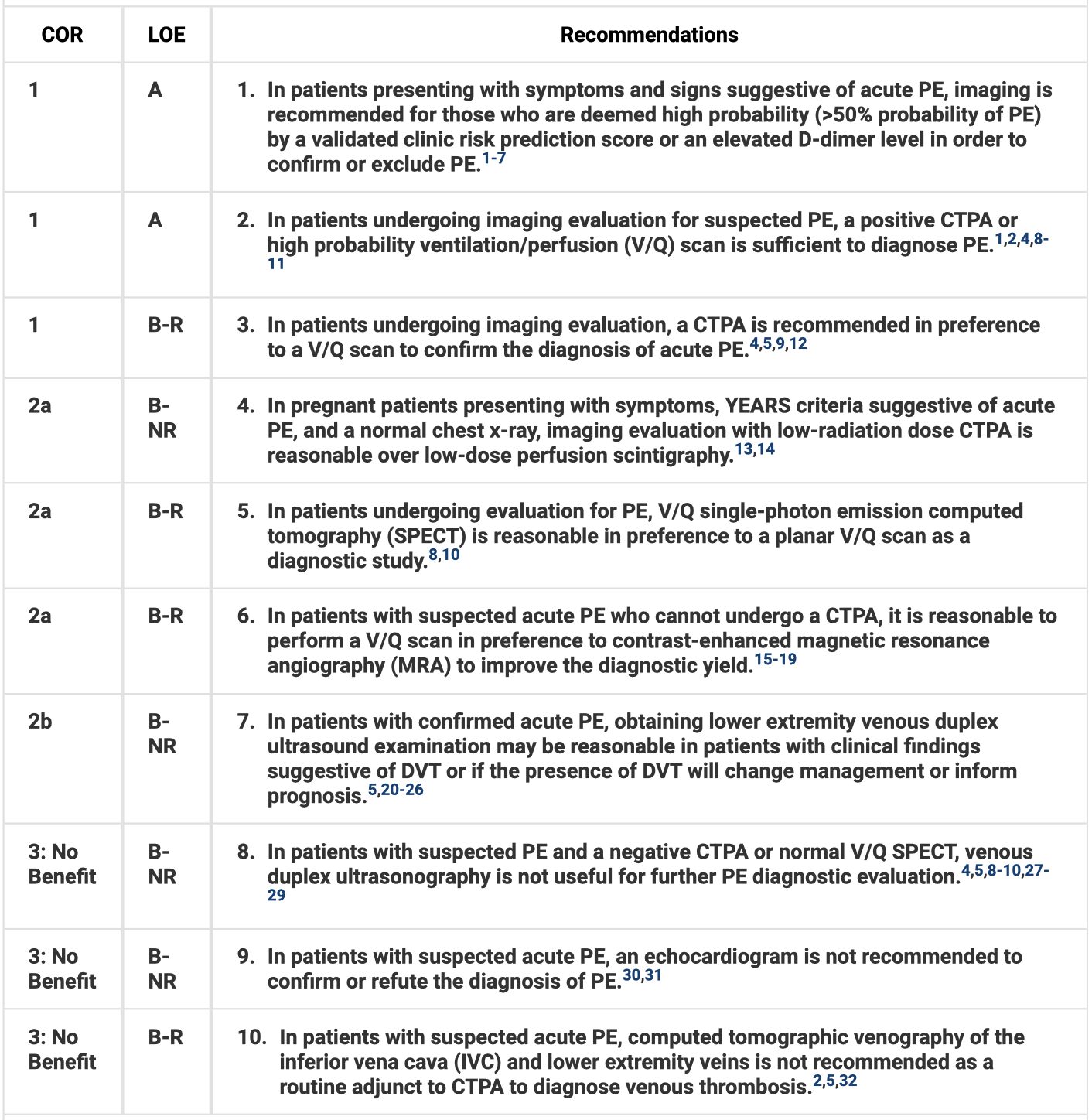
- YEARS is useful in determining need for imaging, including during pregnancy. Use age-adjusted D-dimer for low or intermediate risk patients. CTPA is the imaging test of choice for high probability patients, including pregnancy. Do not use echo to confirm or exclude diagnosis of PE.
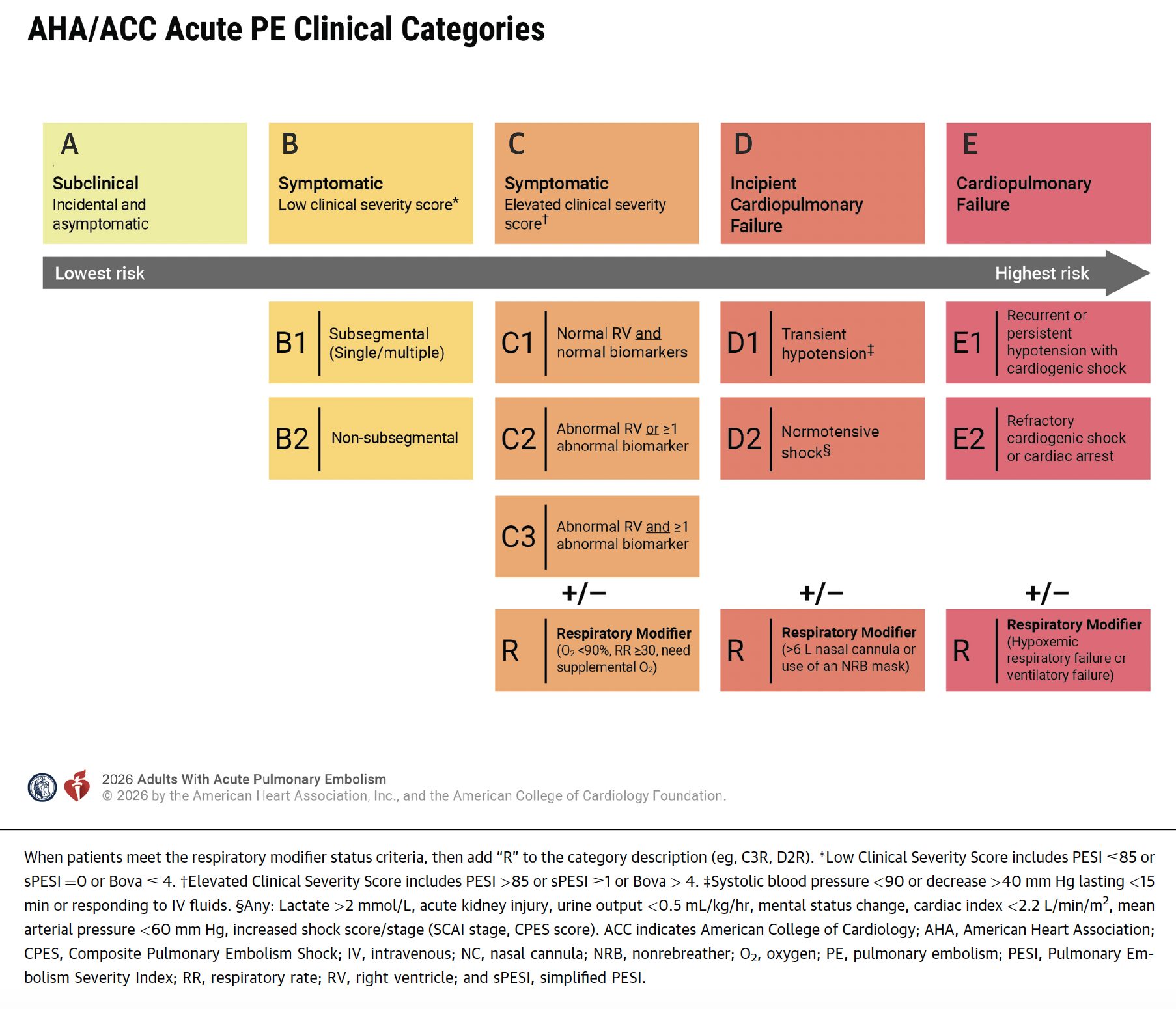
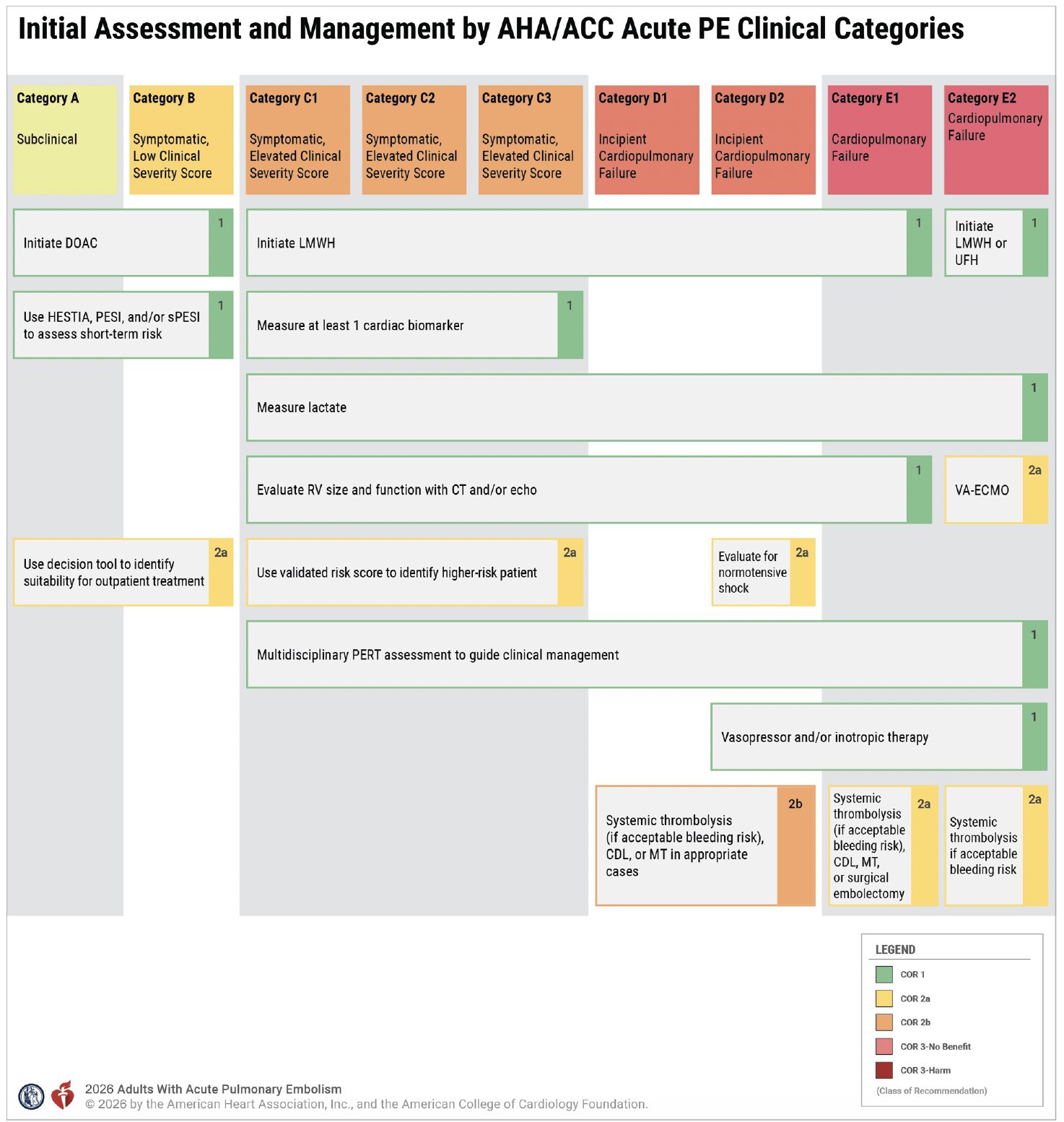
- There are 5 PE clinical categories: a) subclinical, b) symptomatic with low clinical severity, c) symptomatic with elevated clinical severity, d) incipient cardiopulmonary failure, and e) cardiopulmonary failure.
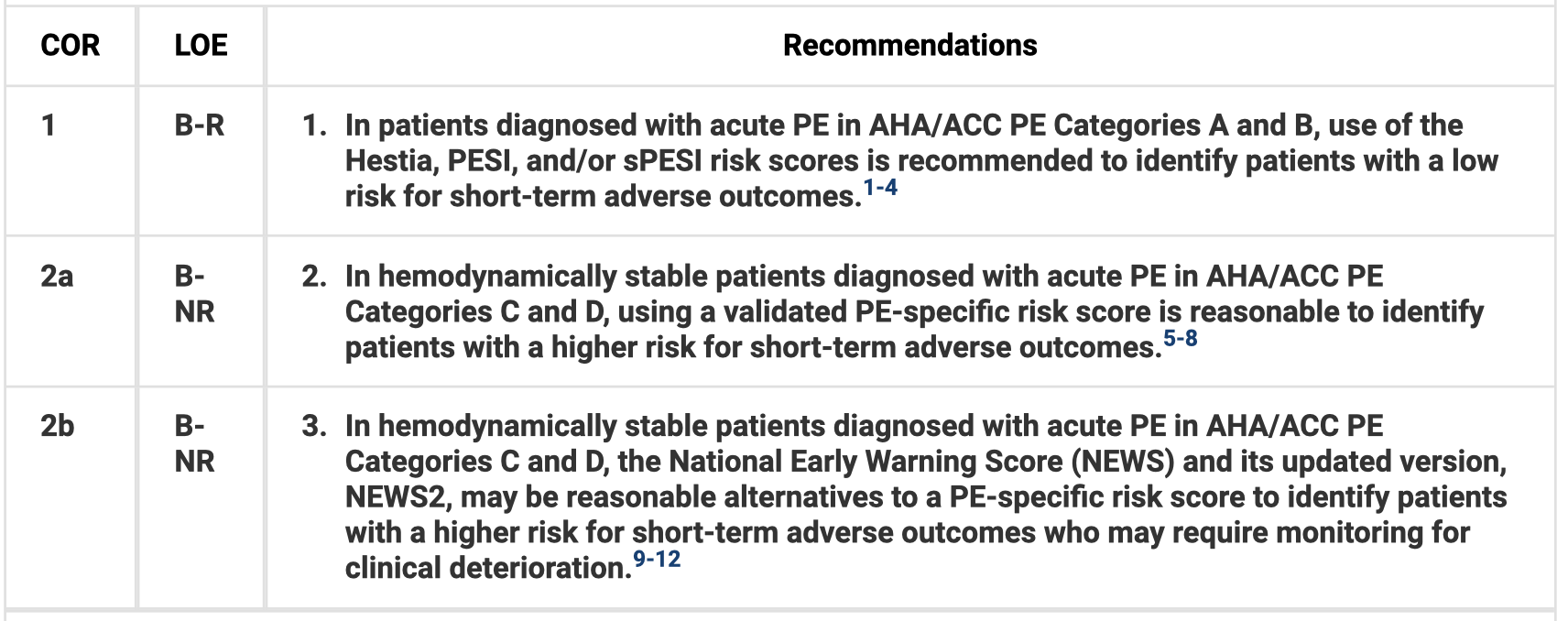
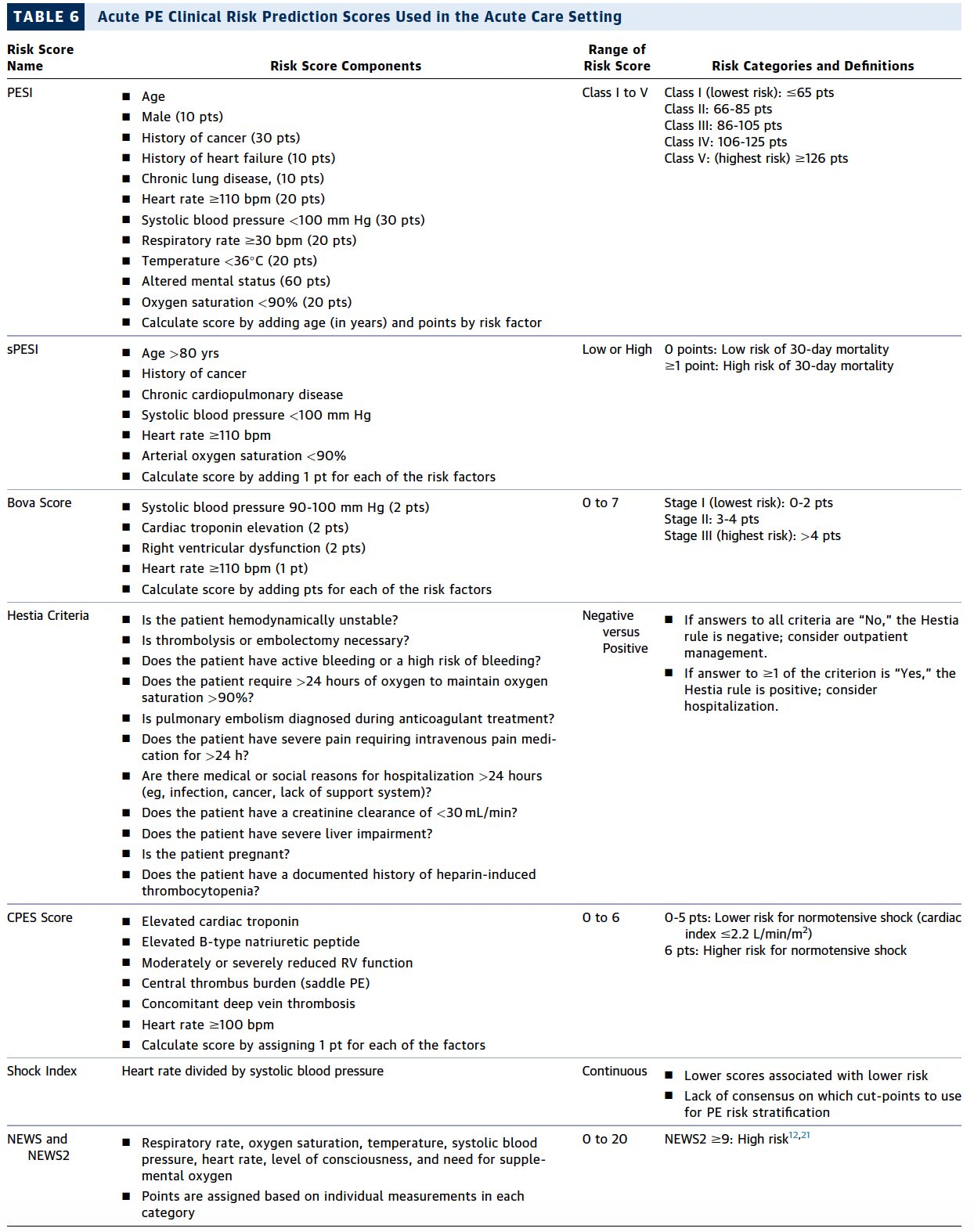
- For patients with categories a and b, use Hestia, PESI, or sPESI to identify low risk patients for adverse outcomes. Biomarkers (troponin, BNP, lactate) can assist in risk stratifying for adverse outcomes. US RV assessment can be helpful in short-term risk stratification in acute PE with symptoms, elevated biomarkers, or hemodynamic issues (including transient).
