Retroperitoneal Hematoma in the Emergency Department
By Courtney Cassella MD
Resident Physician, Icahn School of Medicine at Mount Sinai
Edited by Stephen Alerhand MD and Alex Koyfman MD
Featured on #FOAMED REVIEW 36TH EDITION – Thank you to Michael Macias from emCurious (@EMedCurious) for the shout out!
Clinical Case
A 74 year-old woman with a past medical history of coronary artery disease, aortic stenosis with mechanical valve replacement, and diabetes, presents with right wrist and hip pain after a mechanical trip and fall at home. The patient reports her right leg gave out when she stood up from the couch. She endorses right leg numbness. She denies head trauma or loss of consciousness. She denies headache, lightheadedness, chest pain, shortness of breath, palpitations, nausea, or vomiting. Review of systems is positive for abdominal discomfort and constipation for 2 days.
Physical examination reveals an afebrile, tachycardic, alert and oriented woman in marked discomfort secondary to pain. The exam is notable for right lower quadrant tenderness, right wrist deformity and swelling, and decreased sensation to the right inner thigh.
Background
Retroperitoneal (RP) hematoma or hemorrhage is a rare but potentially life-threatening diagnosis. The presentation and symptoms can be subtle. One can think of RP hematomas in three categories: spontaneous, traumatic, and post-procedural.
For spontaneous hematomas, it is important to keep a high index of suspicion in patients with coagulopathies. In trauma, one must be cognizant of the clues in the trauma work-up and associated injuries of the retroperitoneal organs. There are case reports of RP hematoma after various procedures (ERCP, vaginal mesh), though classically it is a complication of endovascular and percutaneous procedures.
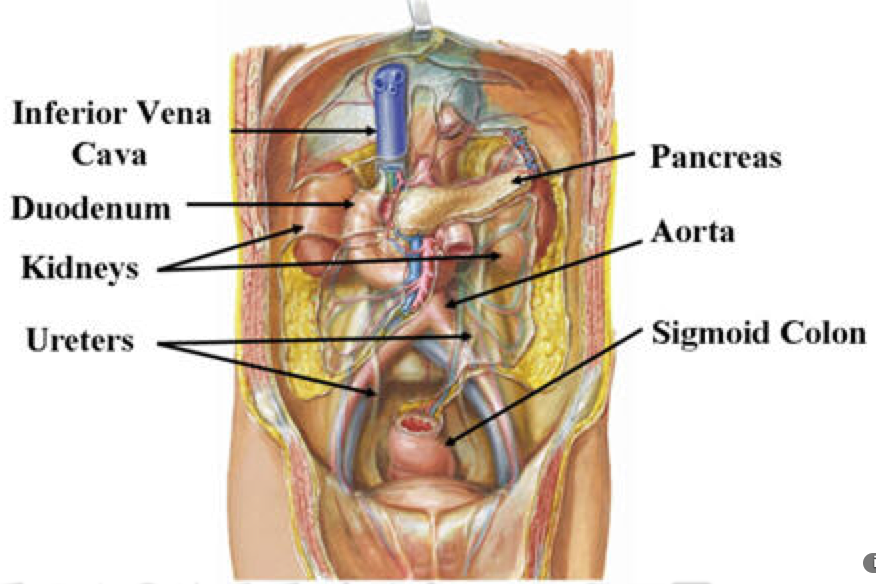
Retroperitoneal Organs (SAD PUCKER)
Suprarenal glands (adrenal glands)
Aorta and Inferior Vena Cava
Duodenum – second, third, and fourth segments
Pancreas – head, neck, and body
Ureters
Colon – ascending, descending
Kidneys
Esophagus
Rectum
Spontaneous Retroperitoneal Hematoma Risk Factors* 2,5,6
- Anticoagulation – increasing suspicion if also with antiplatelet drugs
- Acquired or congenital coagulopathies
- Aneurysm
- Chronic hemodialysis – secondary to the intermittent heparin bolus and platelet dysfunction
Traumatic Mechanisms and Associated Injuries 1,4
- Blunt (70-80%) versus penetrating (20-30%)1
- Avulsion of branches of the aorta, inferior vena cava, superior mesenteric artery
- Rupture of duodenum