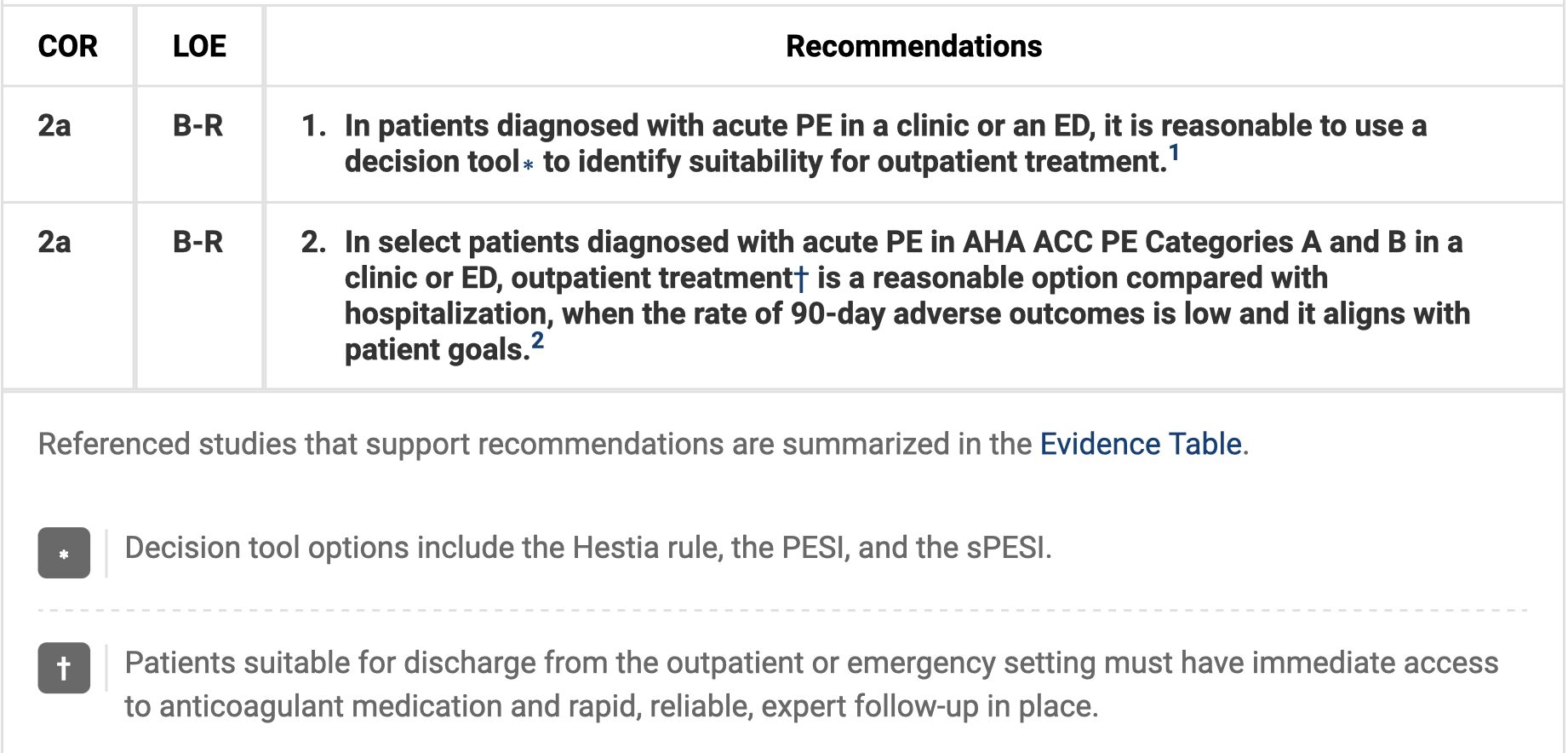
- Outpatient treatment is reasonable in appropriate low risk patients (categories a and b). Use a DOAC for these patients.
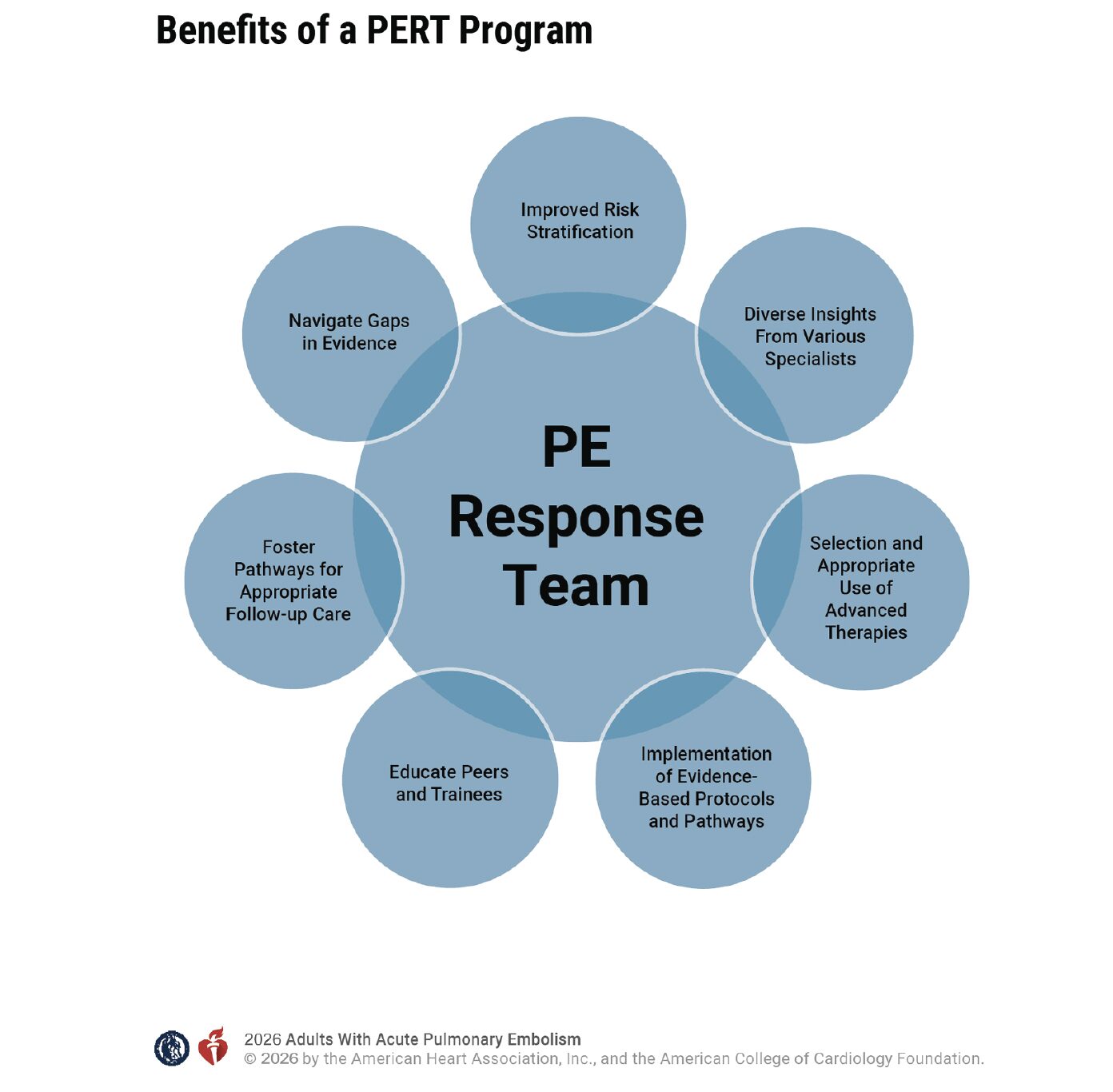
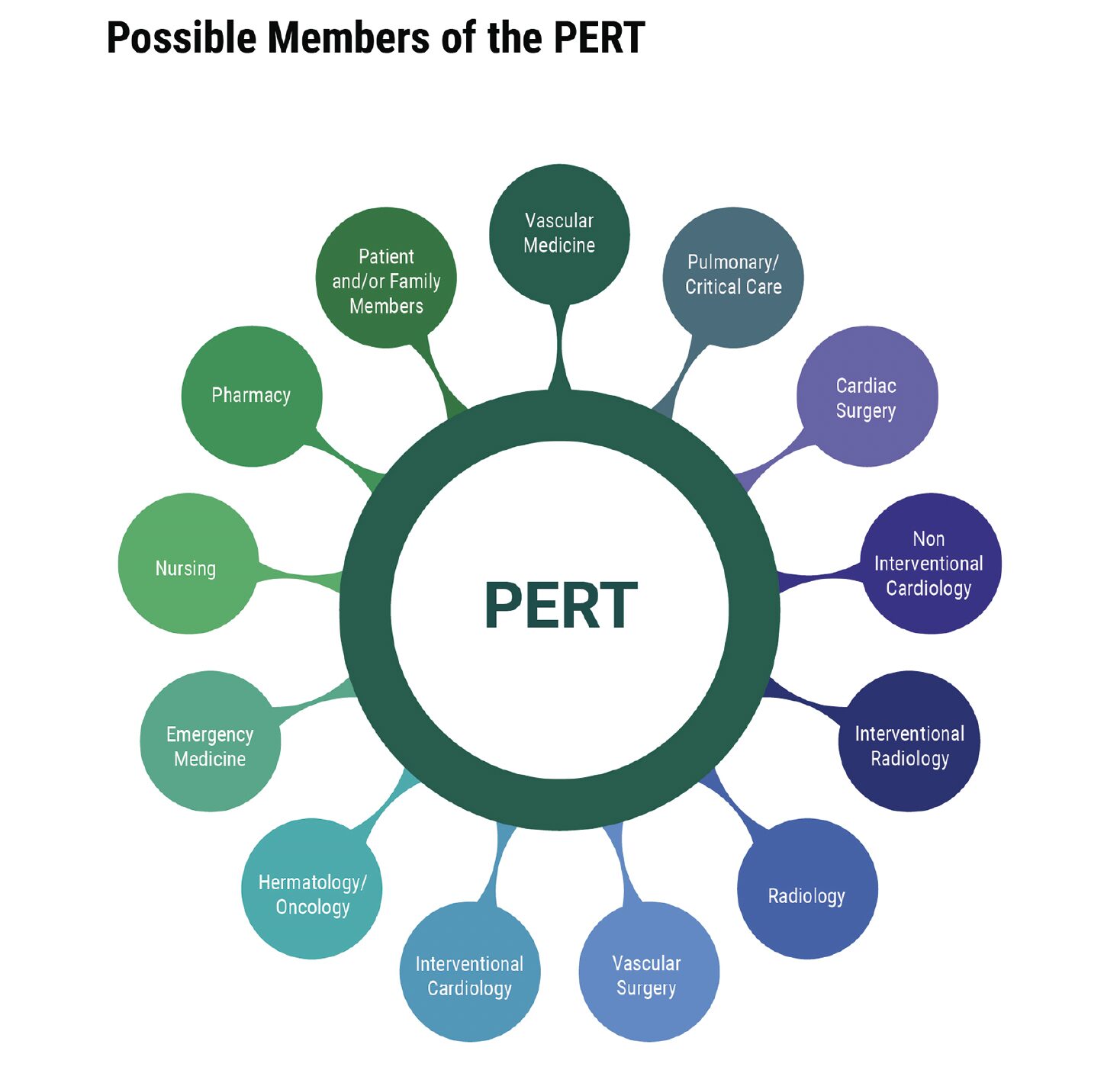
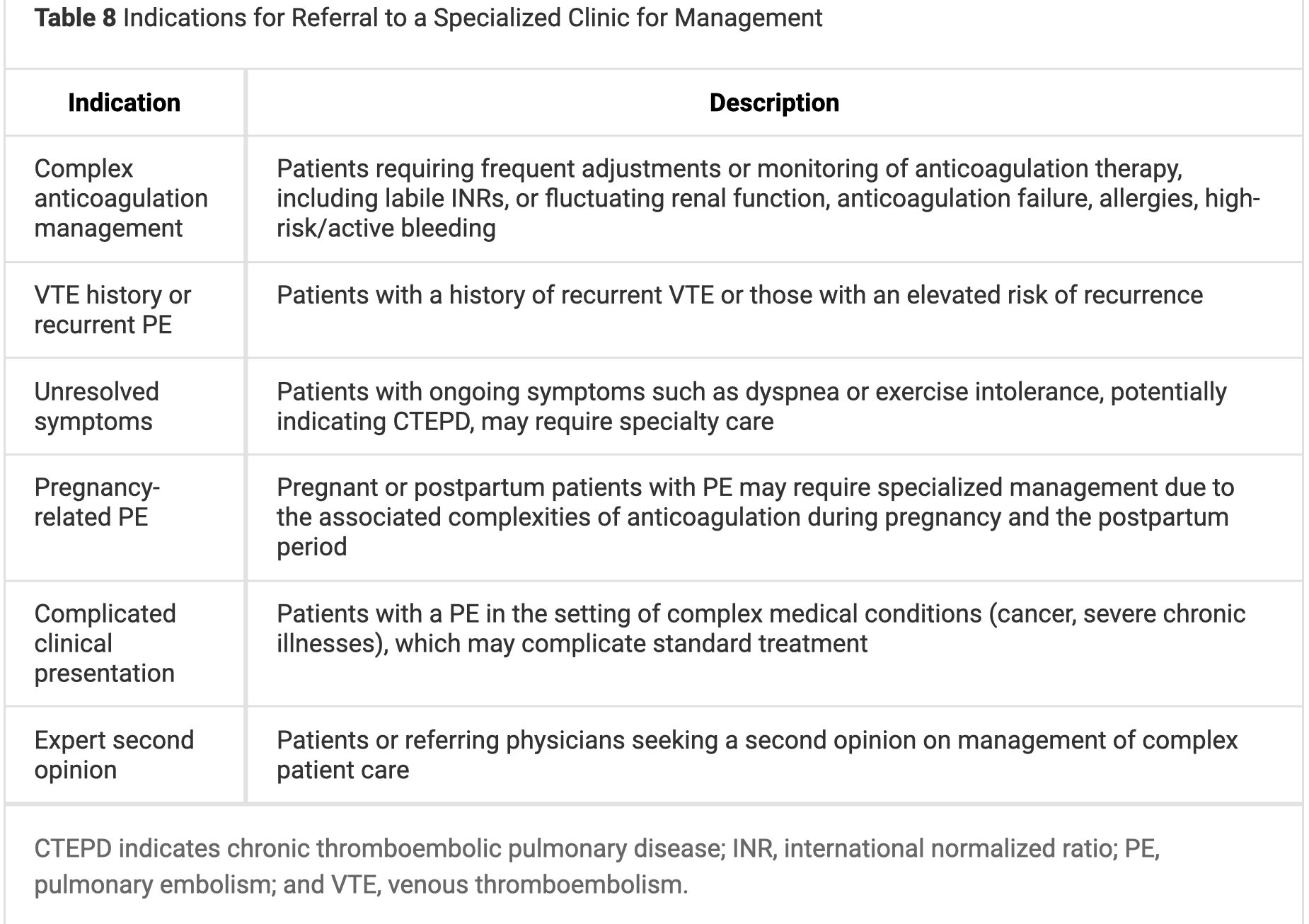
- PERT may be helpful in those with PE at increased risk of adverse outcomes.
- LMWH is recommended over UFH in almost all patients categories c to e.
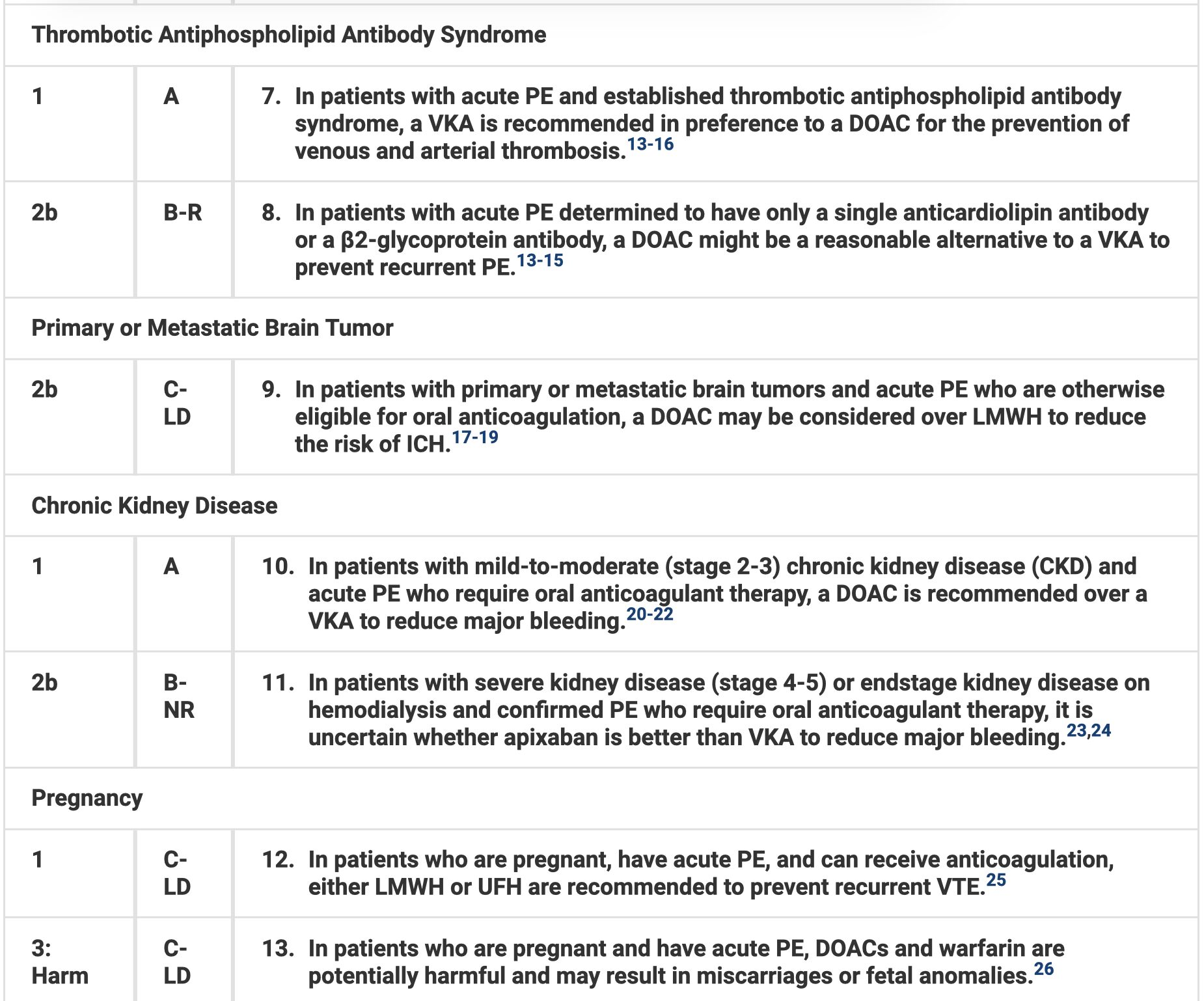
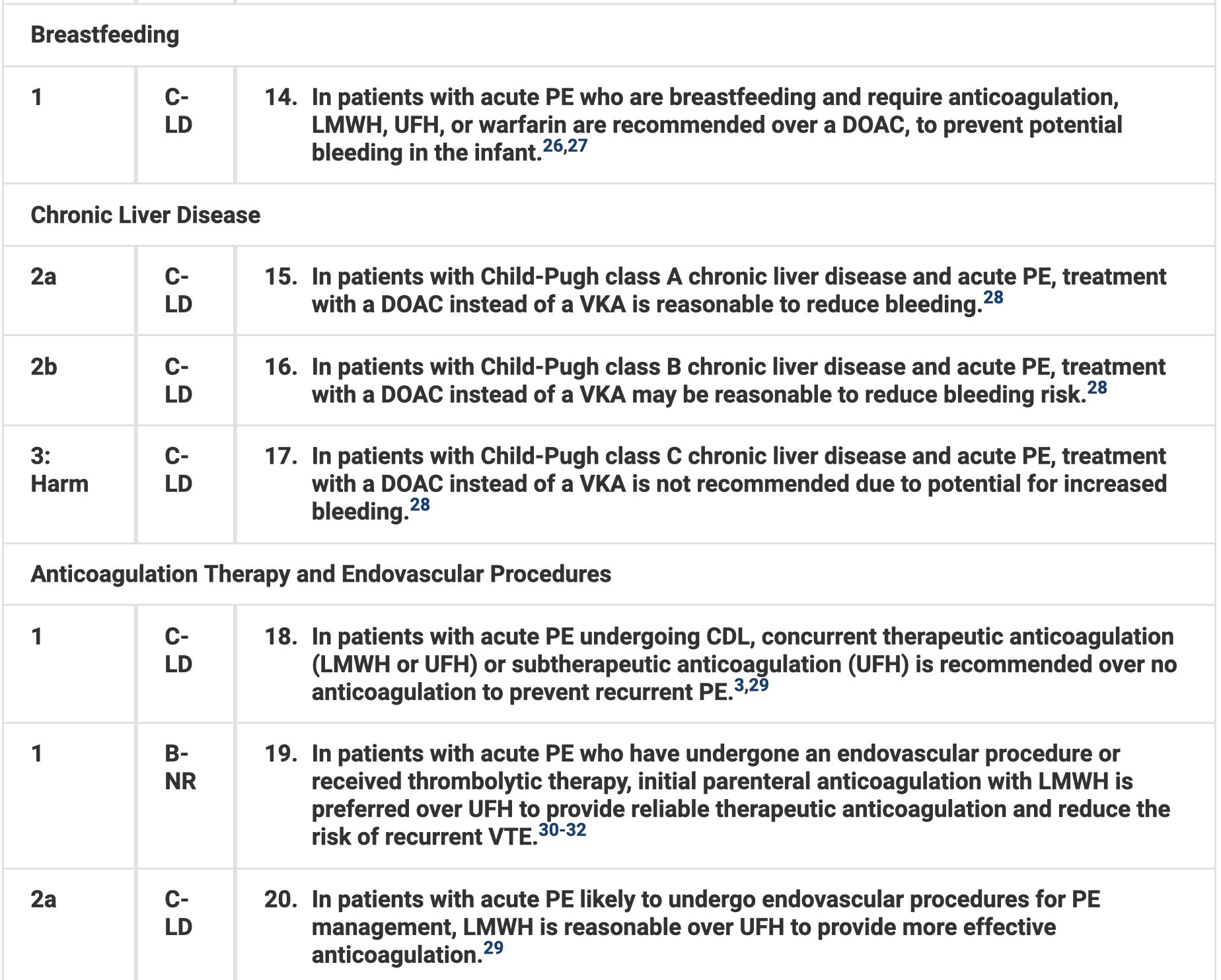
- DOACs should be used in those with CKD or liver disease. In pregnancy or breastfeeding patients, use LMWH or UFH.
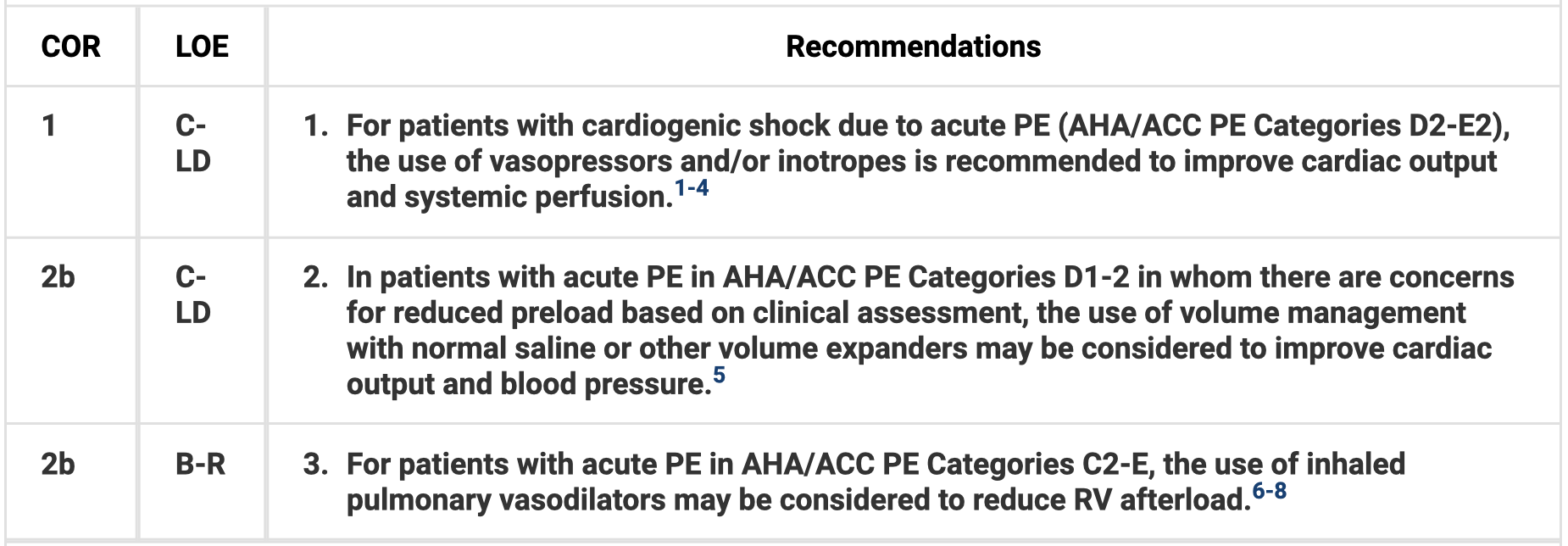
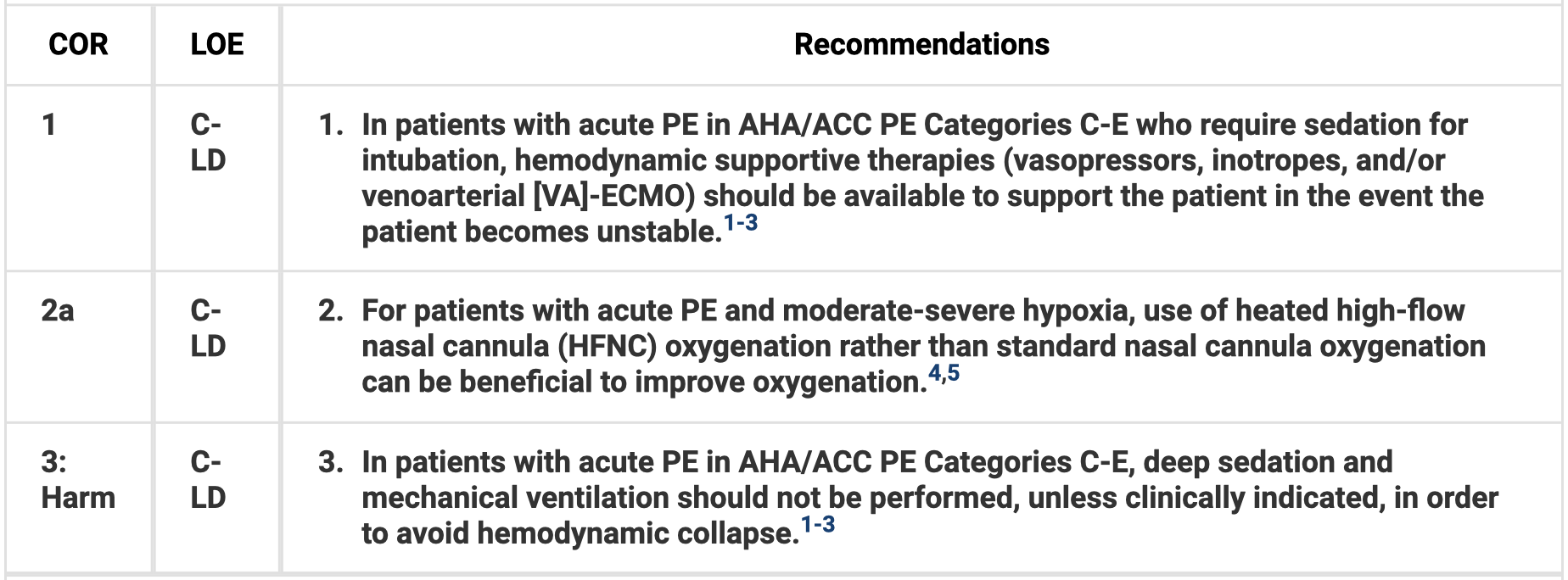
- For those with cardiogenic shock, use vasopressors and/or inotropes. Use HFNC rather than standard nasal cannula oxygenation for moderate-to-severe hypoxia. Avoid deep sedation and mechanical ventilation if possible to avoid hemodynamic collapse.
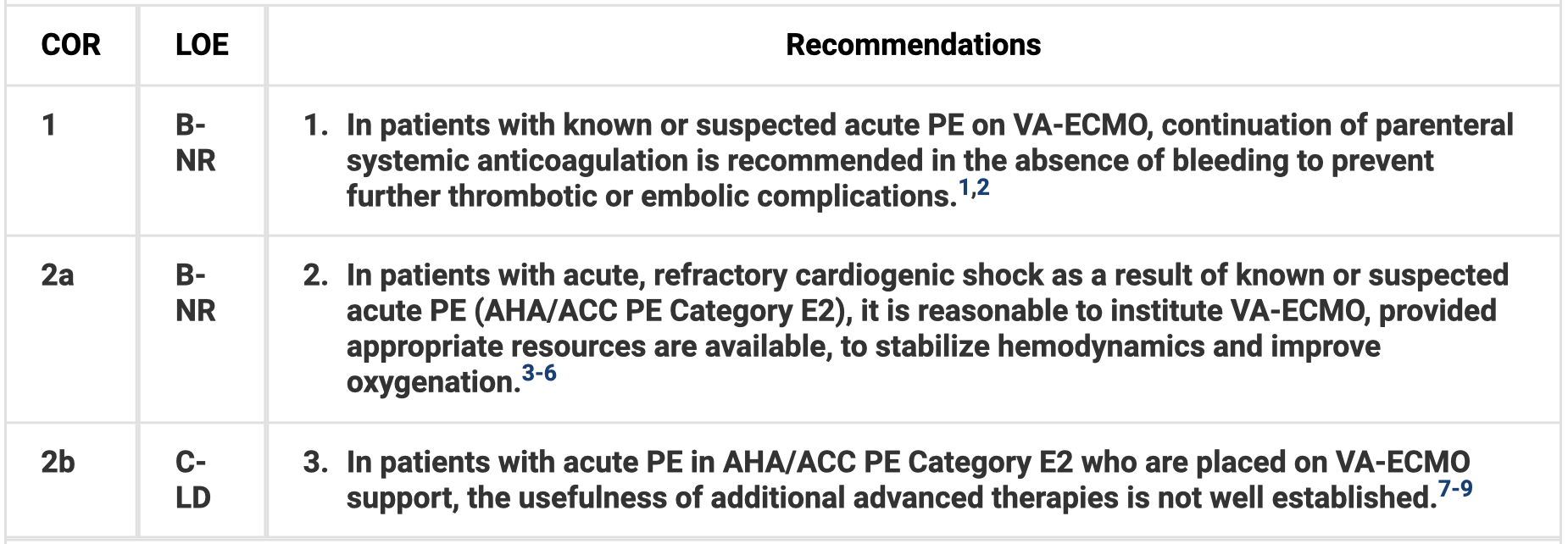
- VA-ECMO is reasonable in those with refractory cardiogenic shock with known/suspected PE.
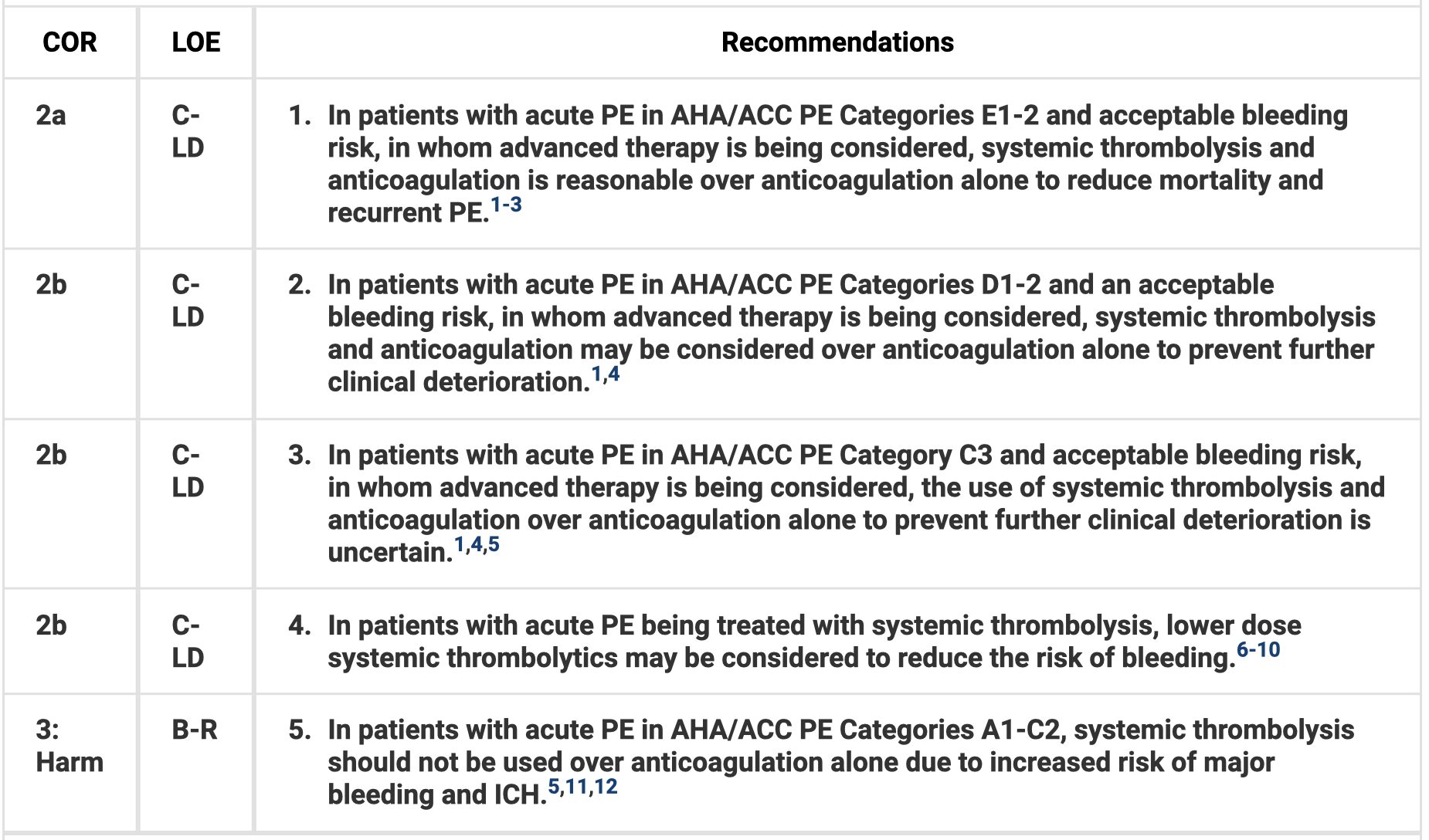
- Administer systemic thrombolysis in those with cardiopulmonary failure from PE. Consider thrombolysis in those with incipient cardiopulmonary failure (transient hypotension or normotensive shock) and acceptable bleeding risk.