- Direct blow with compression or shearing forces against the spine
- Closed loop blowout from deceleration
- Midline transection of the pancreas
- Contact with steering wheel or handlebars
- Rapid deceleration
- Renal contusion, fracture, avulsion, rupture
- Pelvic fracture
- Loss of blood from site of fracture
- Disruption of pelvic venous plexus
History and Physical Exam Findings 1,2,6
- Lenk or Wunderlich Triad
- Pain: Back, groin, flank, abdomen (most common presenting symptom)
- Palpable mass
- Shock
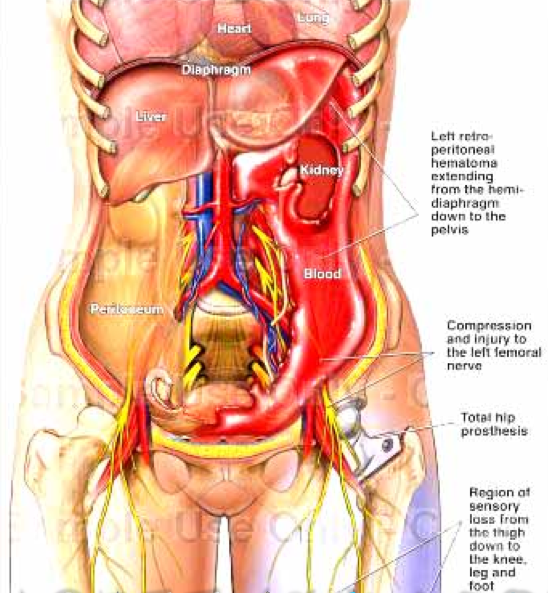
- Leg paresis and/or anterior thigh hypoesthesia
- Secondary to hematoma compressing the femoral nerve
- Cullen’s sign (periumbilical ecchymosis) – late finding
- Grey-Turner’s sign (ecchymosis of the flanks) – late finding
- *History of risk factors as above
Evaluation and Diagnosis 1,3,4,5
- Complete Blood Count for anemia
- Lipase – suggests pancreatic or duodenal injury
- Urinalysis for hematuria – helps point toward renal contusion, bladder injury, and urethral injury associated with pelvic fracture
- Abdominal CT, preferably at least with intravenous contrast to evaluate for extravasation

Treatment 1,2,5,6
- Conservative management
- Fluid resuscitation
- Blood transfusion
- Anticoagulant reversal
- Surgery and/or Interventional Radiology Consult
- Surgical decompression
- Percutaneous drainage
- Embolization
References/Further Reading
- Feliciano DV. “Management of traumatic retroperitoneal hematoma.” Ann Surg 1990; 211(1): 109-23.
- Gonzalez C, et al. “The clinical spectrum of retroperitoneal hematoma in anticoagulated patients.” Medicine (Baltimore) 2003; 82: 257-62.
- Melville SC, Melville DE. Chapter 25. Abdominal Trauma. In: Stone C, Humphries RL. CURRENT Diagnosis & Treatment Emergency Medicine, 7e. New York, NY: McGraw-Hill; 2011. http://eresources.library.mssm.edu:5371/content.aspx?bookid=385&Sectionid=40357240. Accessed February 11, 2015.
- Scalea TM, Boswell SA, Baron BJ, Ma O. Abdominal Trauma. In: Tintinalli JE, Stapczynski J, Ma O, Cline DM, Cydulka RK, Meckler GD, T. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. New York, NY: McGraw-Hill; 2011. http://eresources.library.mssm.edu:5359/content.aspx?bookid=693&Sectionid=45915613. Accessed January 28, 2015.
- Shah RD, et al. “Factors affecting the severity of spontaneous retroperitoneal hemorrhage in anticoagulated patients.” Am J Surg 2008; 195(3): 410-2.
- Sunga KL, et al. “Spontaneous retroperitoneal hematoma: Etiology, characteristics, management, and outcome.” J Emerg Med 2012; 43(2): e157-61.
- http://www.ncbi.nlm.nih.gov/pubmed/24972961