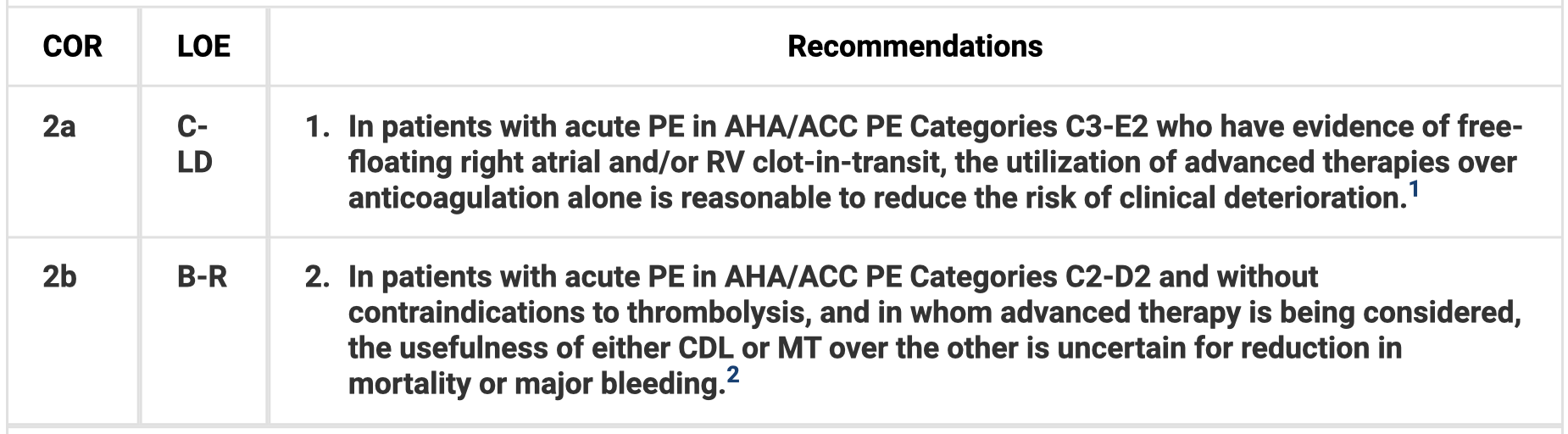
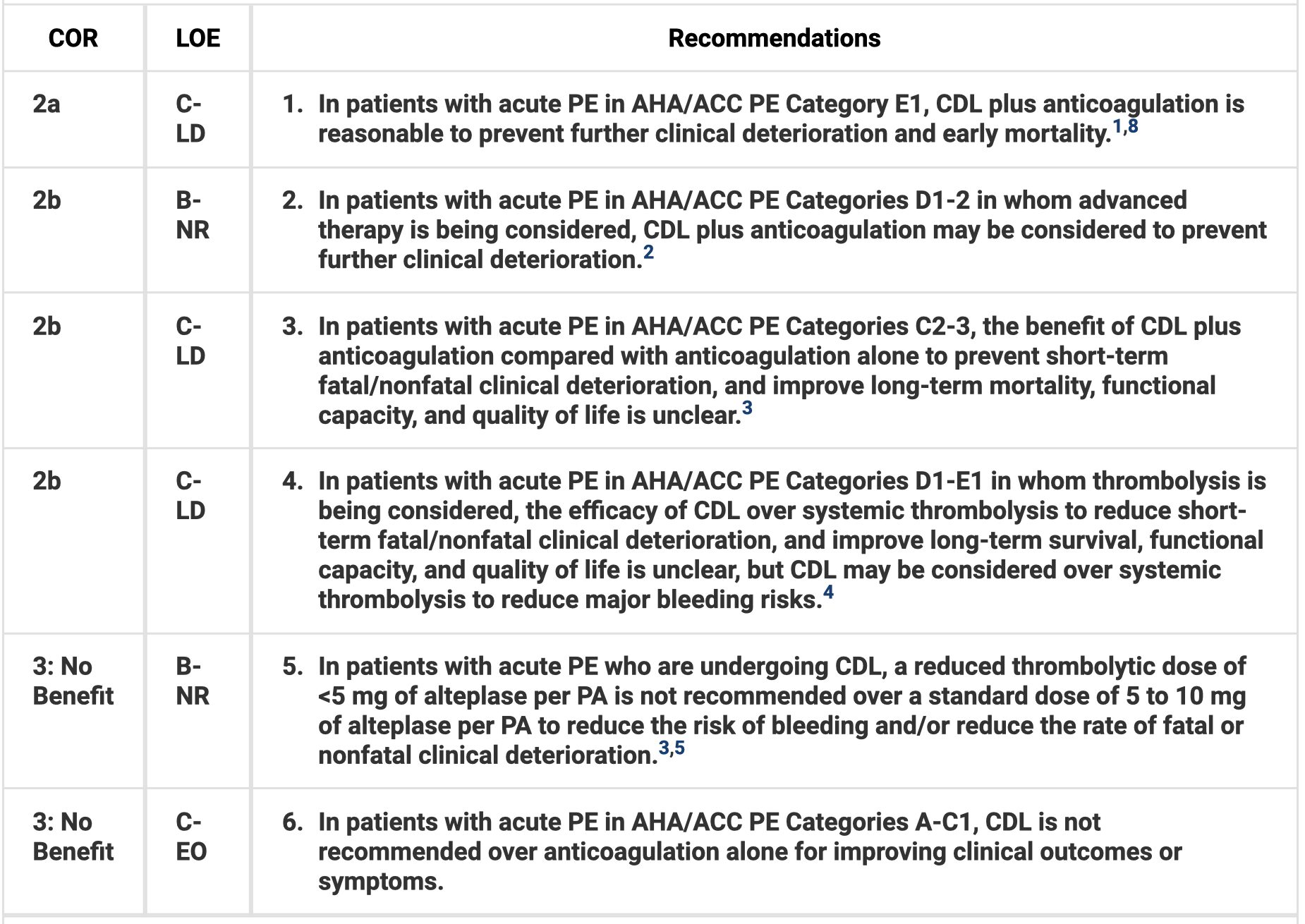
- The benefits of catheter-directed thrombolysis (CDT) plus anticoagulation are unclear in category c (symptomatic with elevated clinical severity), but CDT with anticoagulation is reasonable in category e1 (cardiopulmonary failure with recurrent or persistent hypotension with cardiogenic shock) and can be considered in those with incipient cardiopulmonary failure to prevent further deterioration. CDT is not recommended in categories a and b.
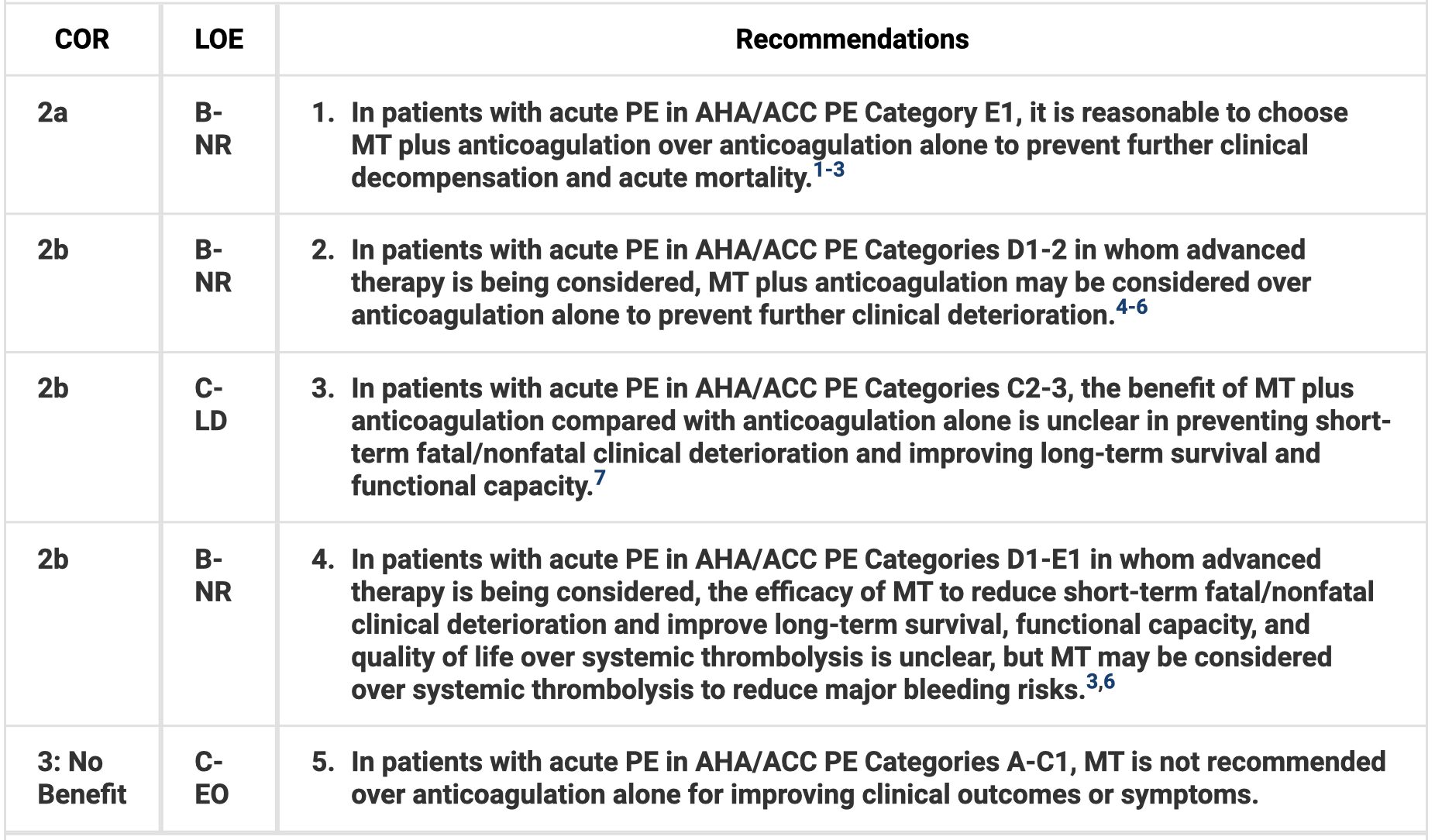
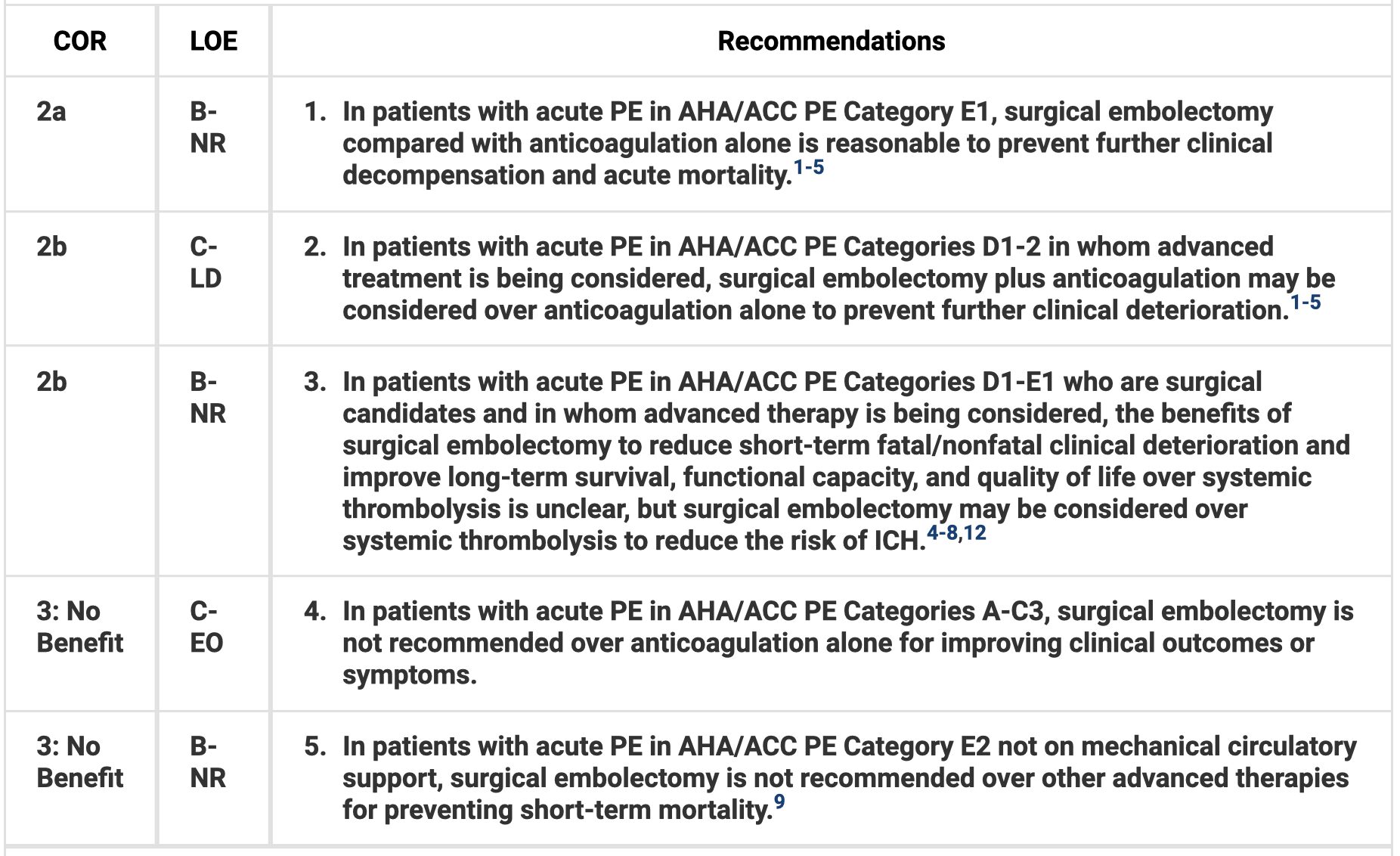
- Mechanical thrombectomy (MT) with anticoagulation or surgical embolectomy (SE) is reasonable in category e1. MT plus anticoagulation or SE may be considered in certain patients with incipient cardiopulmonary failure.
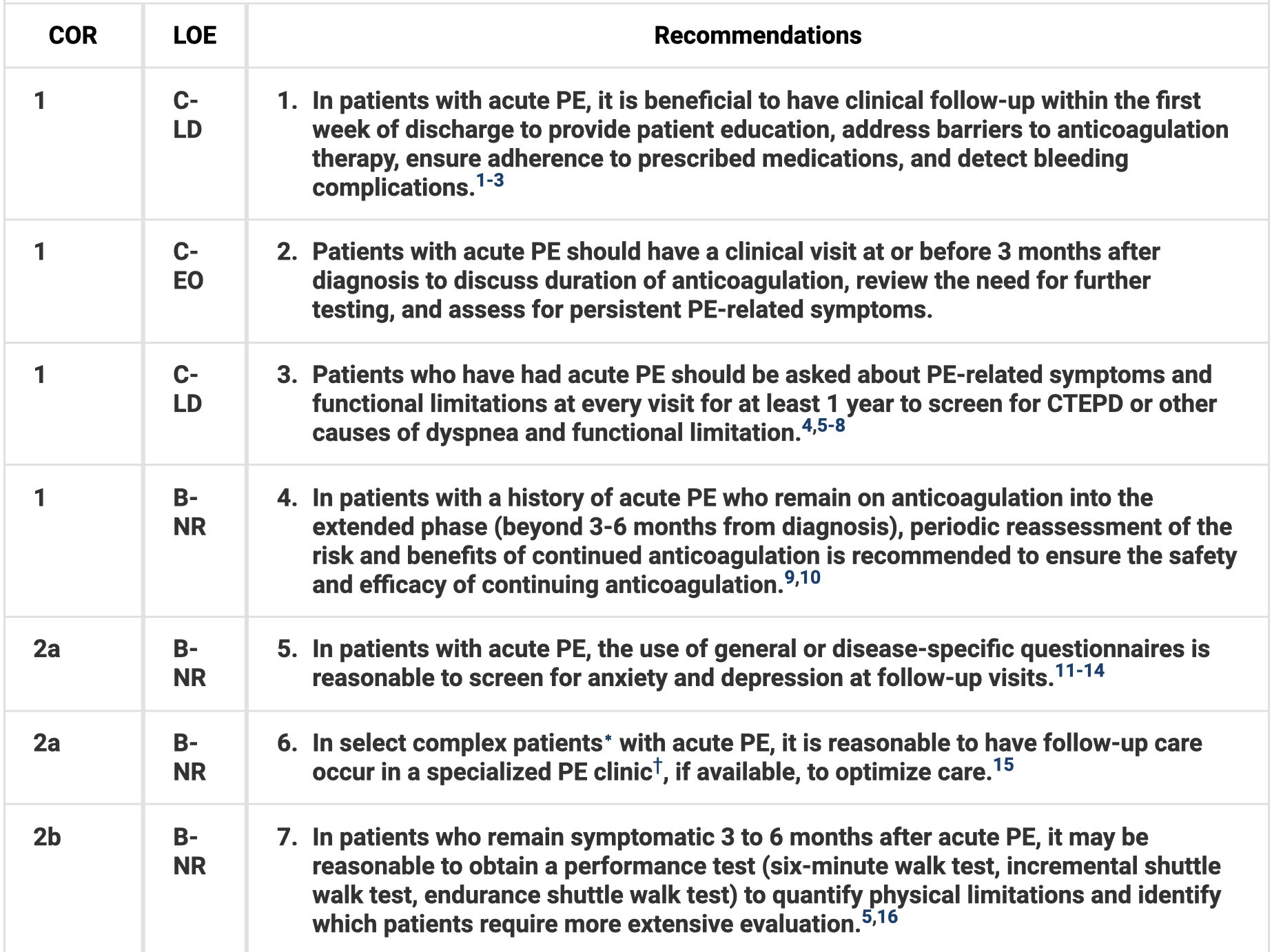
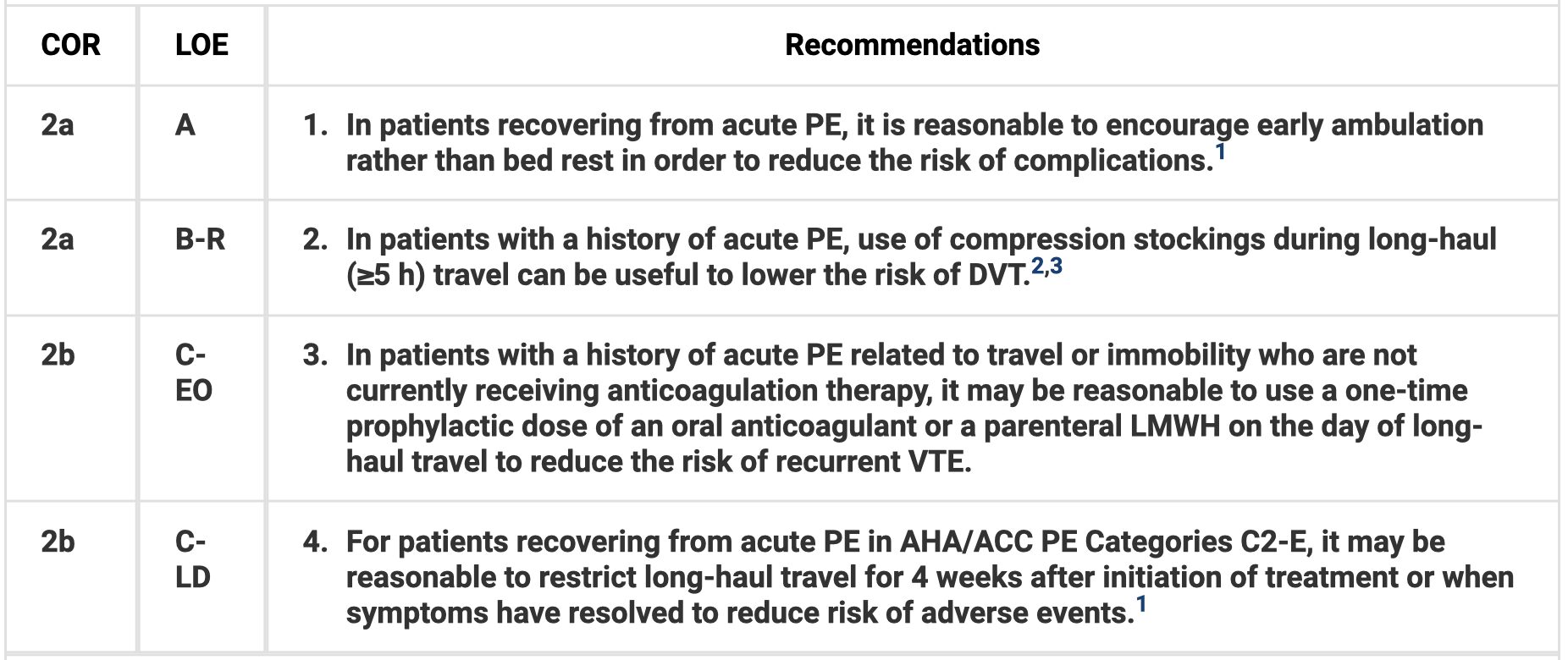
- In patients with acute PE, follow up within the first week of discharge can be helpful. Patients should have a clinical visit at or before 3 months to discuss duration of anticoagulation. Encourage early ambulation.
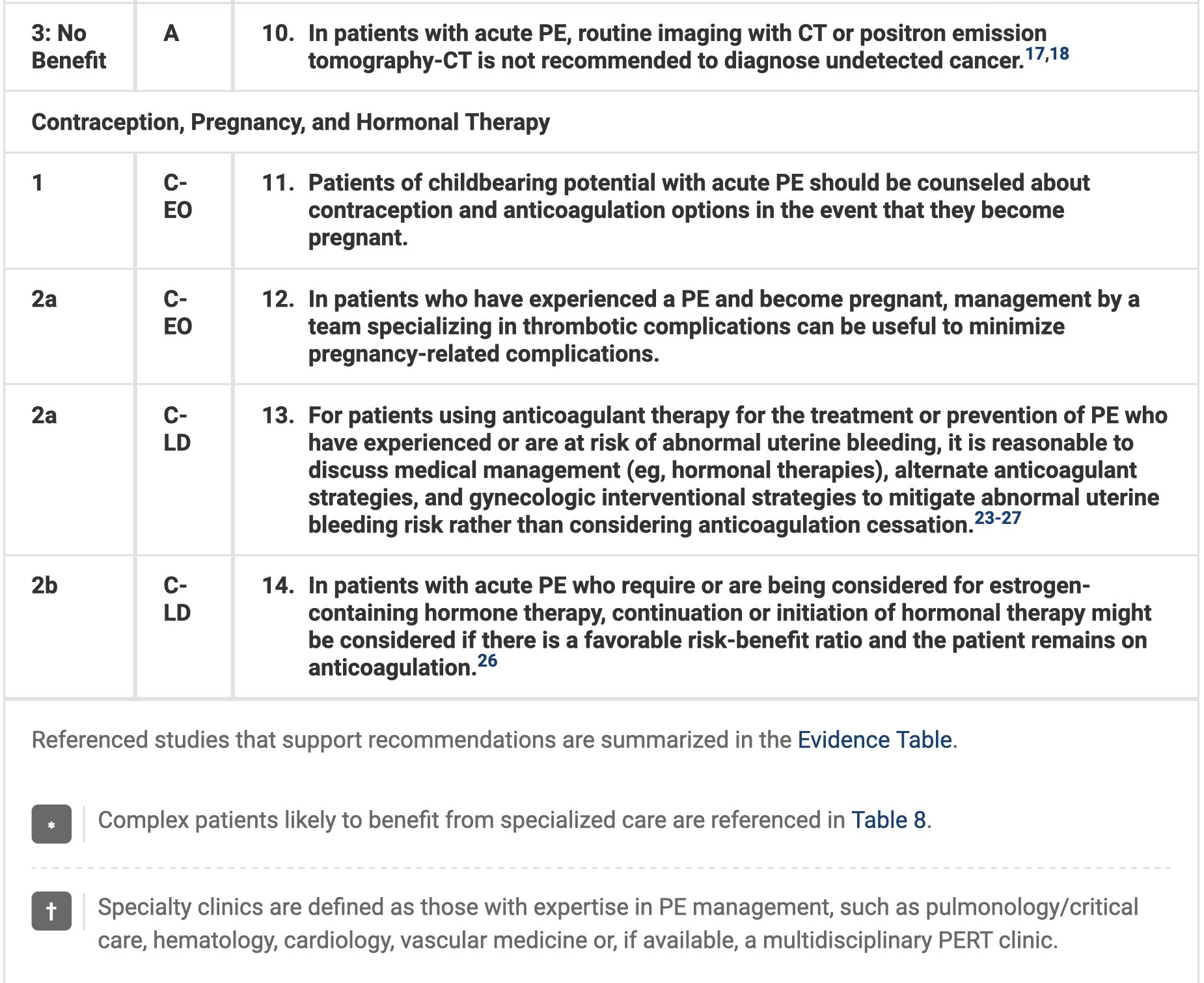
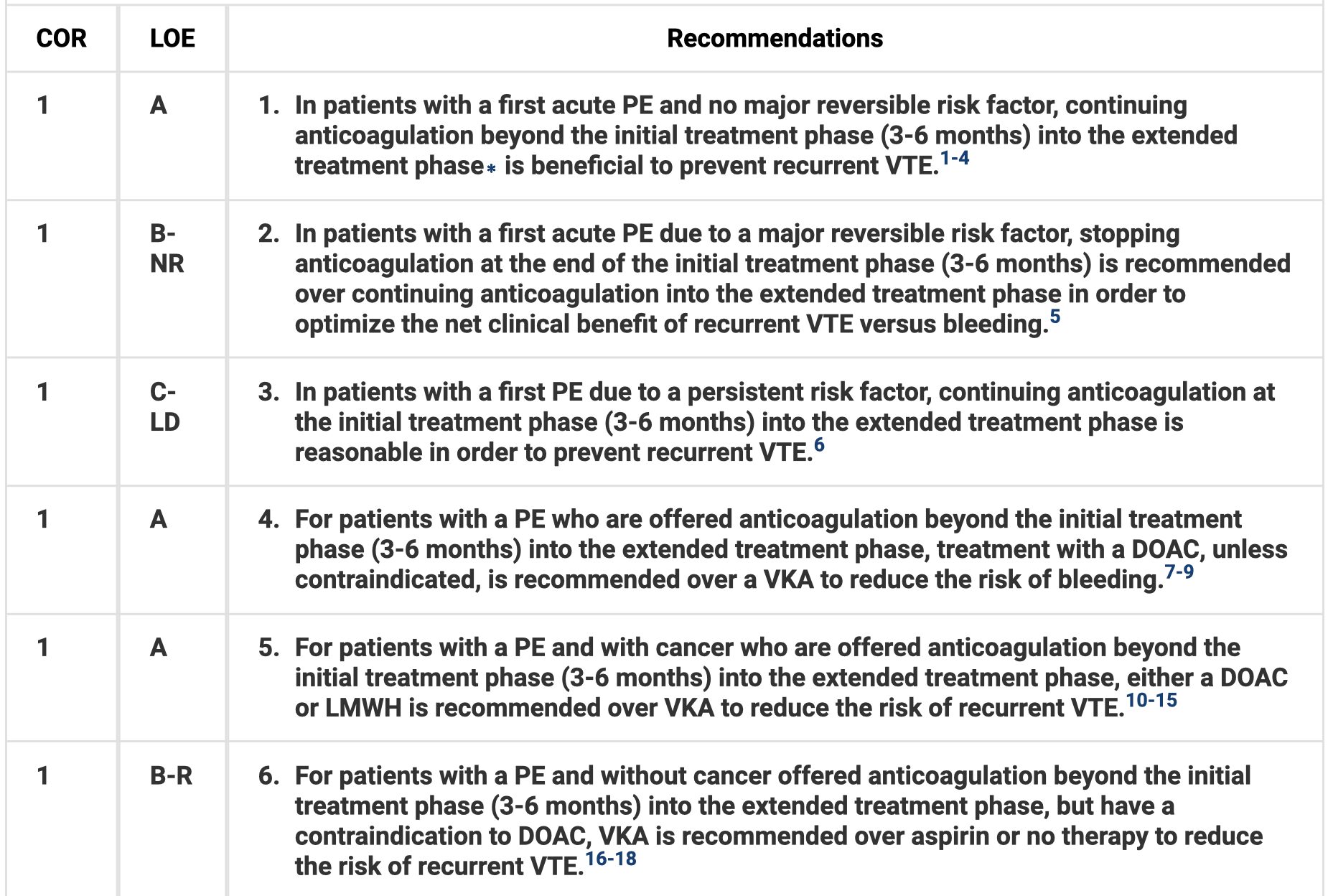
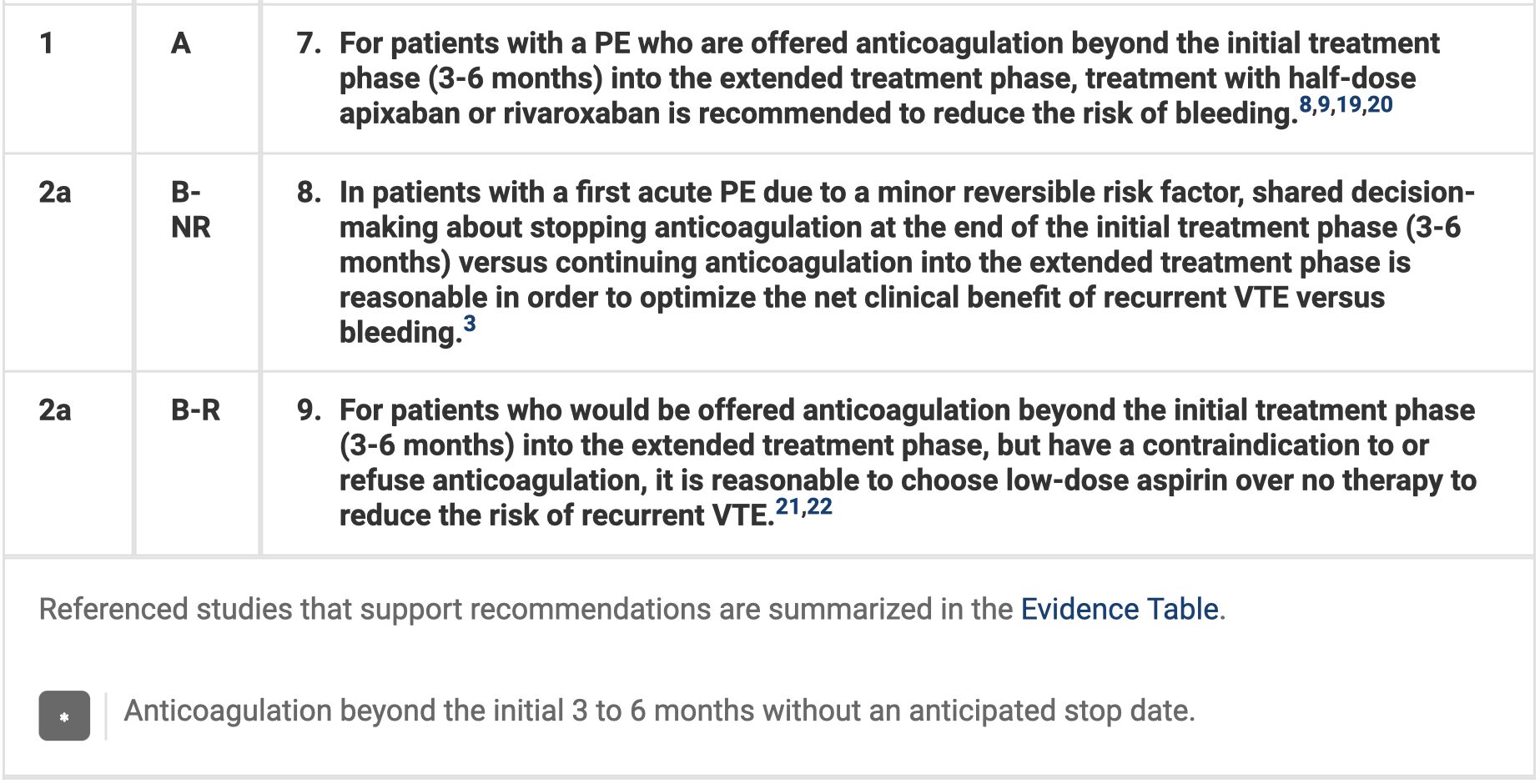
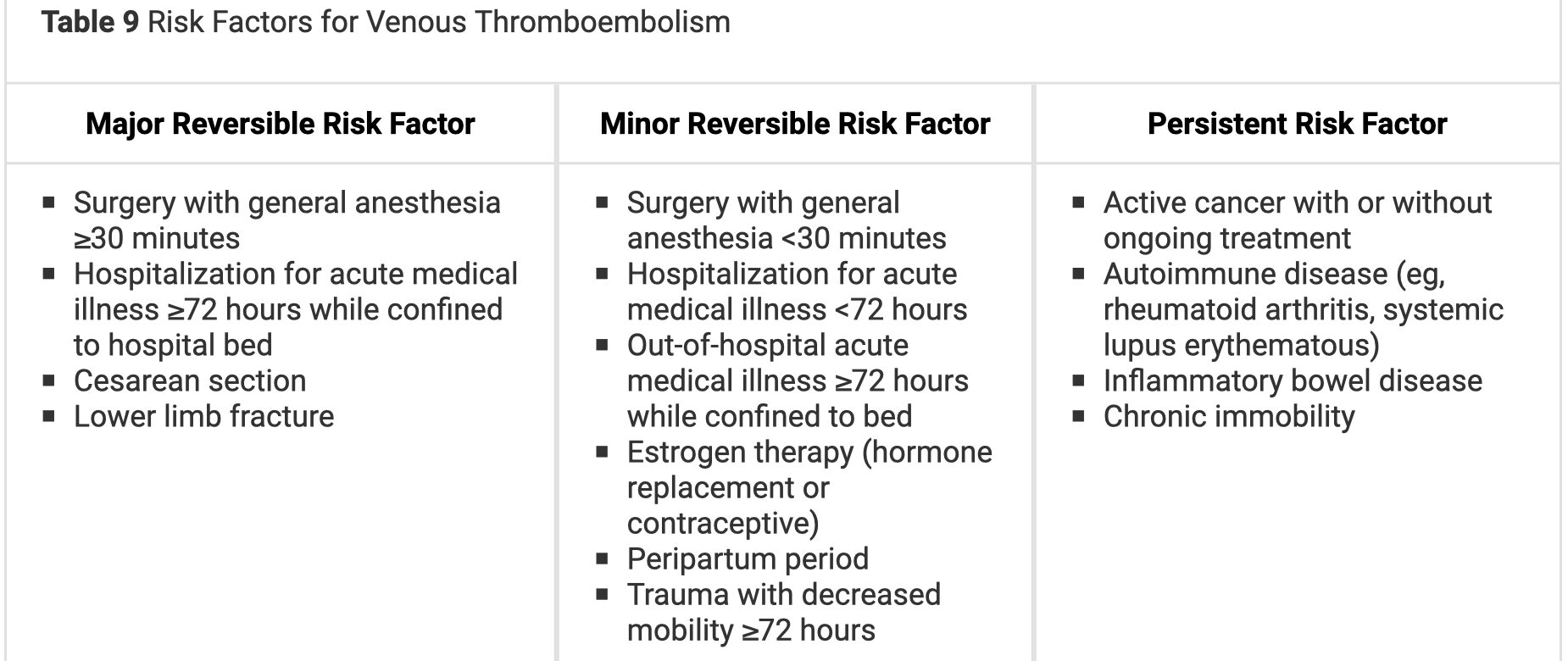
- For patients with first PE and no major reversible risk factor, continuing anticoagulation beyond the initial treatment phase (3-6 months) into an extended phase can help prevent recurrent PE. If those with a major reversible risk factor, stopping at the end of the initial treatment phase is recommended.
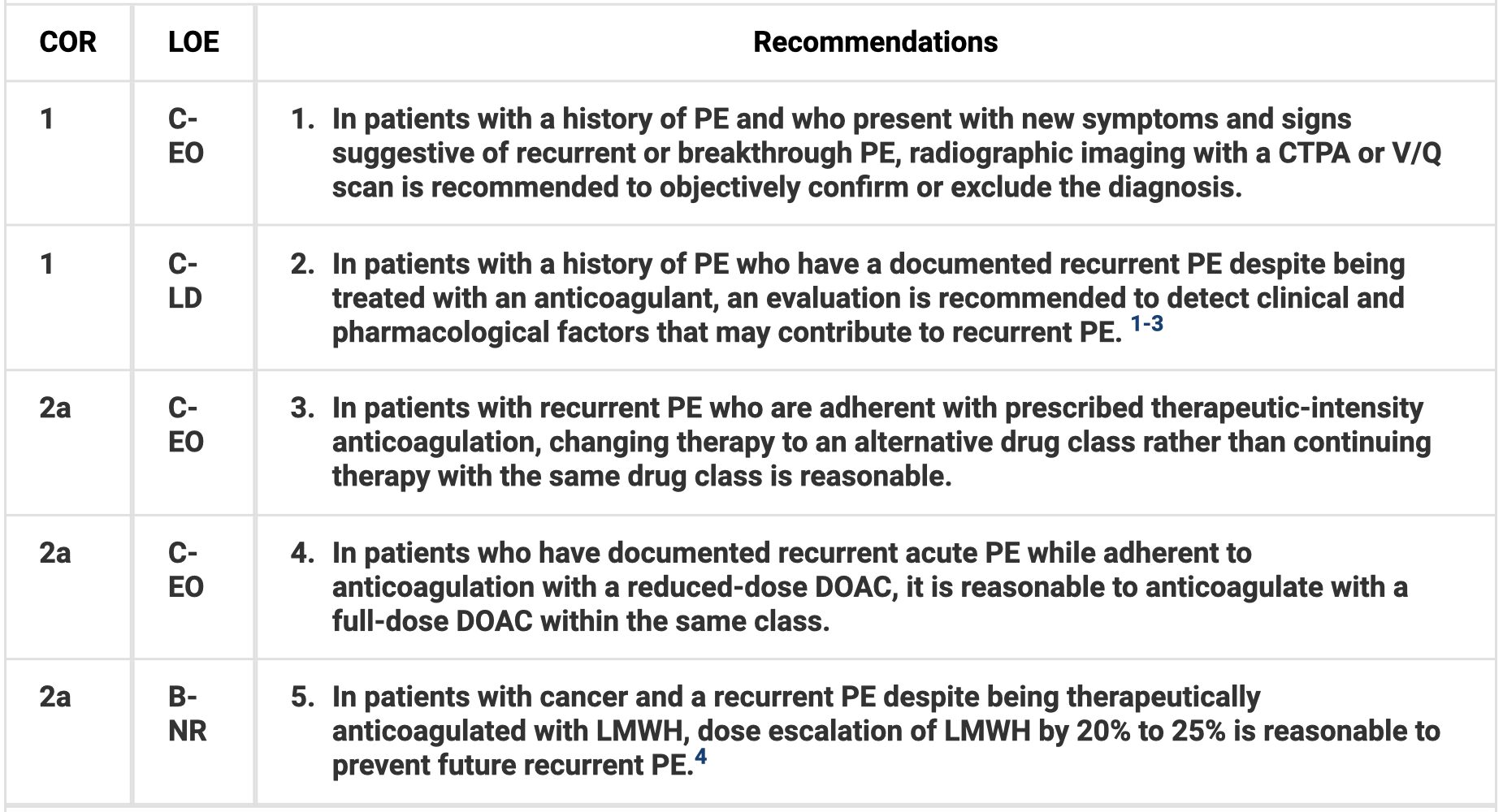
- In patients with history PE and new signs/symptoms of recurrent/breakthrough PE, imaging is recommended. If recurrent PE and adherent to prescribed therapeutic intensity anticoagulation, use an alternative drug class.
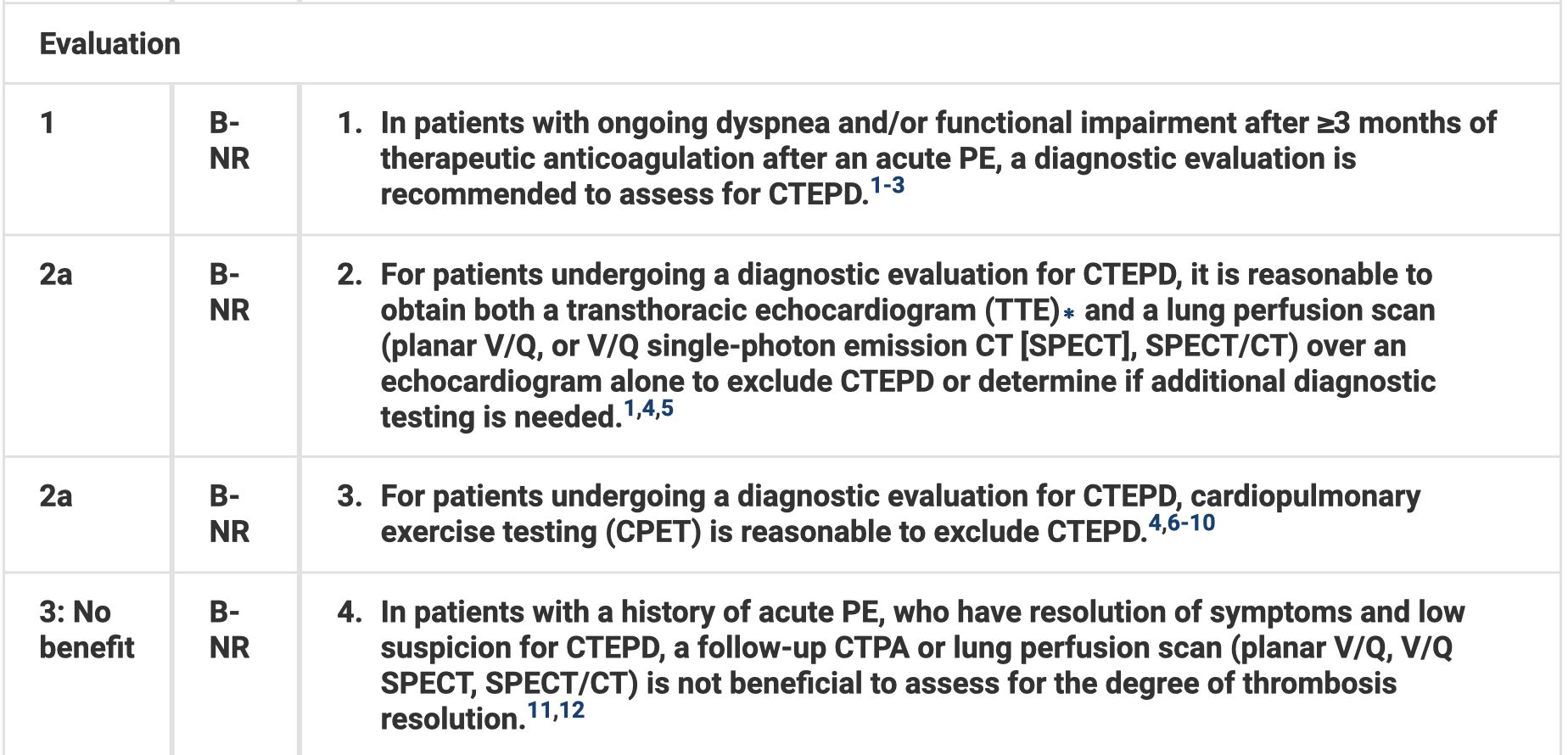
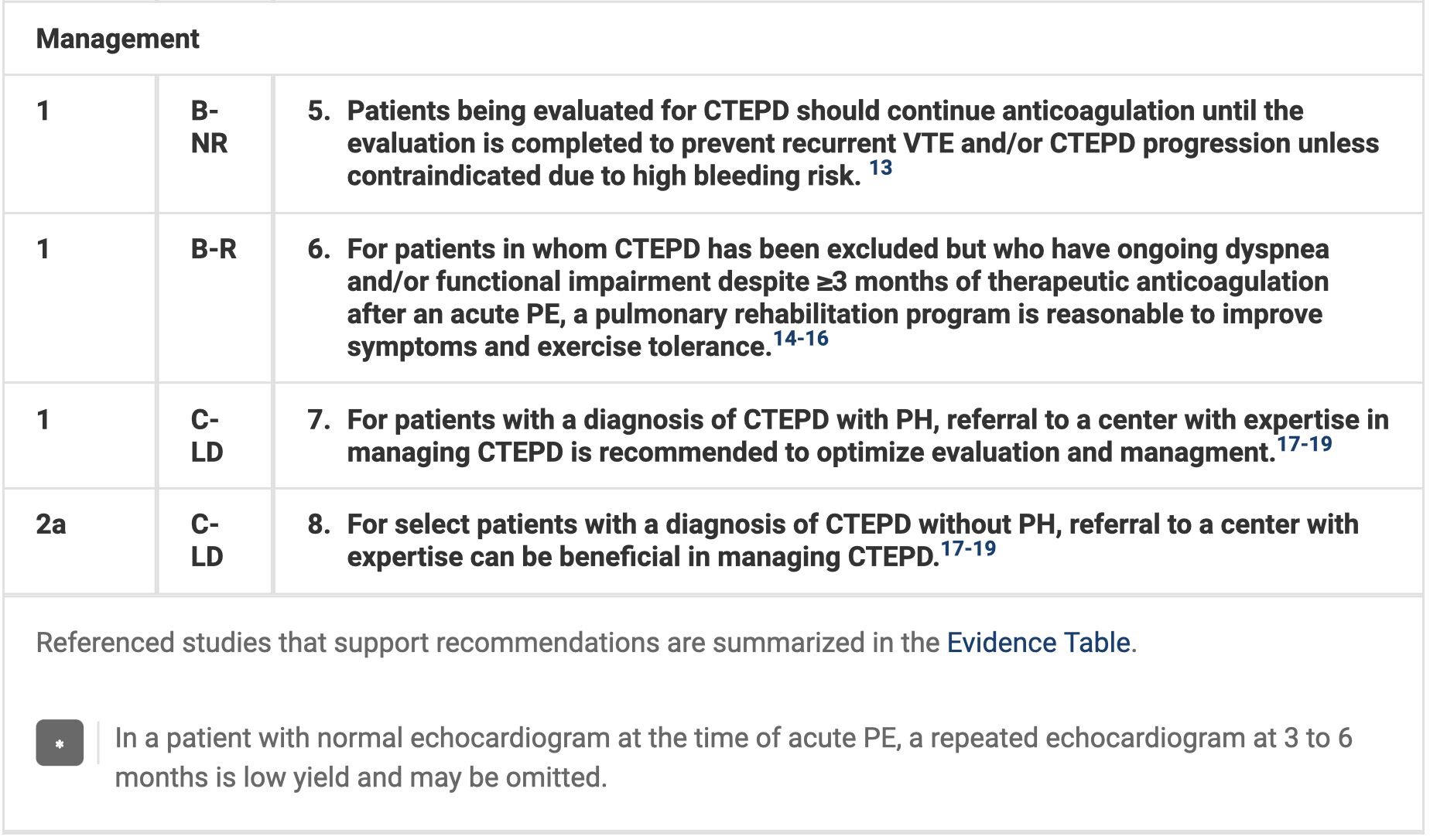
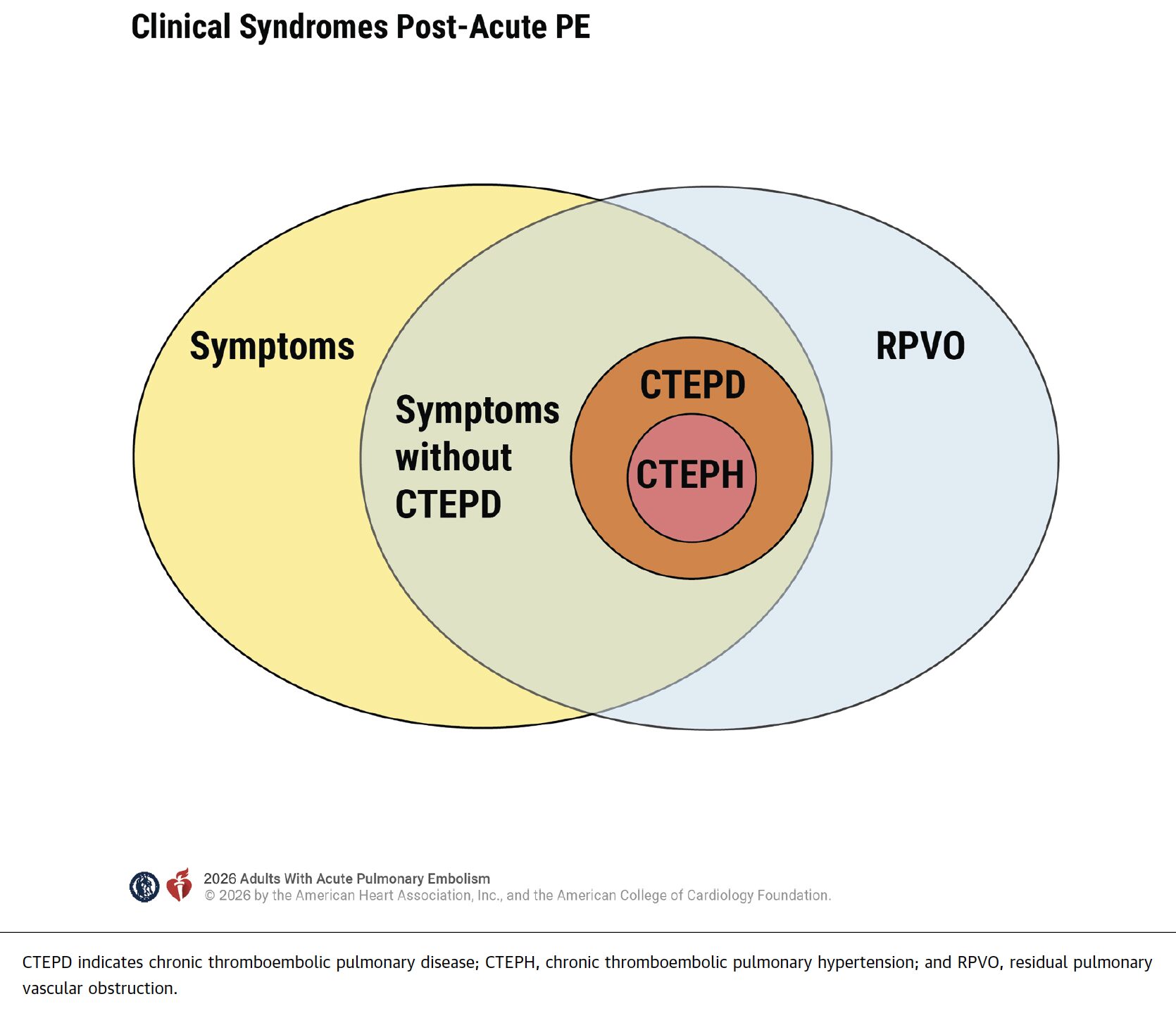
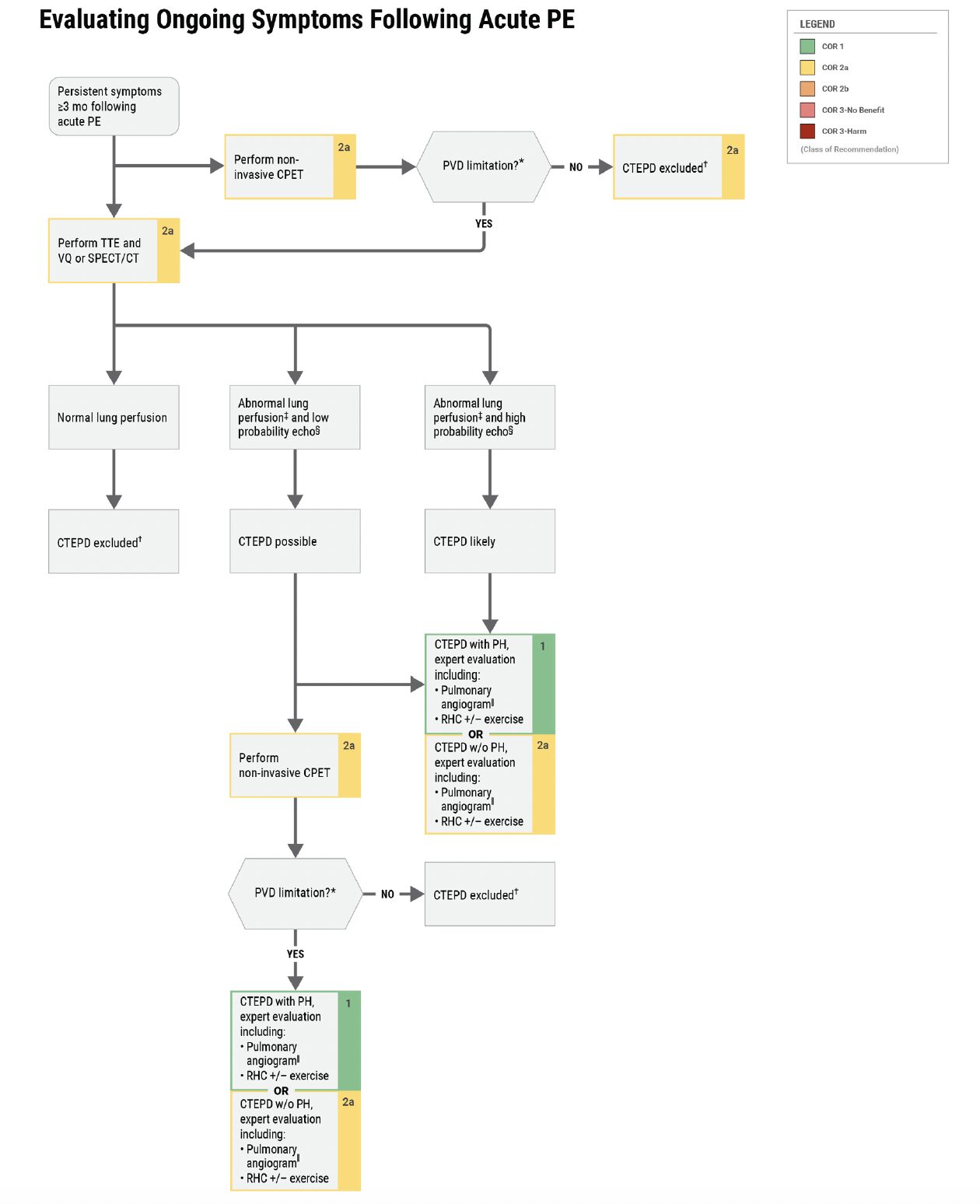
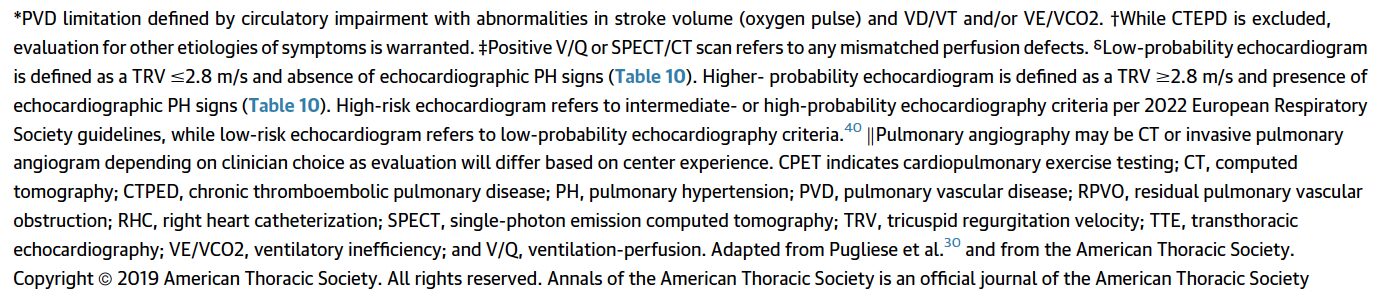
- For patients with ongoing dyspnea and/or functional impairment for at least 3 months of anticoagulation after acute PE, further evaluation for chronic thromboembolic pulmonary disease (CTEPD) is recommended.
Top Ten Messages from the Guidelines:
- A new clinical classification scheme is presented, entitled “Acute Pulmonary Embolism Clinical Categories,” with 5 categories (A-E) and subcategories, ranging from low to high risk for adverse outcomes, in order to enhance the precision of severity classification, prognosis assessment, and evidence-based therapeutic decision-making for patients presenting with acute PE.
- Patients with acute PE who are asymptomatic (AHA/ACC PE Category A) can safely be discharged home from the emergency room and do not need to be hospitalized.
- Early hospital discharge is generally recommended for patients with acute PE who are symptomatic but have a low clinical severity score (AHA/ACC PE Category B).
- Symptomatic patients with acute PE and an elevated clinical severity score, including those with elevated biomarkers and/or right ventricular dysfunction (AHA/ACC PE Category C), incipient cardiopulmonary failure (AHA/ACC PE Category D), and those with cardiopulmonary failure characterized by persistent hypotension (AHA/ACC PE Category E) should be hospitalized to optimize treatment strategies.
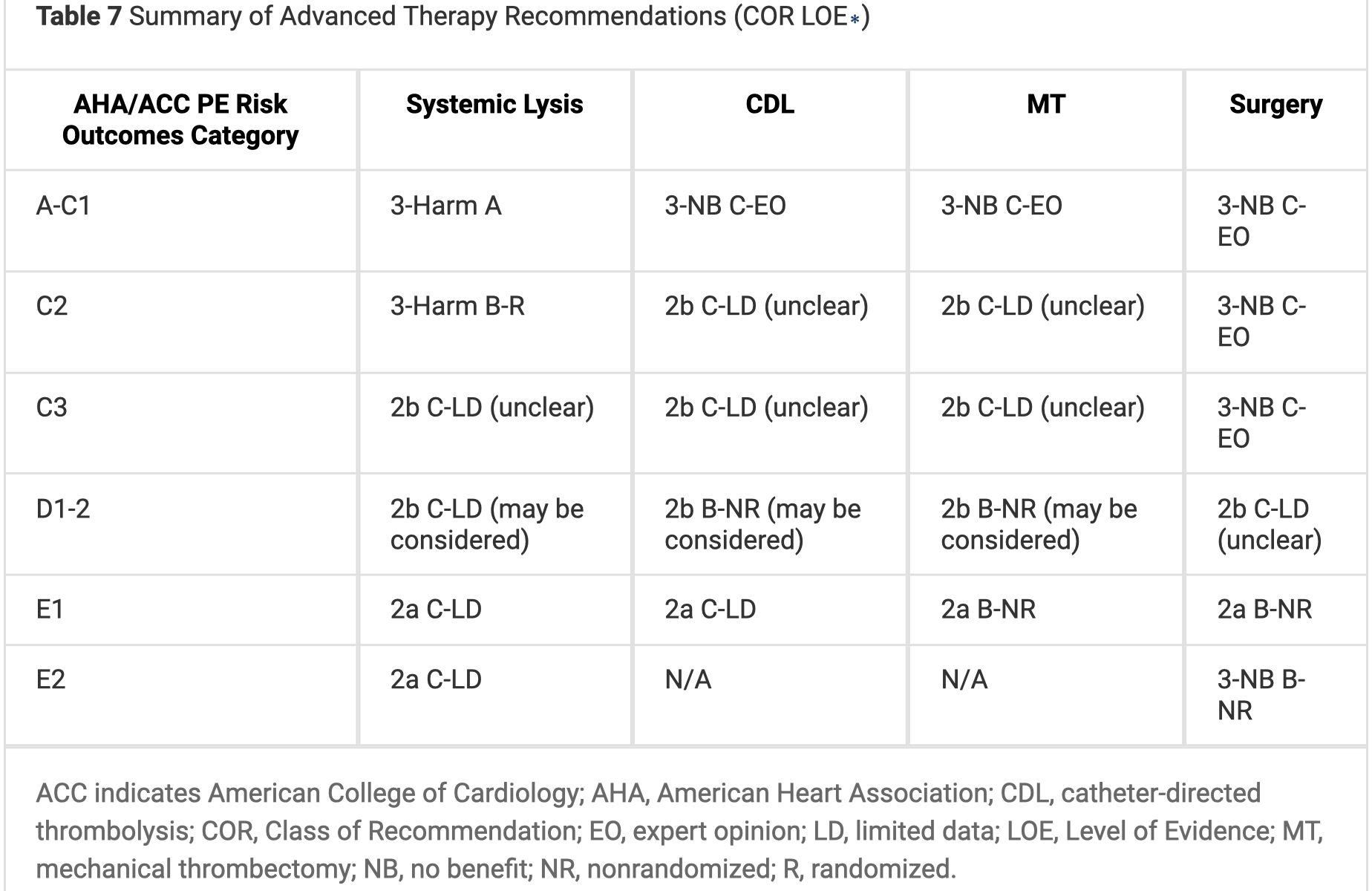
- Advanced therapies, including systemic thrombolysis, catheter-based thrombolysis, mechanical thrombectomy, and surgical embolectomy are reasonable for patients with acute PE in AHA/ACC PE Category E1 and can be considered for patients with acute PE in AHA/ACC PE Category D1-2.
- PE response teams (PERTs) are recommended to improve timeliness of care.
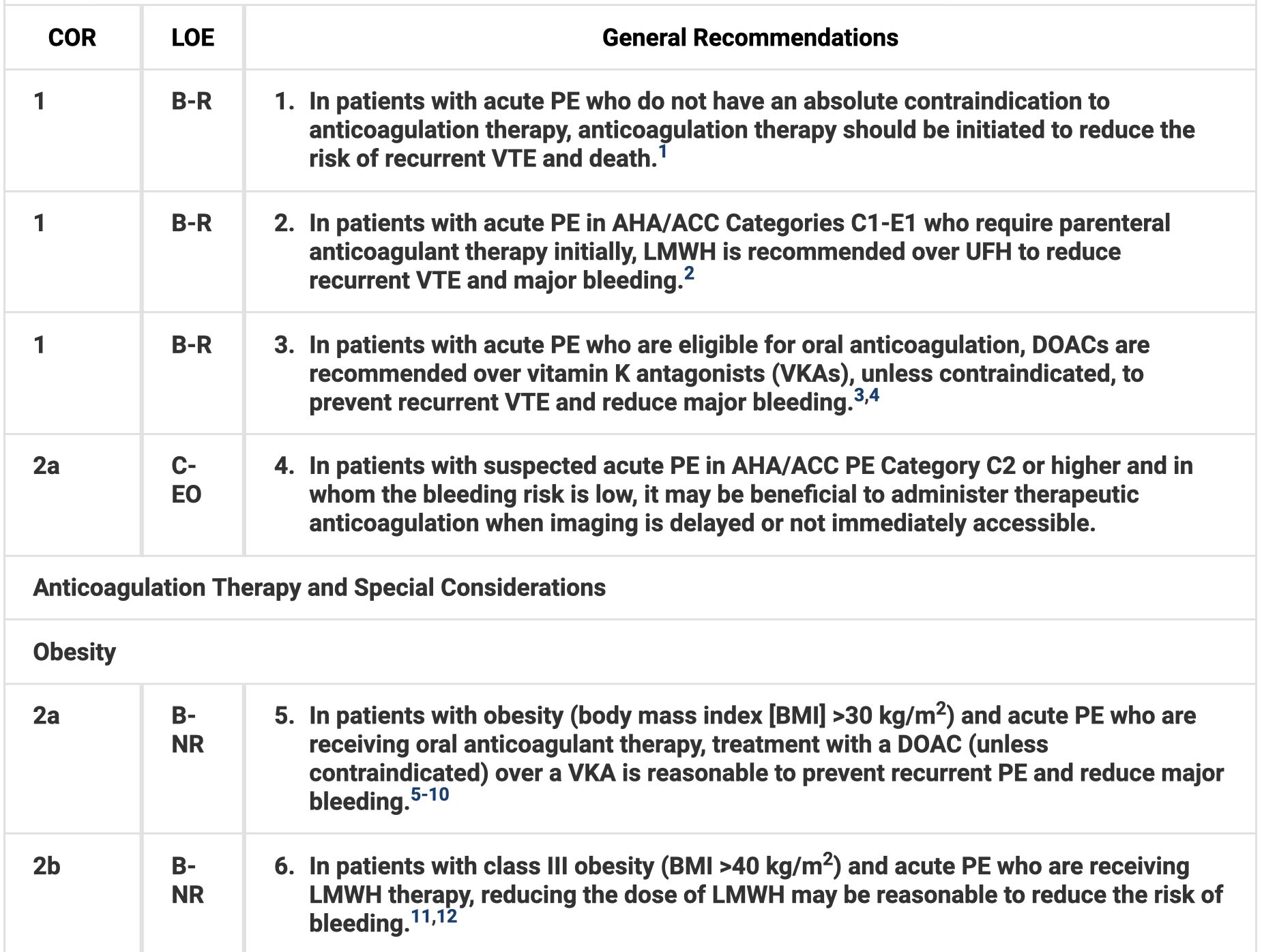
- In patients with acute PE who require initial parenteral anticoagulant therapy, low-molecular-weight heparin (LMWH) is recommended over unfractionated heparin (UFH).
- In patients with acute PE who are eligible for oral anticoagulation, direct oral anticoagulants (DOACs) are recommended over vitamin K antagonists (VKAs), unless contraindicated, to prevent recurrent venous thromboembolism (VTE) and reduce major bleeding.
- In patients with a first acute PE without a major reversible risk factor and in those with a persistent risk factor, continuing anticoagulation beyond the initial treatment phase (3-6 months) into the extended phase is recommended.
- Patients who have had acute PE should be asked about PE-related symptoms and functional limitations at every visit for at least 1 year to screen for chronic thromboembolic pulmonary disease (CTEPD) or other causes of dyspnea and functional limitation.
Evidence Grading:
All recommendations are designated with a class of recommendation (COR) and level of evidence (LOE). COR is the strength of the recommendation, while the LOE is the quality of scientific evidence.

The Guidelines…
Clinical Assessment
Diagnostic Testing

PE Outcomes Risk Stratification
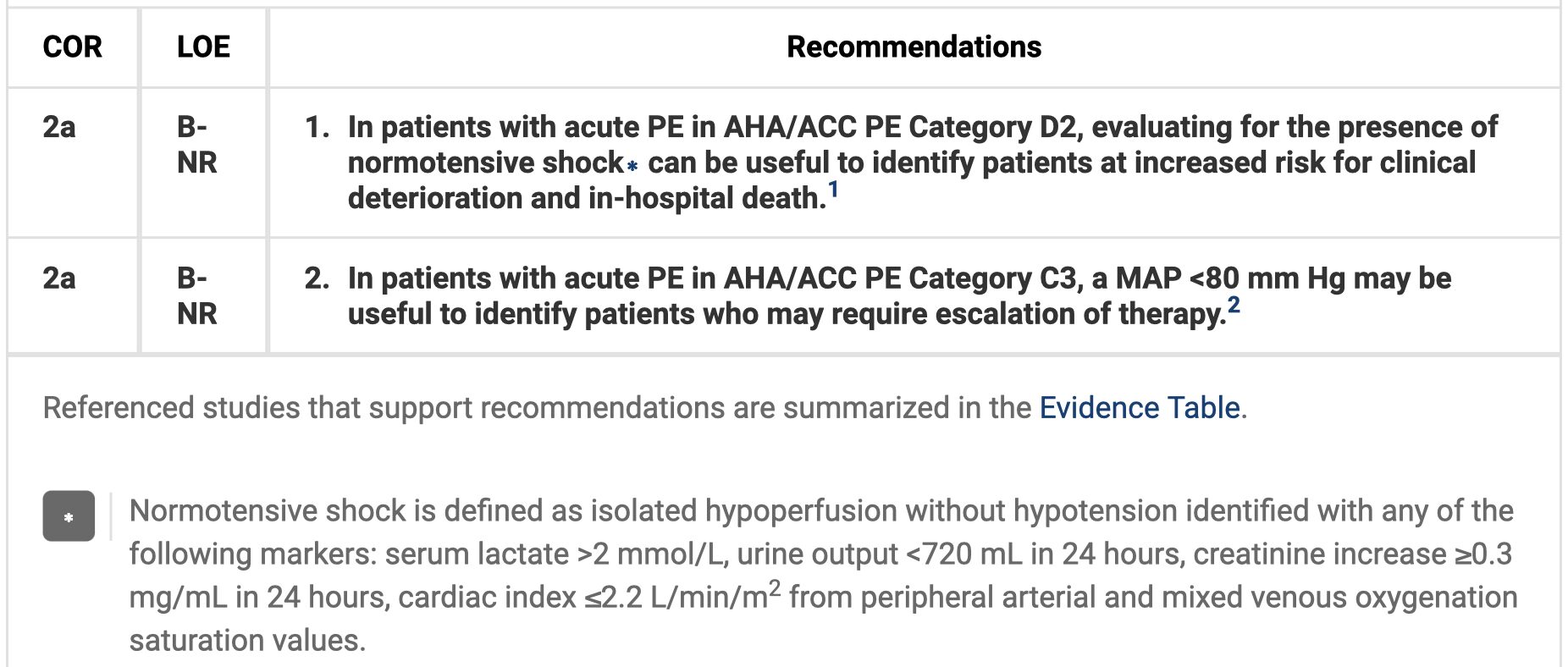
Hemodynamic Assessment
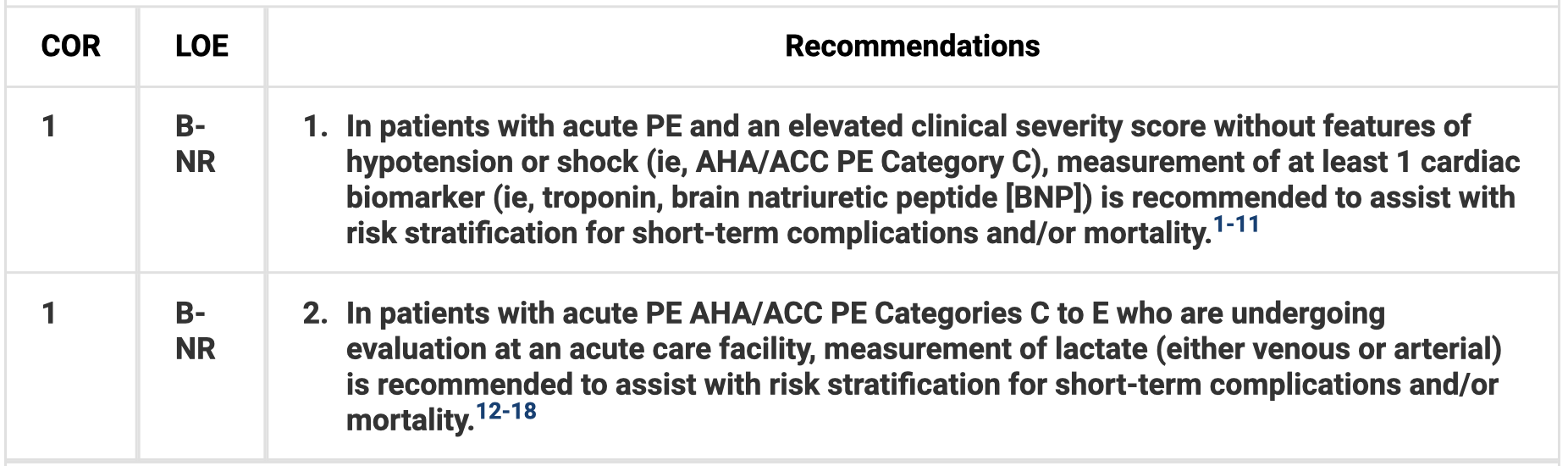
Biomarkers for Risk Stratification
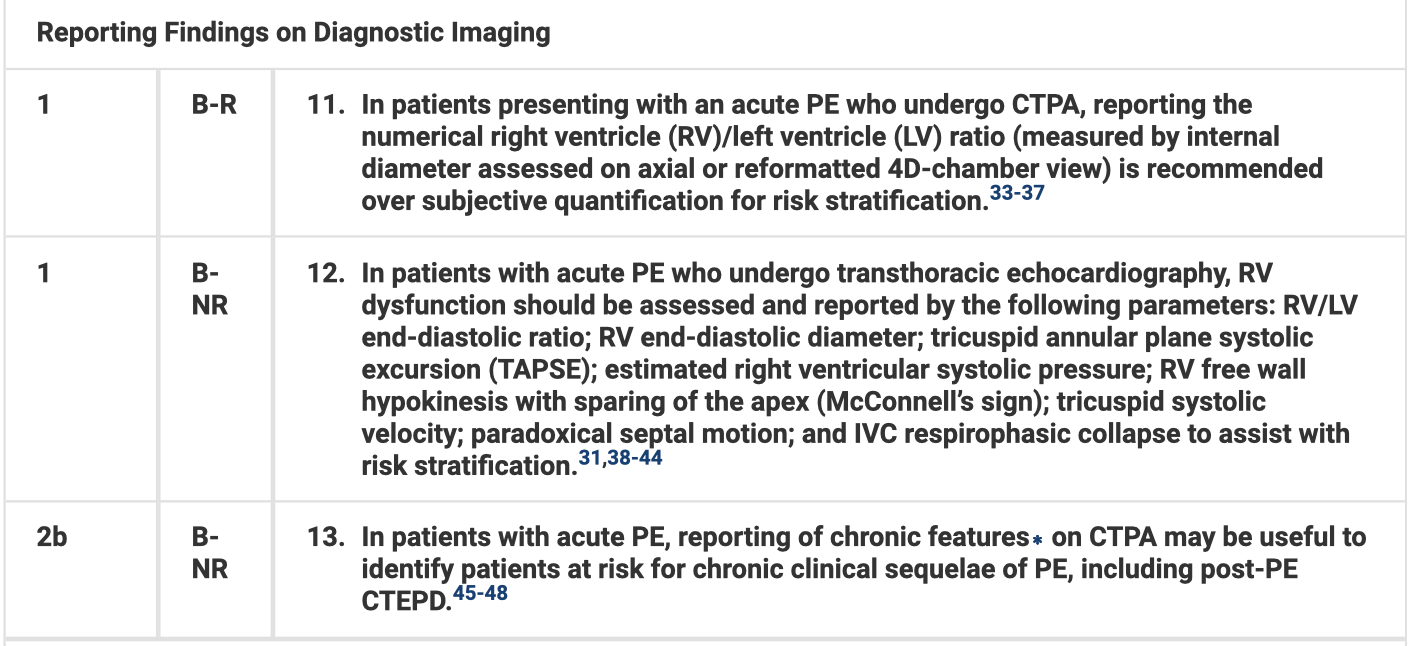
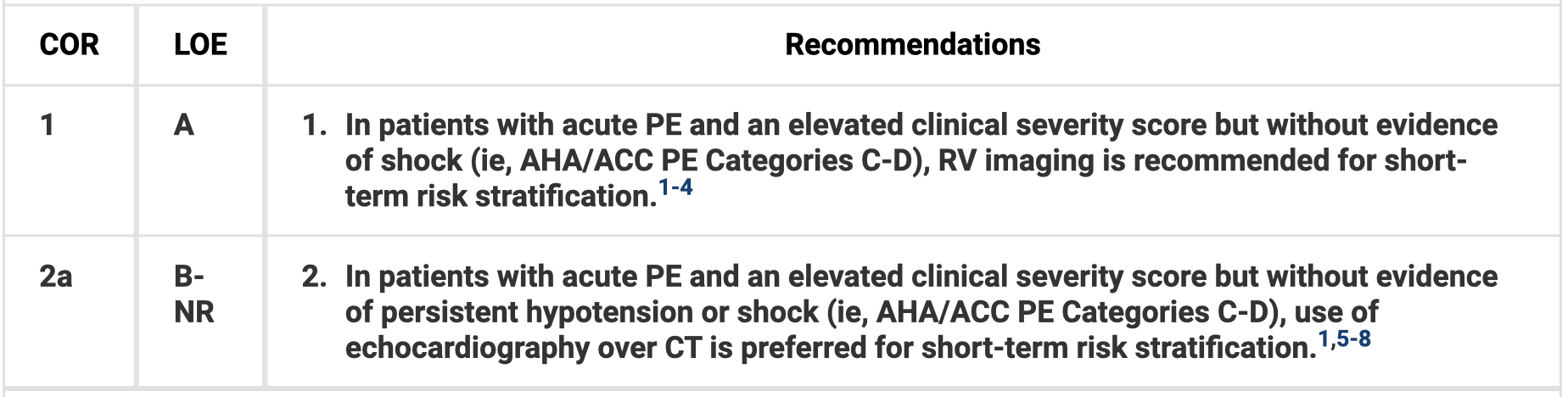
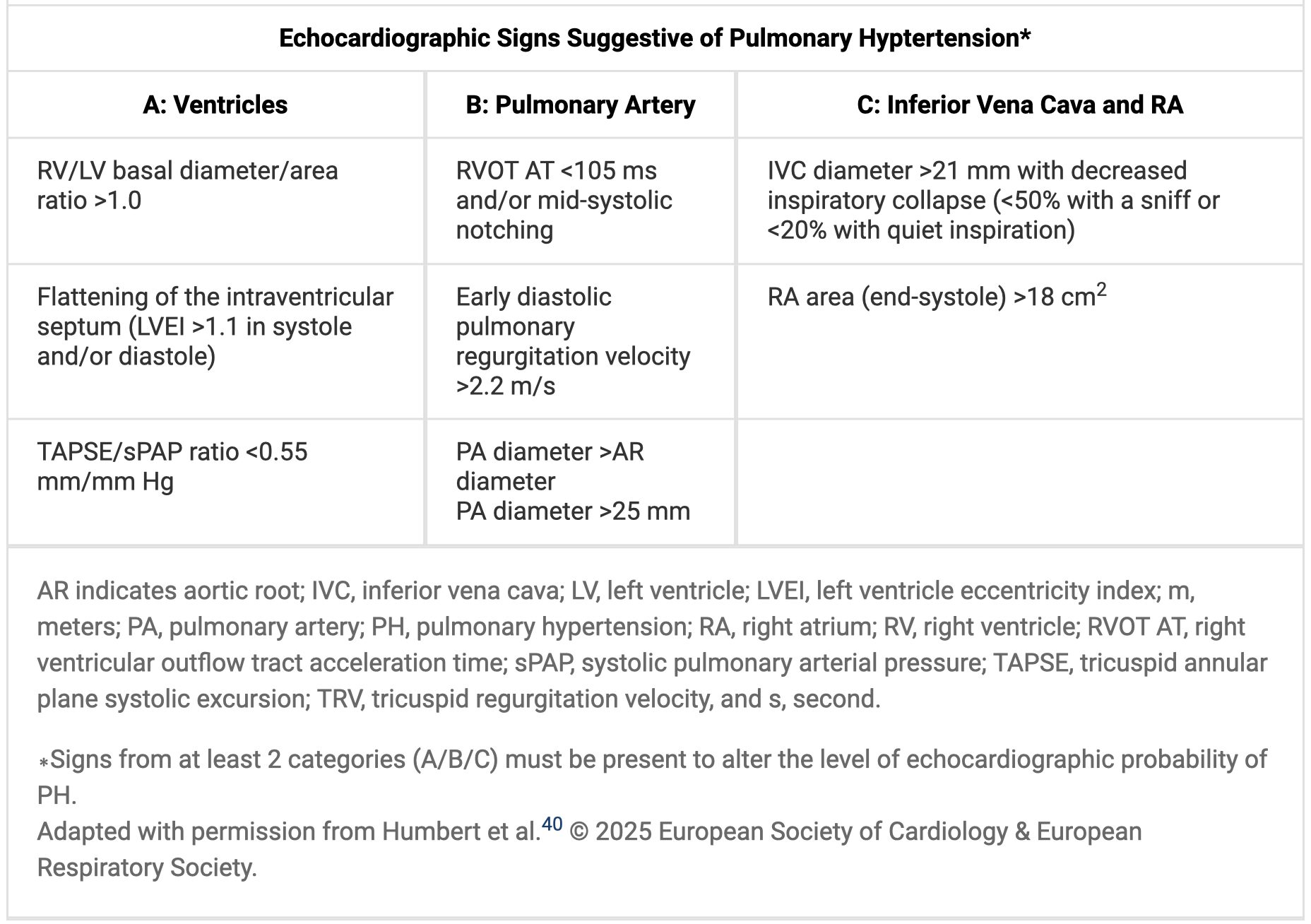
RV Imaging for Risk Stratification
Quantification of Thrombus Burden for Short-Term Risk Stratification

Acute Management
Suitability for Outpatient Management of PE
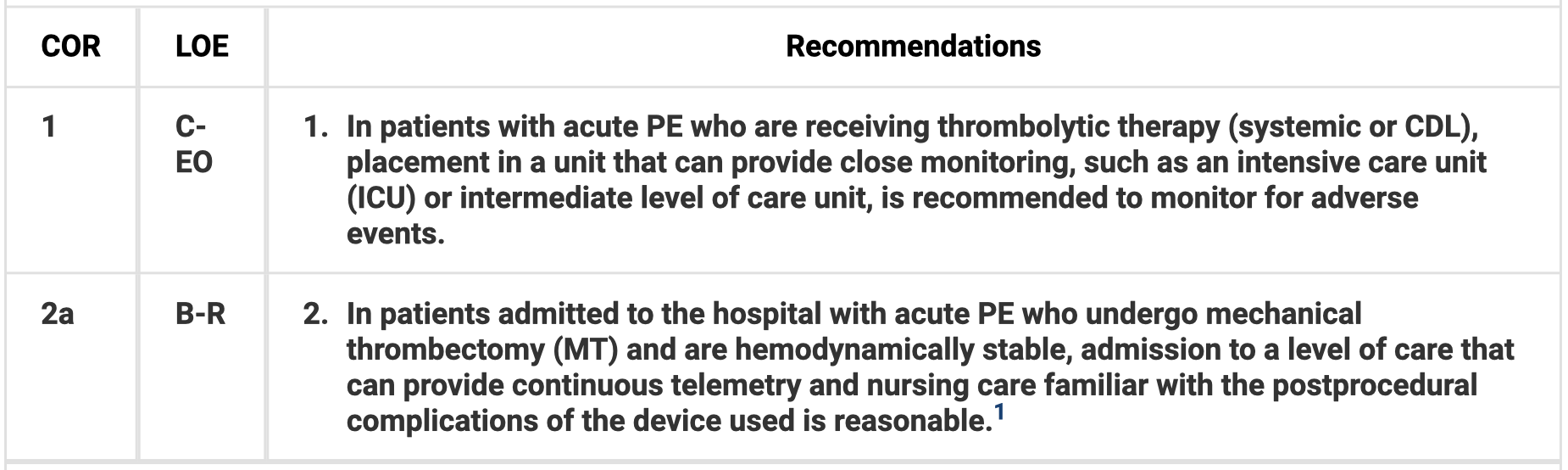
Admission
Interhospital Transfers

Pulmonary Embolism Response Team


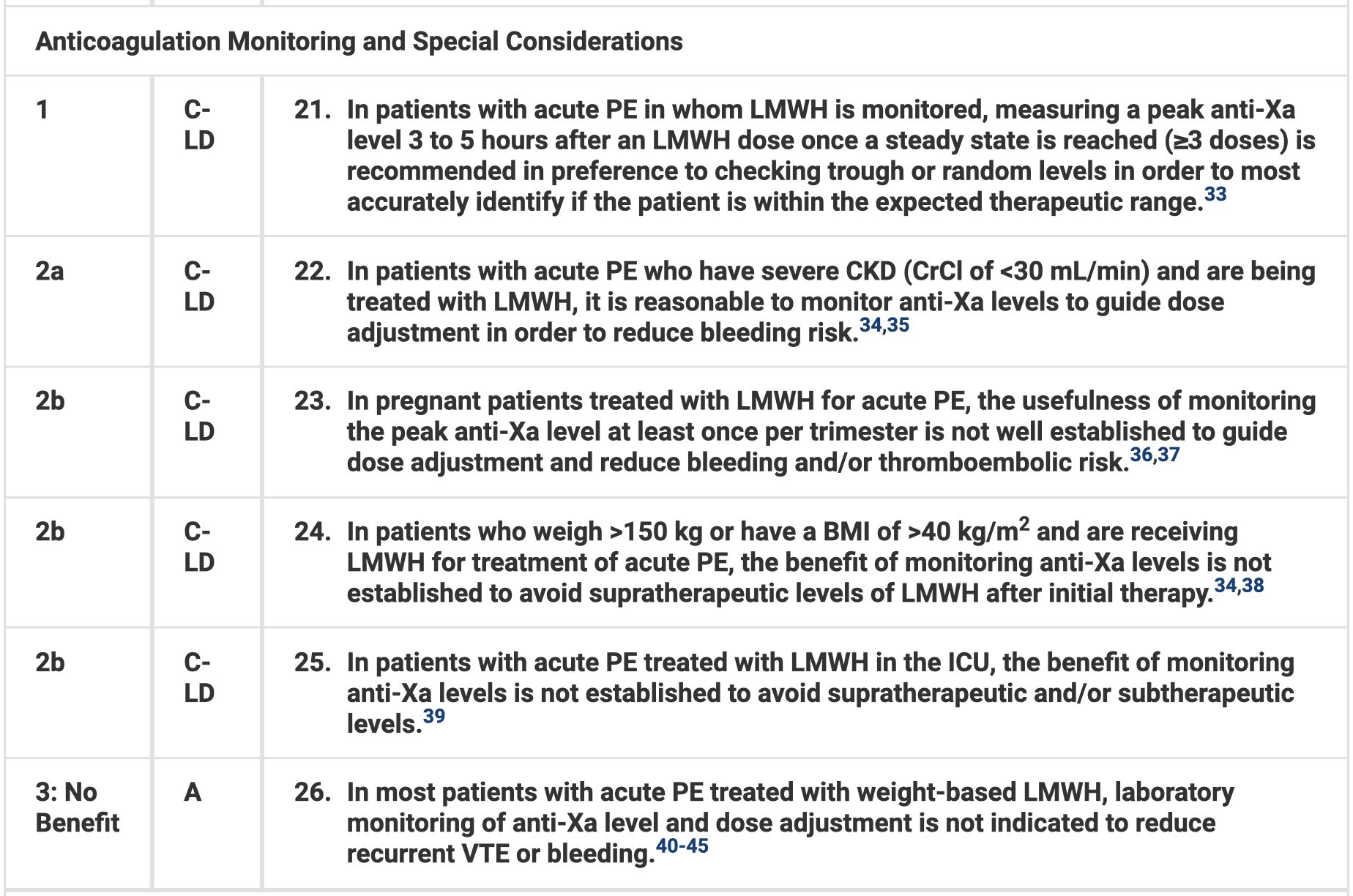
Anticoagulation Therapy
Hemodynamic Pharmacotherapy
Sedation and Ventilatory Strategies
Mechanical Circulatory Support
Role of the IVC Filter

Advanced Management
Systemic Thrombolysis
Catheter-Directed Thrombolysis
Mechanical Thrombectomy
Surgical Embolectomy
Monitoring and Follow-Up
Patient Activity and Travel
Anticoagulation Therapy for Recurrence Risk
Recurrent PE
Persistently Symptomatic Patients after PE
Evidence Gaps





